



In recent years, there is an increased prevalence of patients with advanced chronic kidney disease (ACKD) carrying tunneled central venous catheters (CVC) for haemodialysis.1,2
Catheter-related bacteraemia (CRB) is one of the major causes of morbidity and mortality in these patients.2
The microorganisms responsible for two-thirds of these bacteraemias are gram-positive bacteria,2 not forgetting the other microorganisms.
Ochrobactrum anthropi is a gram-negative, non-fermenting, aerobic, mobile, oxidase- and urease-positive bacillus.3 It is ubiquitous in nature and can be found in hospital environments. Several cases of bacteraemia associated with this microorganism have been described in immunocompromised patients, although some cases have also occurred in immunocompetent patients.4,5 Its isolation as the cause of CRB is rare.
Two cases of bacteraemia due to this microorganism in recent months are described below in patients with a CVC for haemodialysis.
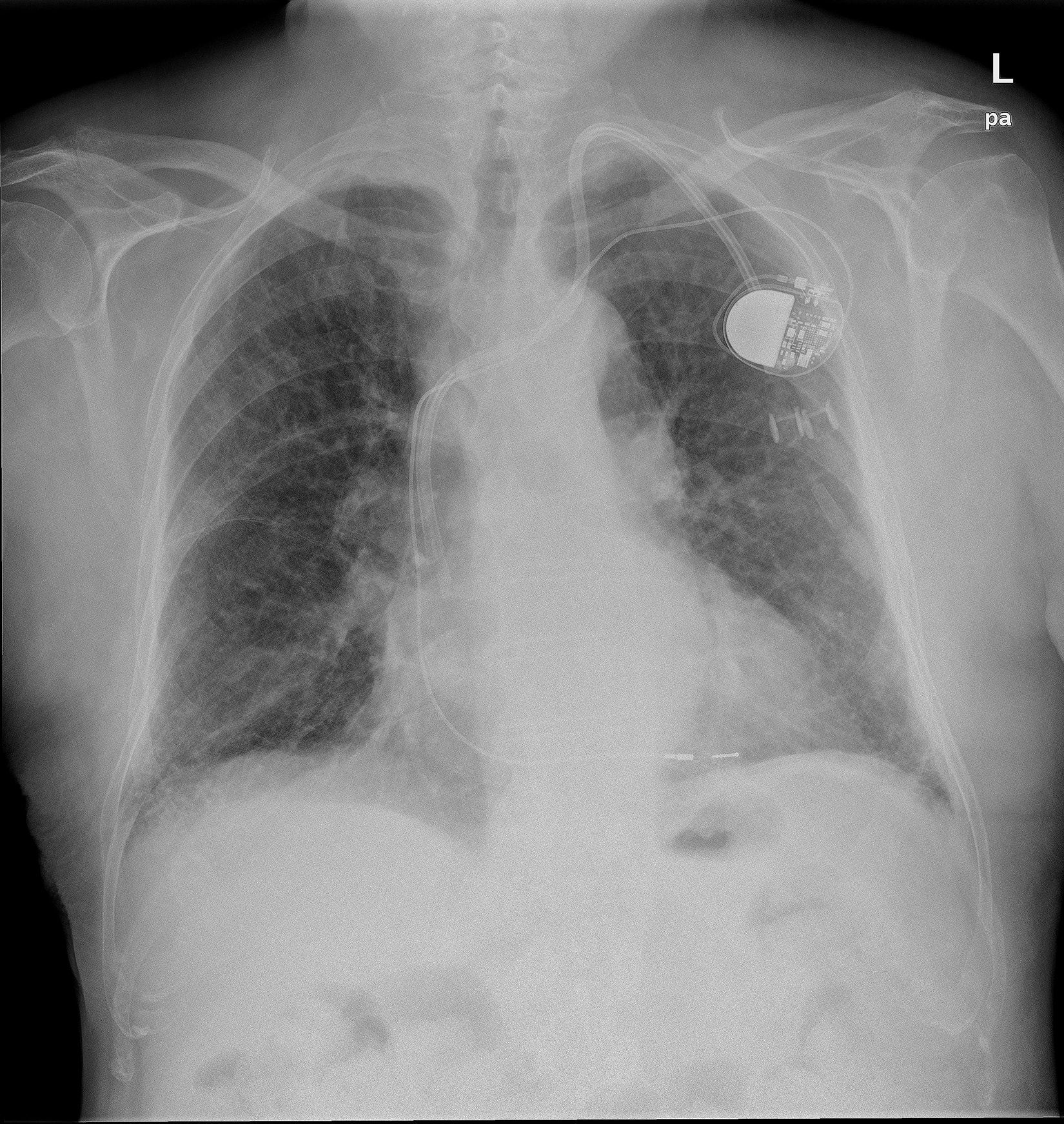
An 84-year-old male patient with pacemaker diagnosed with ACKD secondary to diabetic nephropathy in a haemodialysis program through tunneled jugular CVC, who was admitted with a diagnosis of CRB due to Ochrobactrum anthropi. Treatment was started with post-dialysis gentamicin and CVC sealing with ciprofloxacin, initially discarding replacement of the CVC because of the high risk of vessel tear and moving of the pacemaker cable that was wound around the catheter (Fig. 1). After 4 weeks of antibiotic therapy, given the absence of an infectious condition and the negativisation of blood cultures, treatment was discontinued.
Three months later he had a new episode of CRB due to Ochrobactrum anthropi, and was treated with meropenem and trimethoprim/sulfamethoxazole by antibiogram. A transoesophageal echocardiogram was performed, ruling out the presence of endocarditis. Finally, in view of the persistence of the condition, it was decided to remove the pacemaker and the CVC and implant a new epicardial pacemaker and femoral CVC, which resolved the condition without subsequent recurrences.
The second case is a 88-year-old diabetic and hypertensive woman with significant vasculopathy, diagnosed with ACKD secondary to diabetic nephropathy, on haemodialysis through a femoral CVC, who was admitted due to septic shock of uncertain origin. Empirical antibiotic therapy was started with vancomycin and meropenem, confirming the diagnosis of CRB due to Ochrobactrum anthropi. Despite significant clinical improvement, in view of the persistence of fever and given the history of the previous case, it was decided to remove the CVC and complete treatment with ciprofloxacin. Implanting a new CVC resolved the condition and there were no new infectious complications.
CRB due to Ochrobactrum anthropi is a very rare condition in our setting. This microorganism is a gram-negative bacillus, ubiquitous in nature, belonging to the Brucellaceae family, within the Alphaproteobacteria class.3 In recent years its importance has increased as an emergent pathogen in immunocompromised patients, especially in hospital settings,6 and the most commonly described infection is CRB, due to this bacteria's easy adherence to synthetic hospital materials, a characteristic similar to those of the genus Staphylococcus.5
Although most cases of infection from this microorganism have been described in immunocompromised patients, some cases have been described in immunocompetent patients.4,5
To date, there are few published cases of bacteraemia in patients on haemodialysis,5,7–9 none of them in Spain.
Endophthalmitis, meningitis, endocarditis, osteochondritis, pancreatic abscess and pelvic abscess conditions have been described.
In most of these, the strains of Ochrobactrum anthropi were resistant to beta-lactams and groups of antibiotics such as penicillins, cephalosporins and aztreonam, but were sensitive to aminoglycosides, fluoroquinolones, carbapenems, tetracyclines and trimethoprim/sulfamethoxazole. Resistance is mediated in part by the presence of inducible type AmpC β-lactamases.10 Our cases matched this pattern of sensitivity and resistance.
It should finally be noted that, as in other published cases, we did not see any local signs of infection at the catheter insertion site, with scant clinical expressiveness of the condition, except for the presence of fever. In the second case, the severity of the general condition of the patient was noteworthy, with no focal point of infection data, improving rapidly after starting antibiotic therapy. All this presents the need for high clinical suspicion with early diagnosis and treatment.
In conclusion, it is important to highlight the emergent role of Ochrobactrum anthropi as a pathogen responsible for CRB tunneled for haemodialysis. We also consider that early intravenous antibiotic treatment is important, and if no response is obtained within 48–72h of starting, early withdrawal of the dialysis catheter should be performed to definitively eradicate the microorganism.
Please cite this article as: Torres Aguilera E, Verde Moreno E, Muñoz P, Valerio M, Luño J. ¿Nuevo microorganismo en la bacteriemia asociada a catéter? Nefrologia. 2017;37:98–100.



