


Chronic kidney disease (CKD) is a extremely important public health problem in part because it is not always diagnosed, the prevalence is high (10% of the adult population) with significant vascular morbidity and mortality1,2 The prevalence is increased in diabetic (men 29.3%/women 22.3%) and hypertensive patients (men 57%/women 61.4%) over the age of 60.3
The care of CKD patients is a burden for the Spanish public health system; the cost of care of patients with advanced CKD is aproximalety 800 million euros per year.2 And the prevalence of CKD will increase due to the rise in life expectancies and a greater prevalence of obesity, hypertension (HTN) and diabetes mellitus.4
Diabetic patients with kidney failure present higher morbidity and mortality rates than those with normal kidney function. The estimated glomerular filtration rate (eGFR) has been used to stage CKD; in 2013, the “Kidney Disease: Improving Global Outcomes” guidelines were updated to include the degree of albuminuria to better define de stage of CKD. This allows stratified risk assessment of CKD progression and both cardiovascular and overall mortality.5
Studies on HTN6 and diabetes mellitus7 recommend motorisation of albuminuria and the eGFR.
The use of electronic medical records (EMR) in primary care (PC) centres in Madrid allows us to obtain valid information to conduct epidemiological studies.1
The objective of this work is to determine the prevalence and risk of CKD progression in diabetic and/or hypertensive patients over the age of 40 in Primary Care facilities.
Observational study using EMRs under conditions of regular clinical practice in 263 PC centres in the Community of Madrid, which provided health care to approximately 6,384,000 people (population database). The data was collected from October first 2012 to March 31st 2013.
Patients over the age of 40, who had been diagnosed with HTN and/or diabetes, were included (International Classification of Primary Care, ICPC codes: K86, K87, T90). Excluded patients were those in whom less than 3 or more than 15 months had elapsed between the two consecutive determinations of creatinine or albuminuria. These determination were needed to match the CKD definition set out in the “Kidney Disease: Improving Global Outcomes”8 guidelines.
Creatinine and albuminuria values (albumin/creatinine ratio) were obtained from the EMRs that incorporate all this information directly from all the laboratories in the Community of Madrid. The eGFR value was estimated using the CKD-EPI equation.2
Data collection was performed retrospectively using “SQL” computer language on extracting information from the EMRs.
A total of 24,087 patients were included, with a mean age of 68.8 years (SD: 11.5), 56.6% were women; 22% (5292 patients) were diabetic; 27.5% (6613 patients) hypertensive and 50.6% (12,182 patients) had been diagnosed of both diabetes and hypertension. Table 1 presents the baseline clinical characteristics.
Baseline clinical characteristics of the patients.
| Mean (SD) | |
|---|---|
| Last two values | |
| eGFR CKD-EPI | 79.4 (23.4) |
| Albumin/creatinine ratio | 37.8 (135.0) |
| eGFR CKD-EPI | 79.6 (23.8) |
| Albumin/creatinine ratio | 42.3 (145.1) |
| Cardiovascular risk factors | |
| Cholesterol | 182.9 (34.7) |
| LDL cholesterol | 104.9 (30.3) |
| Mean SBP | 133.0 (12.4) |
| Mean DBP | 75.0 (7.9) |
| HbA1c | 7.0 (1.2) |
The prevalence of CKD in the population under study was 32.27% (95% CI: 31.67–32.86), with 11.4% (95% CI: 11.0–11.8) being due to the exclusive presence of albuminuria (G1-G2/A2-A3). Among the diabetic patients, the prevalence of CKD was 16.95% (95% CI: 15.91–17.95). In the hypertensive patients, it was 24.62% (95% CI: 23.57–25.66), and in those with both diseases it was 31.22% (95% CI: 30.39–32.04).
Table 2 shows the distribution across the different stages of CKD and the risk of progression.
Distribution (in percentages) in chronic kidney disease stages and risk of progression.
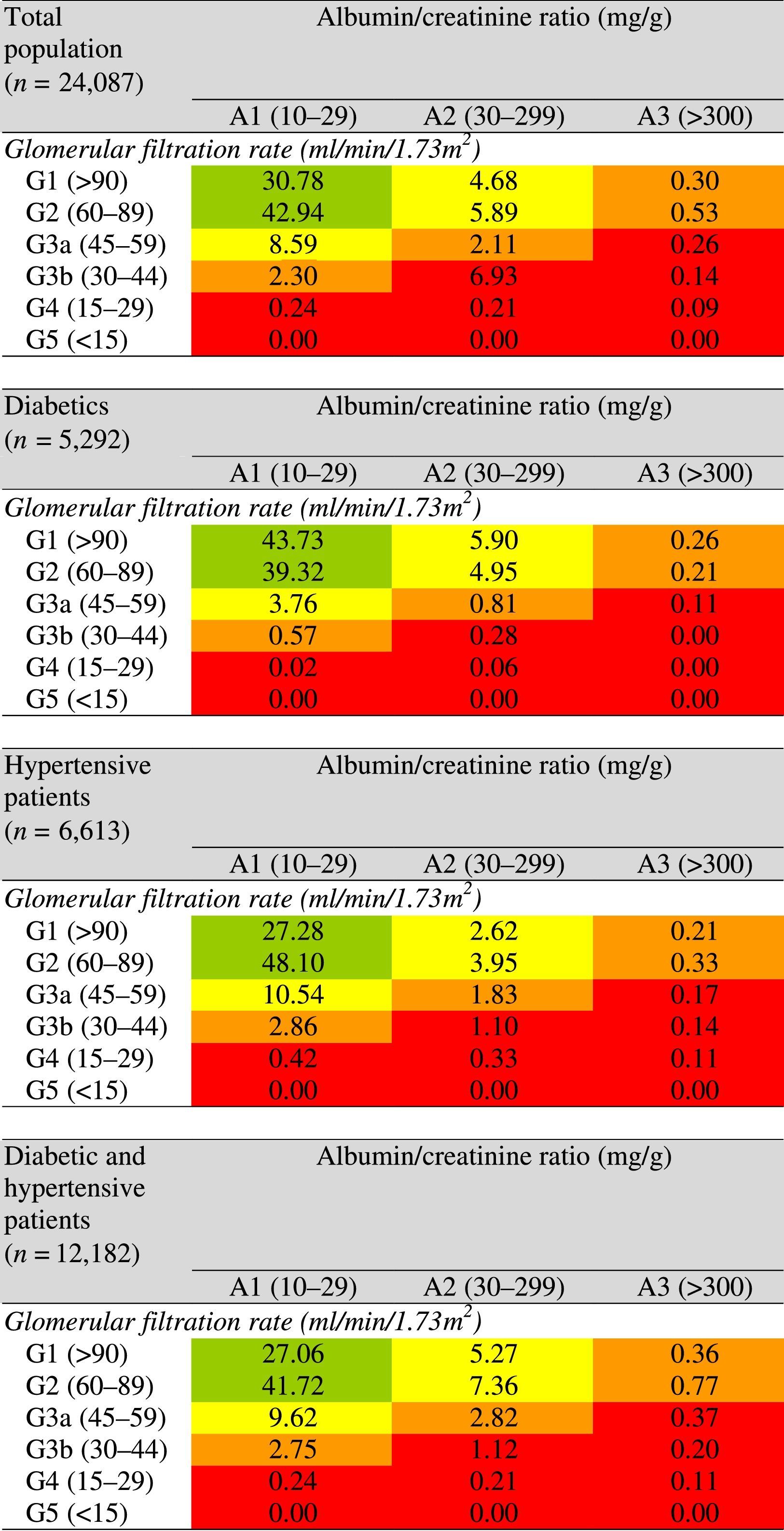
The colours show the adjusted risk ratio for five events (overall mortality, cardiovascular mortality, kidney failure treated with dialysis or transplant, acute kidney failure and CKD progression). The lowest risk corresponds to green (“low risk” category; in the event that there is no data of kidney injury, it may not even be categorised as CKD), followed by yellow (“moderately increased” risk), orange (“high risk”) and red (“very high risk”).2
The overall results of our study coincide with other publications, in which a high prevalence of CKD is observed in hypertensive patients (24%) over the age of 18.8 Among diabetics, there is a large variability, with prevalences of 17.3%9 to 34.6%.7 It is evident that a greater proportion of diabetic patients have albuminuria as compatred with hypertensive patients. This is particularly relevant since some studies have shown that it is an independent risk factor of cardiovascular and all-cause mortality r in primary prevention.10 By contrast, the proportion of patients with a reduced eGFR is greater in hypertensive patients.3
The study's limitations include the impossibility to separate different ethnic groups through the EMRs, for which reason the differentiating equation cannot be applied for eGFR. There may be a significant number of losses among patients with advanced CKD since they have prolonges follow up in hospital facilities. Our work was performed in a population followed in PC that met the full definition of CKD,8 which means that the precision (reduction of random error) of this study is large in patients in early stages of CKD, i.e. patients who are routinely monitored in our setting.
In conclusion, the prevalence of CKD is greater in patients with HTN than diabetics, although there was a greater proportion of diabetic patients with albuminuria. These two populations are at risk of CKD progression and cardiovascular mortality; controlling cardiovascular risk factors and adjusting nephrotoxic drugs according to the stage of the disease is thus extremely important to reduce disease progression.
Please cite this article as: Alemán-Vega G, Gómez Cabañas I, Reques Sastre L, Rosado Martín J, Polentinos-Castro E, Rodríguez Barrientos R. Prevalencia y riesgo de progresión de enfermedad renal crónica en pacientes diabéticos e hipertensos seguidos en atención primaria en la Comunidad de Madrid. Nefrología. 2017;37:343–345.



