


Music has been closely linked to medicine since ancient times, and has brought numerous benefits to the health of patients. Patients with chronic kidney disease (CKD) undergoing hemodialysis (HD) generally have a health-related quality of life (HRQL) lower than the reference values of the general population. The objective of the present study is to verify if the intervention of classical music live and “in situ” during the treatment of HD has effects on the HRQoL of the patients.
Materials and methodsA prospective, group-randomized intervention study of 4 weeks’ duration was carried out in patients with chronic kidney disease undergoing hemodialysis. Descriptive variables are included for data analysis: age, sex, months in treatment, Kt/V, hemoglobinand albumin. Result variable: HRQL, measured with the Kidney Diseasse health questionnaire Quality of life (KDQOL-SF) before and after the musical intervention.
ResultsPatients participated in 2 groups, the intervention group and the control group. The analysis of the results shows that the intervention group improved their quality of life compared to the initial measurement. The difference between the pre and post time of the intervention group with respect to the control group increased the mean score (pm) in all the scales significantly, except in the Work situation, Sexual function and Social support scales. The most important results were given on the Symptoms/problems scale with an increase of 15.78 (p < 0.001) pm; in scale Effects of kidney disease with an increase of 14.96 (p < 0.001) pm; in scale Burden of kidney disease with an increase of 16.36 (p < 0.001) pm; on the Dream scale with an increase of 14.78 (p < 0.001) pm; on the Vitality scale with an increase of 25.46 (p < 0.001) pm; on the Emotional well-being scale with an increase of 29.57 (p < 0.001) pm; on the Pain scale with an increase of 41.92 (p < 0.001) pm and on the General Health scale with an increase of 23.39 (p < 0.001) pm.
ConclusionIntervention with live music and on-site while receiving hemodialysis treatment improves self-perceived HRQL in patients with chronic kidney disease.
La música ha estado estrechamente unida a la medicina desde la antigüedad, y ha aportado numerosos beneficios a la salud de los pacientes.El paciente con enfermedad renal crónica (ERC) en tratamiento de hemodiálisis (HD), generalmente, presenta una calidad de vida relacionada con la salud (CVRS) inferior a los valores de referencia de la población general. El objetivo del presente estudio es verificar si la intervención de música clásica en directo e “in situ” durante el tratamiento de HD tiene efectos sobre la CVRS de los pacientes.
Materiales y métodosSe realizó un estudio de intervención, prospectivo y aleatorizado por grupos, en pacientes con ERC en tratamiento con HD. Durante 4 semanas un grupo de pacientes recibía la intervención con música clásica en directo 30 o 40 minutos durante las sesiones de HD, mientras el grupo control realizaba el tratamiento habitual. Variables descriptivas: edad, sexo, meses en tratamiento, Kt/V, hemoglobina y albúmina. Variable resultado: CVRS, se midió con el cuestionario de salud Kidney Diseasse Quality of life (KDQOL-SF) antes y después de la intervención musical.
ResultadosParticiparon 90 pacientes distribuidos en 2 grupos, el grupo intervención y el grupo control. El análisis de los resultados muestra que el grupo con intervención mejoró su calidad de vida respecto a la medición inicial. La diferencia entre el momento pre y post del grupo intervención respecto al grupo control, aumentó la puntuación media (pm) en todas las escalas de forma significativa, excepto en las escalas Situación laboral, Función sexual y Apoyo social. Los resultados más importantes se dieron en escala Síntomas/problemas con un aumento de 15.78 (p < 0.001) pm; en escala Efectos enfermedad renal con un aumento de 14.96 (p < 0.001) pm ; en escala Carga enfermedad renal con un aumento de 16.36 (p < 0.001) pm; en escala Sueño con un aumento de 14.78 (p < 0.001) pm; en escala Vitalidad con un aumento de 25.46 (p < 0.001) pm; en escala Bienestar emocional con un aumento de 29.57 (p < 0.001) pm; en escala Dolor con un aumento de 41.92 (p < 0.001) pm y en escala Salud General con un aumento de 23.39 (p < 0.001) pm.
ConclusiónLa intervención con música en directo durante el proceso de tratamiento de hemodiálisis mejora la CVRS auto percibida en pacientes con enfermedad renal crónica.
Quality of life is a multidimensional concept, encompassing several dimensions, such as physical, social and emotional, which appraise the personal well-being of patients. It is a very useful variable to evaluate the efficiency of treatments and to predict the possible negative effects of the disease,1 for this reason it has become a fundamental perception for the integral care of the patient.2
Most studies on health-related quality of life (HRQoL) in patients with chronic kidney disease (CKD) on hemodialysis (HD) show that these patients have a lower HRQoL than the reference values of the general population in all subscales of the SF-36 questionary.3–8
It is important to note the review of studies on HRQOL in advanced CKD in Spain, carried out by Rebollo-Rubio et al.;9 after the analysis of 53 articles published between 1995 and May 2014, it was concluded that, in most of the studies analyzed, the HRQOL was significantly affected in patients treated with dialysis.
There are several instruments to measure HRQOL, among them the Kidney Disease Quality of Life (KDQOL-SF) health questionnaire.10 This is a mixed scale that evaluates components for the general population, and at the same time it has a specific level for CKD. The KDQOL-SF scale is one of those with most publications relative to its validation and adaptation to different languages worldwide and its psychometric characteristics are reliable, Cronbach's alpha is >0.7, and its utility is adequate because it is easy to apply and not very complex.11
Many authors have investigated the impact of live music intervention on different pathologies. Through music therapy, it has been shown that music has a beneficial effect and has managed to reduce levels of stress, pain, anxiety, applying it as an adjuvant to treatments.12–18 For example, in the study by Bradt et al.19 they conducted a systematic review of the impact of music therapy (a personalized musical treatment offered by trained music therapists) and music medicine (listening to music recorded by a doctor or nurse), and the physical and psychological effects on cancer patients. They analyzed a total of 52 clinical trials with 3,731 patients, divided into 23 trials of music therapy and 29 as music medicine. They concluded that musical interventions can have beneficial effects on anxiety, pain, fatigue and quality of life in these patients. In addition, they observed that music may have a discrete effect on heart rate, respiratory rate, and blood pressure. However, most of the trials analyzed had a significant bias, so the results should be interpreted with caution.
In addition, Uchiyama et al.20 investigated the effect of music on the regulation of the immune response in mice undergoing heart transplantation. They concluded that mice exposed to opera-type music (La Traviata), classical music (Mozart), or Enya music had a greater regulatory response (decreased IL-2 and interferon-γ) than those that were not exposed.
However, we have not found any study that has examined in depth the influence that music can have on the quality of life of renal patients; therefore, the aim of the study was to test the effect of listening to live classical music in the patient's own living room while receiving HD treatment on the HRQOL of patients with CKD.
Material and methodsThis is a prospective randomized intervention study, with cluster randomization for logistic reasons. It was carried out in a hospital HD unit with 3 shifts per day (morning, afternoon and evening). For reasons of time incompatibility of the musicians, the night shift was excluded from the study and the study was carried out in 4 dialysis shifts with a total of 120 patients:
- A
Monday, Wednesday and Friday mornings.
- B
Monday, Wednesday and Friday afternoons.
- C
Tuesday, Thursday and Saturday mornings.
- D
Tuesday, Thursday and Saturday afternoons.
Patients were informed both orally and in writing of the details of the study, its risks, benefits, and the inclusion and exclusion criteria for participation in the research project.
Inclusion criteria: Patients over 18 years of age, give informed consent, have been in chronic HD program for more than 3 months.
Exclusion criteria: inability to hear the music, inability to answer the surveys, failure to give informed consent to participate, under 18 years of age, hospital admissions for more than 4 weeks or in the last 2 weeks of the intervention.
All those who met the inclusion criteria and decided to voluntarily participate in the study received and signed the informed consent to allow access to their medical data.
A draw was made through stratified sampling to form 2 groups, an intervention group (IG) made of shifts A and D, which had the music component, and a control group (CG) made of shifts B and C according to the results of the draw.
During the one-month period, live musical performances were held in the HD rooms in 2 of the 3 weekly sessions. The musical sessions lasted about 30/40 min. Patients completed the KDQOL-SF questionnaire, during the 2.a and 3.a hour dialysis session, at baseline and in the last week of the intervention.
The descriptive variables recorded were:
- none-
Cause of kidney disease.
- none-
Months on HD treatment.
- none-
Sex.
- none-
Age.
- none-
Vascular access: arteriovenous fistula or central venous catheter.
- none-
Kt/V Daugirdas 2.a generation based on serum urea specifications before and after HD.
- none-
Consumption of psychotropic and/or analgesic medication.
- none-
Serum hemoglobin (g/dL).
- none-
Serum albumin (g/dl).
- none-
Mean blood pressure (mmHg) on the day of the survey.
The outcome variable was the score obtained in the KDQOL-SF quality of life questionnaire.
Regarding the sample size, it was calculated that, accepting an alpha risk of 0.05 and a beta risk of 0.2 in a bilateral contrast, a total of 36 patients were needed in each of the groups to detect a difference equal to or greater than 2 points. The common standard deviation was assumed to be 3 and a correlation coefficient between the initial and final measurements of 0.6. A loss-to-follow-up rate of 20% was estimated. Therefore, more than 36 patients per group were recruited.
The present study respects the fundamental principles established in the Declaration of Helsinki, in the Council of Europe Convention on Human Rights and Biomedicine, in the UNESCO Universal Declaration on the Human Genome and Human Rights, and it meets the requirements established in the Spanish legislation according to the Data Protection Act 3/2018 of December 5, in the field of biomedical research, protection of personal data and bioethics.
Intervention: development of the musical sessionsFor the development of the musical sessions, 30 professional musicians collaborated, all of them teachers of higher conservatories, teachers of professional music conservatories and musicians of professional orchestras, which allowed us to form many and varied chamber music groups and play a large repertoire of musical pieces of different styles, from Bach, Beethoven or Mozart, to music of groups such as Queen or the Celtas Cortos. The number of musicians per group was limited to a maximum of 4 per session, since the musical sessions took place between beds and health personnel, avoiding interfering with patient care.
Four weekly auditions were performed during the month; the 90 IG patients listened to all the chamber ensembles, thus avoiding any kind of bias. The HD room is distributed in 3 subrooms, the musicians were placed in different locations to facilitate visual contact with the patient and not only auditory contact. Fig. 1 shows images of the performances.
KDQOL-SF questionnaire
Among all the questionnaires we chose for the study the KDQOL-SF, adapted to Spanish.21
It is a quality of life questionnaire specifically for patients with kidney disease who are on dialysis and focuses on their problems and concerns.
It has a generic part and a specific part for HD patients.
The generic part consists of the SF-36 questionnaire, which is internationally recognized and used for multicenter studies and has also been adapted to Spanish.22
- •
Physical function.
- •
Social function.
- •
Limitations due to physical difficulties.
- •
Limitations due to emotional difficulties.
- •
Good psychological state.
- •
Vitality/exhaustion.
- •
General feeling of health.
In the last item of the KDQOL-SF patients have to evaluate their overall health on a scale of 0–10 (where 0 would be "the worst possible health" and 10 "the best possible health"), and which represents the patient's overall subjective assessment of their health.
The specific part has 43 items for patients with kidney disease distributed as follows among 11 disease-specific dimensions:
- •
Symptoms/problems.
- •
Daily difficulties due to the disease.
- •
Weight of the disease.
- •
Employment status.
- •
Cognitive function.
- •
Social activity.
- •
Sexual activity.
- •
Sleep-related difficulties.
- •
Social support.
- •
Quality of the attitude of the service staff.
- •
Patient satisfaction.
The score for each dimension ranges from 0 to 100, where higher scores represent better health status, except in the specific scale of cognitive function and quality of social relationships where the highest score represents worse health status.
Statistical analysisFirst, a descriptive analysis of the dependent and independent variables studied was carried out. In this analysis, the variables are presented as mean, standard deviation, median and first and third quartiles in the case of continuous variables, and as relative and absolute frequencies in the case of categorical variables, in order to visualize their distribution and look for possible sources of error in those cases where outliers are present.
For the statistical analysis, several linear mixed regression models were fitted, one per dependent variable (in this case the different dimensions of the questionnaire), to analyze and compare the temporal evolution of each variable in the 2 study groups (control and intervention). All models also included age, sex, Kt/V, hemoglobin, systolic and diastolic blood pressure, and albumin as covariates (fixed effects). To evaluate the difference in the temporal evolution of these variables in both groups, the interaction between time instant and group was included in the models. This interaction is necessary to assess how the 2 groups diverge with time progression. To account for the non-independence of observations in the case of repeated measures per patient (variables measured for the same patient in 2 different time periods), a random intercept was added to the models with the patient as a random factor.
To assess the statistical significance of the estimates, we calculated p-values for fixed effects using the Satterthwaite approximation to the degrees of freedom. A value of p < 0.05 was considered statistically significant. All models were diagnosed by examining the normality of the residuals and testing for heteroscedasticity.
All statistical analyses were performed with R software (version 3.4.1; R Foundation for Statistical Computing, Vienna, Austria) using mainly the lme4 package (version 1.1–17).
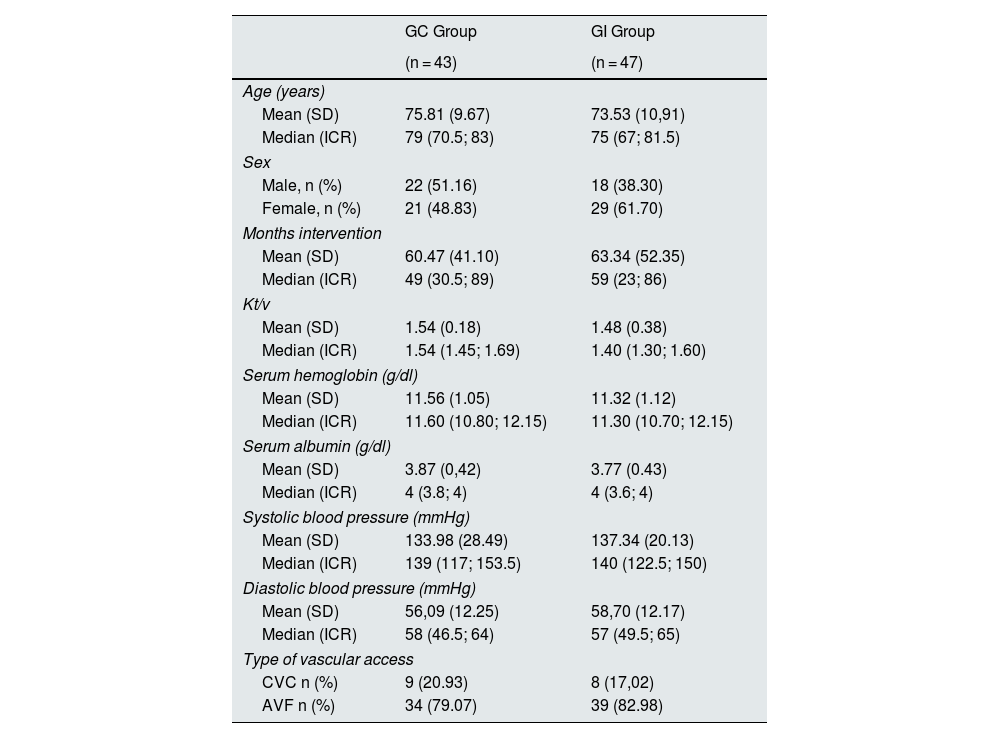
ResultsA total of 120 patients were selected for the study, 92 agreed to participate and the sample was finally reduced to 90; one patient died and was eliminated and the other was to transfered to another hospital. The clinical and demographic characteristics of the patients included in this study are specified in Table 1.
Clinical and demographic characteristics of the population included in the study.
| GC Group | GI Group | |
|---|---|---|
| (n = 43) | (n = 47) | |
| Age (years) | ||
| Mean (SD) | 75.81 (9.67) | 73.53 (10,91) |
| Median (ICR) | 79 (70.5; 83) | 75 (67; 81.5) |
| Sex | ||
| Male, n (%) | 22 (51.16) | 18 (38.30) |
| Female, n (%) | 21 (48.83) | 29 (61.70) |
| Months intervention | ||
| Mean (SD) | 60.47 (41.10) | 63.34 (52.35) |
| Median (ICR) | 49 (30.5; 89) | 59 (23; 86) |
| Kt/v | ||
| Mean (SD) | 1.54 (0.18) | 1.48 (0.38) |
| Median (ICR) | 1.54 (1.45; 1.69) | 1.40 (1.30; 1.60) |
| Serum hemoglobin (g/dl) | ||
| Mean (SD) | 11.56 (1.05) | 11.32 (1.12) |
| Median (ICR) | 11.60 (10.80; 12.15) | 11.30 (10.70; 12.15) |
| Serum albumin (g/dl) | ||
| Mean (SD) | 3.87 (0,42) | 3.77 (0.43) |
| Median (ICR) | 4 (3.8; 4) | 4 (3.6; 4) |
| Systolic blood pressure (mmHg) | ||
| Mean (SD) | 133.98 (28.49) | 137.34 (20.13) |
| Median (ICR) | 139 (117; 153.5) | 140 (122.5; 150) |
| Diastolic blood pressure (mmHg) | ||
| Mean (SD) | 56,09 (12.25) | 58,70 (12.17) |
| Median (ICR) | 58 (46.5; 64) | 57 (49.5; 65) |
| Type of vascular access | ||
| CVC n (%) | 9 (20.93) | 8 (17,02) |
| AVF n (%) | 34 (79.07) | 39 (82.98) |
CVC, central venous catheter; AVF, arteriovenous fistula; CG, control group; ICR, interquartile range; SD, standard deviation; IG, intervention group.
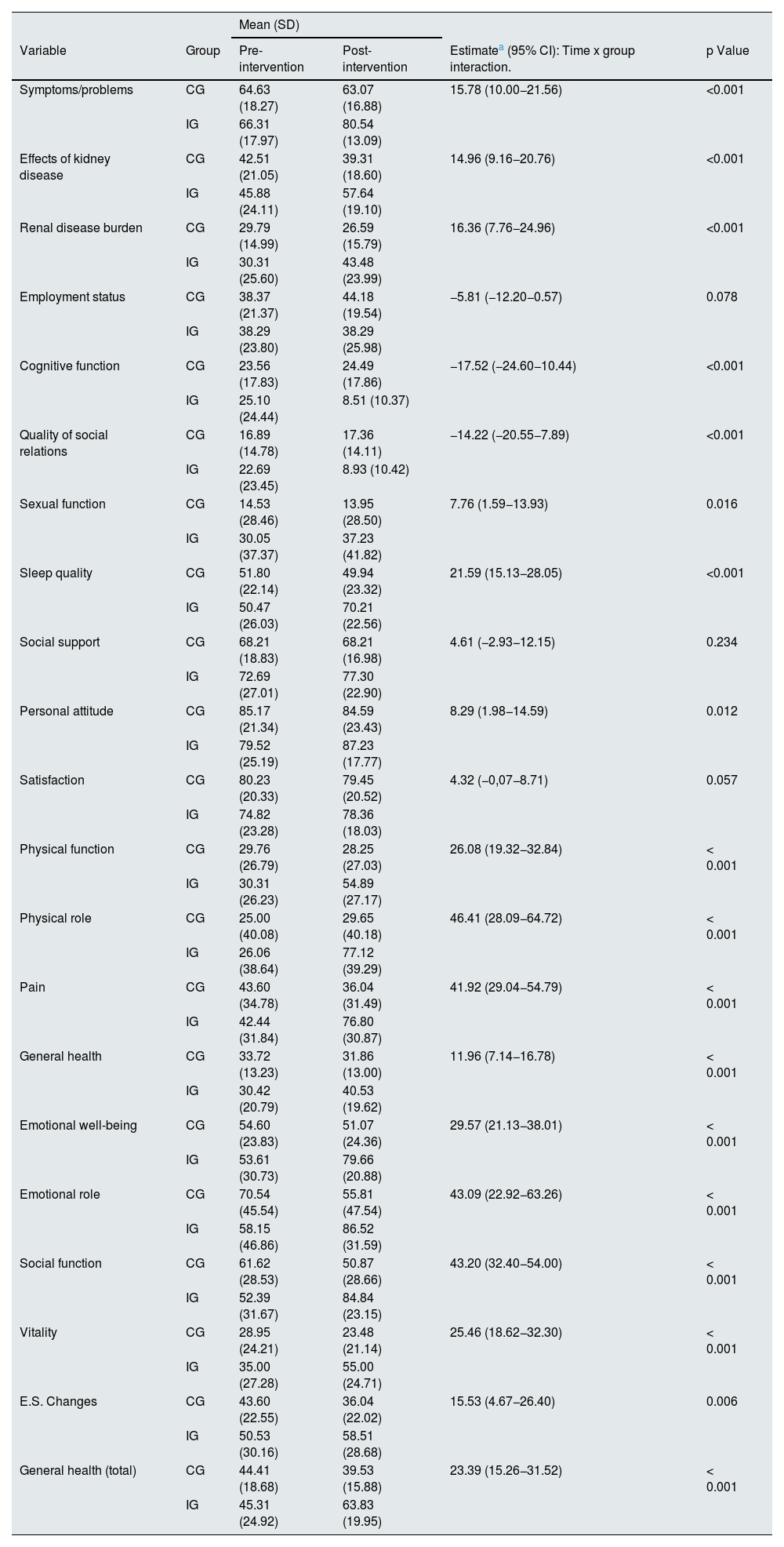
The results of the statistical analysis show that the difference between the time pre- and post- in IG as compared to the CG increased the mean score significantly in 18 of the 21 test scales (Table 2). The results indicate that the control and intervention groups have evolved differently between the 2 time points, and that this difference in evolution is significant in 18 scales of the test. The Pain, Social Function, Emotional Role and Physical Role scales are noteworthy, since these variables in the IG underwent an increase that differed by more than 40 points with respect to the difference in these same variables in the CG between the 2 time points (Fig. 2).
Time evolution of the analyzed scales of the KDQOL-SF questionnaire for the control group (CG) and the intervention group (IG).
| Mean (SD) | |||||
|---|---|---|---|---|---|
| Variable | Group | Pre-intervention | Post-intervention | Estimatea (95% CI): Time x group interaction. | p Value |
| Symptoms/problems | CG | 64.63 (18.27) | 63.07 (16.88) | 15.78 (10.00−21.56) | <0.001 |
| IG | 66.31 (17.97) | 80.54 (13.09) | |||
| Effects of kidney disease | CG | 42.51 (21.05) | 39.31 (18.60) | 14.96 (9.16−20.76) | <0.001 |
| IG | 45.88 (24.11) | 57.64 (19.10) | |||
| Renal disease burden | CG | 29.79 (14.99) | 26.59 (15.79) | 16.36 (7.76−24.96) | <0.001 |
| IG | 30.31 (25.60) | 43.48 (23.99) | |||
| Employment status | CG | 38.37 (21.37) | 44.18 (19.54) | −5.81 (−12.20−0.57) | 0.078 |
| IG | 38.29 (23.80) | 38.29 (25.98) | |||
| Cognitive function | CG | 23.56 (17.83) | 24.49 (17.86) | −17.52 (−24.60−10.44) | <0.001 |
| IG | 25.10 (24.44) | 8.51 (10.37) | |||
| Quality of social relations | CG | 16.89 (14.78) | 17.36 (14.11) | −14.22 (−20.55−7.89) | <0.001 |
| IG | 22.69 (23.45) | 8.93 (10.42) | |||
| Sexual function | CG | 14.53 (28.46) | 13.95 (28.50) | 7.76 (1.59−13.93) | 0.016 |
| IG | 30.05 (37.37) | 37.23 (41.82) | |||
| Sleep quality | CG | 51.80 (22.14) | 49.94 (23.32) | 21.59 (15.13−28.05) | <0.001 |
| IG | 50.47 (26.03) | 70.21 (22.56) | |||
| Social support | CG | 68.21 (18.83) | 68.21 (16.98) | 4.61 (−2.93−12.15) | 0.234 |
| IG | 72.69 (27.01) | 77.30 (22.90) | |||
| Personal attitude | CG | 85.17 (21.34) | 84.59 (23.43) | 8.29 (1.98−14.59) | 0.012 |
| IG | 79.52 (25.19) | 87.23 (17.77) | |||
| Satisfaction | CG | 80.23 (20.33) | 79.45 (20.52) | 4.32 (−0,07−8.71) | 0.057 |
| IG | 74.82 (23.28) | 78.36 (18.03) | |||
| Physical function | CG | 29.76 (26.79) | 28.25 (27.03) | 26.08 (19.32−32.84) | < 0.001 |
| IG | 30.31 (26.23) | 54.89 (27.17) | |||
| Physical role | CG | 25.00 (40.08) | 29.65 (40.18) | 46.41 (28.09−64.72) | < 0.001 |
| IG | 26.06 (38.64) | 77.12 (39.29) | |||
| Pain | CG | 43.60 (34.78) | 36.04 (31.49) | 41.92 (29.04−54.79) | < 0.001 |
| IG | 42.44 (31.84) | 76.80 (30.87) | |||
| General health | CG | 33.72 (13.23) | 31.86 (13.00) | 11.96 (7.14−16.78) | < 0.001 |
| IG | 30.42 (20.79) | 40.53 (19.62) | |||
| Emotional well-being | CG | 54.60 (23.83) | 51.07 (24.36) | 29.57 (21.13−38.01) | < 0.001 |
| IG | 53.61 (30.73) | 79.66 (20.88) | |||
| Emotional role | CG | 70.54 (45.54) | 55.81 (47.54) | 43.09 (22.92−63.26) | < 0.001 |
| IG | 58.15 (46.86) | 86.52 (31.59) | |||
| Social function | CG | 61.62 (28.53) | 50.87 (28.66) | 43.20 (32.40−54.00) | < 0.001 |
| IG | 52.39 (31.67) | 84.84 (23.15) | |||
| Vitality | CG | 28.95 (24.21) | 23.48 (21.14) | 25.46 (18.62−32.30) | < 0.001 |
| IG | 35.00 (27.28) | 55.00 (24.71) | |||
| E.S. Changes | CG | 43.60 (22.55) | 36.04 (22.02) | 15.53 (4.67−26.40) | 0.006 |
| IG | 50.53 (30.16) | 58.51 (28.68) | |||
| General health (total) | CG | 44.41 (18.68) | 39.53 (15.88) | 23.39 (15.26−31.52) | < 0.001 |
| IG | 45.31 (24.92) | 63.83 (19.95) | |||
The estimate reflects the interaction between time and group, btained using linear mixed regression models. More specifically, the estimate indicates the difference between the time evolution (post-intervention time minus pre-intervention time) of the IG with respect to the time evolution of the CG for each of the study variables. In this case, a positive estimate indicates that the variable has increased its value in the IG after the intervention and by a greater amount than in the CG.
 and the intervention group (IG) at the 2 time points analyzed (pre- and post-intervention). The horizontal lines indicate the mean value of the scale for CG and IG respectively at each time point. In relation to the statistical data obtained, the difference in the temporal evolution of the two groups is very pronounced in the Pain, Social Function and Emotional Role scales, since the values of these scales increase considerably in GI, but decrease in CG. On the other hand, the Physical Role scale increases in both groups, but the increase in IG is much greater than in the CG group.")
Distribution of the Pain, Social Function, Emotional Role and Physical Role scales of the KDQOL-SF questionnaire for the control group (CG) and the intervention group (IG) at the 2 time points analyzed (pre- and post-intervention). The horizontal lines indicate the mean value of the scale for CG and IG respectively at each time point. In relation to the statistical data obtained, the difference in the temporal evolution of the two groups is very pronounced in the Pain, Social Function and Emotional Role scales, since the values of these scales increase considerably in GI, but decrease in CG. On the other hand, the Physical Role scale increases in both groups, but the increase in IG is much greater than in the CG group.
As for, the analysis of covariates, in the linear mixed regression models implemented only the effects of sex and albumin were significant (p < 0.05) for several of the test dimensions. The remaining covariates studied were not significant (p > 0.05) for any of the dimensions studied.
Specifically, the effect of sex (male over female) was significant (p < 0.05) for the dimensions Symptoms/problems (9.12), Effects renal disease (8.75), Sexual function (20.21), Physical function (12.21), Physical role (9.12), Pain (18.63), Social function (12.07) and S.E. changes (11.60). In all these variables, the effect was positive, so it can be deduced that the score of the test variables tends to be higher in men.
Additionally, the effect of albumin turned out to be significant (p <. 0.05) for the dimensions Symptoms/problems (8.86), Effects renal disease (11.74), Burden renal disease (13.67), Vitality (18.87), Sexual function (21.16), Physical function (17.51), Physical role (16.20), Pain (19.25), Emotional well-being (17.87), Social function (17.31) and General health (13.89). In all these variables the effect was positive, so it can be deduced that the higher the albumin value the greater the response to the dimensions of the test.
DiscussionThe application of music in medicine has been present since ancient times, and has evolved according to the customs and beliefs of each era; all this has been weaving the background of what we know today as music therapy.
According to Maranto,23 this concept in the field of medicine is defined as the use of music therapy strategies to help in the treatment of diseases and in the restoration of people's health.
Previous studies have revealed the benefits that music has on the disease in different pathologies, such as Oncology, ICU, Surgery, even in patients with kidney disease on HD treatment.24–27 In 2006, da Silva28 measured the therapeutic effect of music in patients with CKD on HD treatment, through a qualitative study by analyzing patients' narratives. He concluded that the presence of music in HD sessions had a satisfactory therapeutic effect. The therapy was positive in terms of alteration in the perception of time, providing feelings of well-being, joy, happiness, relaxation, entertainment, change in routine, absence of symptoms or positive thoughts. Other authors such as Bechert Carminha et al.29 analyzed the influence of the quaternary rhythm of music on emotions, on the perception of time and on the appearance of hypertension and pain in the patient during the dialysis session. The results showed that more than 80% of the patients reported that they felt better and also that time passed faster. In the clinical context, the study indicates that the musical intervention was beneficial, but was not determinant in the reduction of pain and blood pressure.
As we can see, most of these studies evaluate the effect of music on anxiety, stress and pain, however, the effect of music on the quality of life of the HD patient has not been evaluated. In addition, the application of music in most cases has not been carried out in a direct way but in a passive way through recorded music.
One of the innovations of our study is the fact that classical music was played live in the hospital itself, while the patients were receiving HD treatment. This direct contact, both visual and acoustic, could enhance the effect produced by music and should be the subject of future studies.
It should not be forgotten that patients with CKD have an HRQOL well below the reference values of the general population. Patients with CKD should be valued as biopsychosocial beings, since the emotional aspect is a determining factor for the success of treatment and for the improvement of quality of life.29 This self-perceived quality of life is what we have tried to improve in our study through musical exposure, the subjective well-being of patients, i.e. what they think and how they feel about their lives, after the application of music during HD. This well-conducted musical application has proved to be a relevant therapeutic resource and has favorably influenced the patient, since we have obtained a satisfactory and highly relevant result in 18 of the 21 scales. As limitations of the study we can consider that there was scarce representation of the working population, so the work situation scale is not evaluable due to the scarce representation of this population, only 20/90 were of working age and, of these, only 6 were working (6.6%) and of the population with a sexual life, only 70/90 (22.2%) had an active sexual life, the rest did not, due to age or lack of a partner. This may have influenced the lack of positive results on these scales found in our study. The social support scale was not modified by the music either, perhaps because the intervention was short term and changes in this type of parameters could be expected in a long term intervention, if they were to occur.
In short, we can deduce that the measurement of HRQOL should be present in the routine practice of renal units, since it provides us with very valuable and important information, and allows us to act on the most affected parameters. In addition, the results indicates that music should be part of the renal patient's treatment, since we have shown that it is an aid to improve their quality of life, and it is not harmful in any way, thus achieving the best possible state of well-being for these patients.
In conclusion, a live musical intervention during HD treatment improves self-perceived HRQoL in patients with CKD.
FinancingThis research has not received specific support from public sector agencies, commercial sector or non-profit entities.
Conflict of interestThe authors declare that they have no conflicts of interest.
Key concepts
- •
Patients with chronic kidney disease on hemodialysis treatment have a health-related quality of life lower than the reference values of the general population.
- •
Classical music performed live in hemodialysis rooms helps to improve the renal patient's self-perceived quality of life.
- •
The application of live music as an adjuvant to renal treatment is a relevant therapeutic resource that contributes favorably to the patient's health.
To the nursing staff of the hemodialysis unit for their invaluable collaboration.
To all the musicians who have participated in the study in a totally altruistic and voluntary way.



