
The most common cause of hypercalcaemia in patients with non-metastatic solid tumours is the secretion of parathyroid hormone-related (PTHr) protein.1
The patient is an 11-year-old female with no history of interest, to be evaluated for an abdominal mass. Upon arrival the patient showed high serum creatinine, hypercalcaemia and hypophosphatemia (Table 1). The baseline renal function test also showed hypercalciuria and hyperphosphaturia. CT scan showed a large intra-abdominal mass. A complete resection of the tumour was performed. An anatomopathological study revealed the presence of an ovarian granulosa cell tumour.
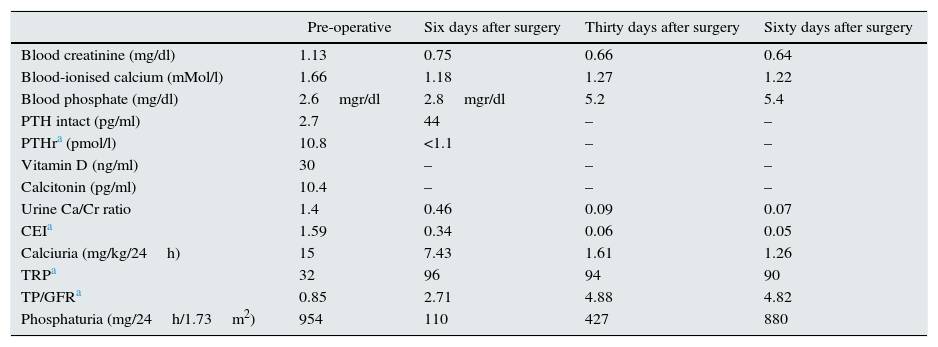
Biochemical blood and urine values prior to tumour removal and at days 6, 30 and 60 after surgery.
| Pre-operative | Six days after surgery | Thirty days after surgery | Sixty days after surgery | |
|---|---|---|---|---|
| Blood creatinine (mg/dl) | 1.13 | 0.75 | 0.66 | 0.64 |
| Blood-ionised calcium (mMol/l) | 1.66 | 1.18 | 1.27 | 1.22 |
| Blood phosphate (mg/dl) | 2.6mgr/dl | 2.8mgr/dl | 5.2 | 5.4 |
| PTH intact (pg/ml) | 2.7 | 44 | – | – |
| PTHra (pmol/l) | 10.8 | <1.1 | – | – |
| Vitamin D (ng/ml) | 30 | – | – | – |
| Calcitonin (pg/ml) | 10.4 | – | – | – |
| Urine Ca/Cr ratio | 1.4 | 0.46 | 0.09 | 0.07 |
| CEIa | 1.59 | 0.34 | 0.06 | 0.05 |
| Calciuria (mg/kg/24h) | 15 | 7.43 | 1.61 | 1.26 |
| TRPa | 32 | 96 | 94 | 90 |
| TP/GFRa | 0.85 | 2.71 | 4.88 | 4.82 |
| Phosphaturia (mg/24h/1.73m2) | 954 | 110 | 427 | 880 |
CEI: calcium excretion index; PTHr: parathyroid hormone-related protein; TP/GFR: phosphate per 100ml of glomerular filtration rate; TRP: tubular reabsorption of phosphate.
Clinical course was favourable. In the follow-up, one week after removal of the tumour, blood calcium levels normalised but urinary calcium remained high. The hypophosphataemia persisted, despite greater renal reabsorption of phosphate. After one month, all blood and urine biochemical parameters were within the normal range (Table 1).
Hypercalcaemia due to hypersecretion of PTHr by malignant tumours is an exceptional finding at paediatric age.2,3 Parathyroid hormone (PTH) and PTHr have shown similar effects in the renal handling of calcium and phosphate.4–7 They release calcium from bone and promote the renal reabsorption of calcium in the distal nephron. They also produce hyperphosphaturia by decreasing the tubular reabsorption of phosphate that may result in hypophosphataemia. However, patients with hyperparathyroidism may present with hypercalciuria.8 The elevated calcaemia in our patient is related to high levels of PTHr. Significantly, hypercalciuria persisted after excision of the tumour and normalisation of calcaemia levels.
Another remarkable finding was the presence of hypophosphataemia, which became significant. The hypophosphataemia coincided with a situation of renal phosphate loss, evidenced by low levels of TRP and TP/GFR, indicating that the hypophosphataemia was of renal origin.
In conclusion, we present a case of PTHr-mediated hypercalcaemia secondary to an ovarian tumour in an age group that is rarely affected by this condition. In addition to transient renal failure, the biochemical data show hypercalcaemia accompanied by hypercalciuria. The hypophosphataemia is secondary to an excessive loss of phosphate through the kidney.
Please cite this article as: Ubetagoyena Arrieta M, Martinez Sainz de Jubera J, García de Andoin Barandiaran N, Úriz Monaut JJ, López Cuesta S, Domínguez Castells A. Hipercalcemia e hipofosforemia en niña con tumour ovárico. Nefrologia. 2017;37:100–101.



