

Ecthyma gangrenosum is a skin lesion usually produced by Pseudomonas aeruginosa, resulting from infection of a hair follicle or from systemic infection usually in immunocompromised patients.1 It is a rare disease with high rate of morbidity and mortality. The lesions begin as erythematous macules, which later develop into haematic papules or vesicles that rupture, thus producing necrotic ulcers. An early diagnosis and antibiotic treatment are essential to improve the prognosis of the disease. Here we present a case of a renal transplant patient on dual immunosuppressive therapy, who had ecthyma gangrenosum caused by P. aeruginosa, 3 years after the renal transplant, with a good response to antibiotic treatment.
This case involves a 63-year-old female patient, with hypertension, type 2 diabetes and a kidney transplant from a cadaver donor 3 years earlier; she attended the emergency room for a two day history of generalised skin lesions, fever and sore throat. Relevant history included a post-transplant intestinal ischaemia resolved with intestinal resection. She is currently being treated with mycophenolate mofetil (MMF) and tacrolimus.
On arrival she had a temperature of 38°C, blood pressure of 126/75mmHg and heart rate of 81bpm. On physical examination there were painful vesicular-bullous skin lesions of haemorrhagic content on the right leg, abdomen and left arm, about 3–25mm in diameter, and punctate erythematous lesions on the nasolabial folds and tongue blisters, and on the oral mucosa (Fig. 1). The laboratory tests showed haemoglobin 11.3g/dL, platelets 210,000, leukocytes 1780 (neutrophils 11.2%, lymphocytes 23% and monocytes 60.7%), glucose 140mg/dL, creatinine 1.95mg/dL (baseline 1mg/dL), urea 93mg/dL, potassium 3.31mEq/L, procalcitonin 1.1ng/ml, CRP 6.30mg/dL, pH in venous blood gases 7.39, l-lactate 2mmol/l. In the preceding days she had received empirical antibiotic therapy with amoxicillin-clavulanic acid for a sore throat.
 and on the back of the leg (B), corresponding to ecthyma gangrenosum.")
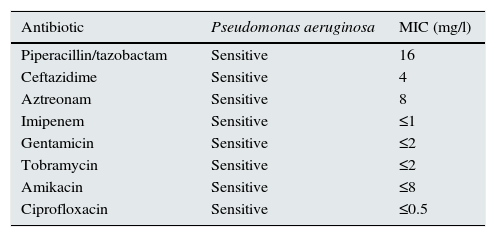
Suspecting ecthyma gangrenosum, the patient was admitted and placed on broad-spectrum antibiotics (daptomycin, ceftazidime and Meropenem®) after obtaining blood cultures, a wound culture and a biopsy of the lesion in Dermatology. Also, immunosuppression was reduced with a temporary suspension of MMF. During admission, the patient progressed favourably, and the skin lesion cultures were positive for P. aeruginosa; the daptomycin was stopped after determining sensitivity by an antibiogram (Table 1). In addition to antibiotic therapy, one of the bullous lesions was drained, and copper sulfate and silver sulfadiazine were applied topically. After 7 days of treatment, the lesions improved and the lab test results normalised (Cr 0.79mg/dL and leukocytes 3,000μ/l), and so the patient was discharged. In follow-up, and after completing 3 weeks of antibiotic therapy, the patient's symptoms resolved completely.
Antibiograms of wound exudate.
| Antibiotic | Pseudomonas aeruginosa | MIC (mg/l) |
|---|---|---|
| Piperacillin/tazobactam | Sensitive | 16 |
| Ceftazidime | Sensitive | 4 |
| Aztreonam | Sensitive | 8 |
| Imipenem | Sensitive | ≤1 |
| Gentamicin | Sensitive | ≤2 |
| Tobramycin | Sensitive | ≤2 |
| Amikacin | Sensitive | ≤8 |
| Ciprofloxacin | Sensitive | ≤0.5 |
MIC: minimum inhibitory concentration.
We therefore report here an exceptional case of ecthyma gangrenosum in a patient with a renal graft that functioned for 3 years, with a positive outcome after treatment, despite the initial condition of neutropenia and immunosuppression.
There are few data on ecthyma gangrenosum published to date, with the majority of them concerning patients with haematological diseases in paediatric or immunosuppressed patients.2,3 As for kidney transplant patients, 3 cases have been reported so far.4–6 In all 3 cases the outcome has been favourable, after targeted antibiotic treatment, whether or not combined with debridement of the lesions,. In one of these cases the initial evolution was torpid, with septic shock, and required admission to the intensive care unit and repeated surgical debridement. The patient improved thereafter.5 Therefore it seems that starting treatment early with broad-spectrum antibiotics (which especially covers P. aeruginosa) when these lesions are suspected, as well as granulocyte-colony stimulating factor and surgery if necessary, affects how the condition, which is potentially fatal, develops.7
An association between neutropenia and increased mortality has been documented in patients with ecthyma gangrenosum, with neutropenia being one of the main factors for poor prognosis.8 In a series of 43 cases of immunocompetent paediatric patients who developed sepsis due to P. aeruginosa, 9 out of 10 patients who died had presented with leukopenia at the onset of symptoms.9 It is noteworthy that in reviewing cases in the immunocompetent general population, the evolution of the disease is more torpid, with increased mortality in patients with a renal transplant on immunosuppressive therapy.7
In conclusion, the clinical suspicion of ecthyma gangrenosum in patients with a renal transplant and suggestive lesions requires an initial aggressive approach with broad-spectrum antibiotics, granulocyte-colony stimulating factor and surgical debridement, if necessary, in order to avoid major life-threatening complications.
FundingThe authors declare that they have not received any funding to complete this study.
Please cite this article as: Santos B, Sanz M, Nuñez A, Mayor LO, Quiroga B. Ectima gangrenoso en paciente portadora de trasplante renal. Nefrologia. 2016;36:573–574.



