
Hypernatremia secondary to the use of hypertonic saline solution (HSS) as a scolicidal agent in hydatid cyst surgery is a complication that is very uncommon but extremely serious as it can cause irreversible neurological complications.1
We report a case of severe acute hypernatremia following hydatid cyst surgery. The patient was a 60-year-old woman who had no prior medical history and lived in an urban setting. She sought care for abdominal discomfort in the right hypochondrium during the past year. Abdominal ultrasound imaging revealed a cyst consistent with a hydatid cyst measuring 20 cm in diameter, category CE1–CE2 according to the World Health Organization classification;2 in addition, Echinococcus granulosus serology was positive. She was diagnosed with hepatic hydatid disease. A decision was made to administer treatment with albendazole for four weeks and perform a partial cystectomy/pericystectomy.
A laparotomy was done with local opening of the cyst, as well as protection of the abdominal wall and peritoneum with plastic material; a total of 2500 cc of cyst contents were aspirated. During cyst puncture, the patient presented sudden arterial hypotension and bradycardia that responded to epinephrine, methylprednisolone and dexchlorpheniramine. Thereafter, 3% HSS was twice instilled in the cyst cavity up to full repletion; each time, the HSS was left in place for 15 min and then a total of 5 l of contents were aspirated. An estimated 1000 cc of bleeding occurred. During surgery, a total of 1000 cc of 0.9% normal saline and 600 cc of packed red blood cells were administered. After that, the patient showed a tendency towards arterial hypotension, requiring norepinephrine as a continuous infusion. When the procedure was complete, marked hypernatremia was seen with Na+ 182 mmol/l (plasma osmolarity 378 mOsm/kg).
In the first 24 h, 2000 cc of 5% glucose in saline were administered. The patient also presented acute liver failure, development of anaemia, hyperfibrinolysis and disseminated intravascular coagulation with a blood deficit due to drainage of 1500 cc, requiring transfusion of red blood cells, platelets and fresh frozen plasma, for a total volume of 1650 cc. She presented diuresis of 680 cc. A CT scan of the head showed no acute abnormalities.
After 24 h, her sodium level dropped to 171 mOsm/l (plasma osmolarity 361 mOsm/kg), her blood glucose level was 445 mg/dl and acute kidney failure (AKF) was seen with a creatinine level of 2.22 mg/dl and diuresis of 180 cc. The patient was administered 1800 cc of 5% glucose in saline, furosemide infusion was started at a rate of 20 mg/h for 24 h and insulin infusion was initiated.
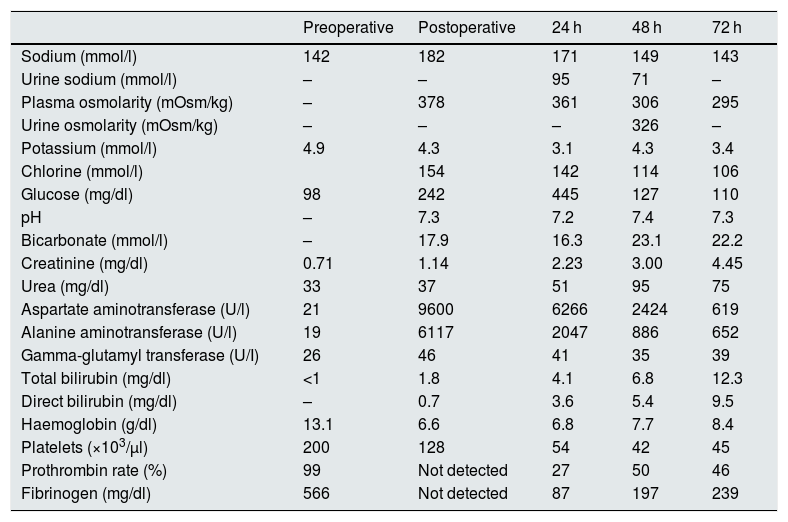
After 72 h, her hypernatremia had been corrected, so infusion of 5% glucose in saline was suspended and parenteral nutrition was started. The patient’s haemodynamic status remained poor. She was dependent on invasive mechanical ventilation and norepinephrine infusion. In addition, she had oligoanuria with a creatinine level of 4.45 mg/dl. She required continuous venovenous hemodiafiltration (CVVHDF) for two weeks; subsequently, negative balances were achieved with a diuretic, and after that spontaneous diuresis was achieved and full kidney function was recovered. On hospital discharge, she exhibited no neurological or other sequelae. Table 1 shows the patient’s laboratory values of note.
Laboratory parameters.
| Preoperative | Postoperative | 24 h | 48 h | 72 h | |
|---|---|---|---|---|---|
| Sodium (mmol/l) | 142 | 182 | 171 | 149 | 143 |
| Urine sodium (mmol/l) | – | – | 95 | 71 | – |
| Plasma osmolarity (mOsm/kg) | – | 378 | 361 | 306 | 295 |
| Urine osmolarity (mOsm/kg) | – | – | – | 326 | – |
| Potassium (mmol/l) | 4.9 | 4.3 | 3.1 | 4.3 | 3.4 |
| Chlorine (mmol/l) | 154 | 142 | 114 | 106 | |
| Glucose (mg/dl) | 98 | 242 | 445 | 127 | 110 |
| pH | – | 7.3 | 7.2 | 7.4 | 7.3 |
| Bicarbonate (mmol/l) | – | 17.9 | 16.3 | 23.1 | 22.2 |
| Creatinine (mg/dl) | 0.71 | 1.14 | 2.23 | 3.00 | 4.45 |
| Urea (mg/dl) | 33 | 37 | 51 | 95 | 75 |
| Aspartate aminotransferase (U/l) | 21 | 9600 | 6266 | 2424 | 619 |
| Alanine aminotransferase (U/l) | 19 | 6117 | 2047 | 886 | 652 |
| Gamma-glutamyl transferase (U/I) | 26 | 46 | 41 | 35 | 39 |
| Total bilirubin (mg/dl) | <1 | 1.8 | 4.1 | 6.8 | 12.3 |
| Direct bilirubin (mg/dl) | – | 0.7 | 3.6 | 5.4 | 9.5 |
| Haemoglobin (g/dl) | 13.1 | 6.6 | 6.8 | 7.7 | 8.4 |
| Platelets (×103/μl) | 200 | 128 | 54 | 42 | 45 |
| Prothrombin rate (%) | 99 | Not detected | 27 | 50 | 46 |
| Fibrinogen (mg/dl) | 566 | Not detected | 87 | 197 | 239 |
Total open or partial cystectomy/pericystectomy requires the use of scolicidal agents intended to kill the parasite and impede its intraperitoneal spread. Various scolicidal agents have been used, including: silver nitrate, formaldehyde, oxygenated water, alcohol, povidone-iodine and HSS. HSS was used for the first time in 1950.1
The most serious complication of the use of HSS in hydatid cyst surgery is acute hypervolemic hypernatremia, which was first reported in 1982.3 Hypernatremia can occur because HSS is accidentally administered in a blood vessel of the liver, because it spills into the peritoneum, due to its absorption through the cyst wall or because it enters the gastrointestinal tract through possible connections between the cyst and the biliary tree. However, peritoneal absorption has been reported as the main cause.3,4 It is therefore stipulated that precautions be taken in using HSS to prevent contact with the peritoneal surface during surgery.1
In our case, approximately 5 l of 3% HSS were infused which is a high sodium load (2470 mOsm). According to the patient’s weight and height (60 kg and 155 cm, respectively), she may have gained 39.2 mOsm/kg of sodium of. The acute hypernatremia caused haemorrhagic shock due to haemolysis, disseminated intravascular coagulation and hyperfibrinolysis; previously, the patient had presented anaphylactic shock at the start of the surgery. All that triggered AKF and acute liver failure. In this case, to correct electrolyte imbalance, it was infused hypotonic solution such as 5% glucose plus furosemide. Another treatment option would be CVVHDF with high Na+ in the bath and slow blood flow rates. Conventional haemodialysis would not be considered since blood sodium levels would drop too quickly (although the Na+ in the dialysis bath can be increased). In our case, given the patient’s oligoanuric AKF and haemodynamic status, continuous renal replacement therapy was indicated.
The adverse effect reported could have a directly proportional relationship to the volume of HSS used.
In surgery for hepatic hydatid disease, which is increasingly uncommon, if HSS is used, blood sodium levels must be closely monitored.
Please cite this article as: Álvarez-Santamarta L, Bande JJ, Astudillo E, Gorostidi M, Díaz-Corte C. Hipernatremia grave tras el empleo de cloruro sódico hipertónico en cirugía de hidatidosis hepática. Nefrologia. 2021;41:597–598.



