







Vascular calcification (VC) associated to chronic kidney disease (CKD) is a complex phenomenon closely related to mineral bone metabolism disorders. Many are the factors implicated, as the drugs used in the treatment of CKD. Some in vitro studies suggest that electrolyte and acid–base disorders induced by haemodialysis (HD) may play a key role in VC.
MethodsWe analysed electrolyte and acid–base disorders that occur during an HD session in 26 patients randomly assigned to 1.25mM or 1.5mM calcium bath.
ResultsThere is a calcium load in all the patients, independently of calcium bath concentration or basal serum calcium levels. At the end of the session, 100% of the patients dialysed with 1.5mM calcium bath have calcium serum levels >1.3mM. However, this only occurs in 15% of the patients dialysed with 1.25mM calcium bath. During this calcium load, phosphorus levels persist uncontrolled. Besides, there is a progressive alkalinisation in all the patients. In the end of the session 50% have serum bicarbonate >30mM and 23% pH >7.5.
ConclusionsDuring HD sessions occur electrolyte and acid–base disorders that induce VC: calcium load and alkalisation in presence of elevated phosphorus levels. It is necessary to perform studies with kinetic models of calcium load and alkalinisation different from the actual ones.
La calcificación vascular (CV) asociada a la enfermedad renal crónica (ERC) es un fenómeno estrechamente ligado a las alteraciones en el metabolismo mineral óseo. Existen muchos factores implicados, entre ellos los fármacos empleados en el tratamiento de la ERC. Algunos estudios in vitro señalan que las alteraciones electrolíticas y ácido-básicas que tienen lugar durante la sesión de hemodiálisis (HD) pueden jugar un papel clave en el proceso de CV.
MétodosAnalizamos las alteraciones electrolíticas y ácido-básicas que tienen lugar durante la sesión de HD en 26 pacientes, empleando de forma aleatorizada concentraciones de calcio en el líquido de diálisis de 1,25 o 1,5mM.
ResultadosEn todos los pacientes, independientemente del baño de calcio empleado, se produce una ganancia de calcio. En el grupo de pacientes dializados con baño de calcio 1,5mM, el 100% finaliza la sesión con valores de calcio sérico>1,3mM, mientras que en el de 1,25mM, esto solo ocurre en el 15%. Al inicio de la sesión, esta ganancia de calcio coincide con niveles de fósforo aún no controlado. Además, en todos los pacientes se observa una alcalinización progresiva: el 50% finaliza la sesión con cifras de bicarbonato>30mM y el 23% con pH>7,5.
ConclusionesDurante la sesión de HD se producen cambios electrolíticos y ácido-básicos inductores de CV: ganancia de calcio y alcalinización en presencia de fósforo sérico inicialmente elevado. Son necesarios estudios con modelos cinéticos de ganancia de calcio y alcalinización diferentes a los actuales.
Vascular calcification (VC), a process inherent to ageing, is influenced by multiple classical cardiovascular risk factors, such as arterial hypertension, diabetes mellitus, obesity, and dyslipidaemia, amongst others.1 In the general population, VC takes place in the intimal arterial layer,2 affecting mainly central arteries (the aorta and its branches) and is linked to systemic atherosclerosis.3
Cardiovascular events are the primary cause of morbidity and mortality in patients with chronic kidney disease (CKD).4 In these patients, 2 patterns of VC have been described: predominantly intimal, and predominantly medial. However, there is much debate regarding the differences between intimal calcification and medial calcification. There is no definitive evidence to suggest that calcification isolated to the media is distinct from the calcification that comes from the natural history of atherosclerosis; nor is there definitive evidence to the contrary.5,6 What is certain is that it is closely related to the mixture of metabolic and biological abnormalities that accompany CKD,7,8 notably CDK-mineral and bone disorders. This entity implies abnormalities in the metabolism of calcium, phosphorus,9 vitamin D,10,11 FGF23-Klotho, and parathyroid hormone (PTH).12 To those we must add biological abnormalities such as dysfunctional production of calcification inhibitors by smooth muscle cells, and chronic inflammation.13 Together, these factors induce physiochemical changes in the smooth muscle cells of the arterial wall, promoting their transformation into osteoblasts,14 and hydroxyapatite deposition. Classically, the [Ca]×[P] product has been used to determine VC risk in renal patients.15 However, some in vitro studies have demonstrated that with a stable [Ca]×[P] product, it is the individual concentration of each element that determines the development of VC.16
Until now, all therapeutic efforts have been directed at controlling these metabolic abnormalities (essentially phosphate binders,17 vitamin D derivatives,18 and calimimetics19) and the classical risk factors, with varying and contradictory results. Although some of these treatments can slow progression, none have been demonstrated to reverse VC.20,21
In comparison with patients in the early stages of CKD, patients treated with haemodialysis (HD) have higher cardiovascular morbidity and mortality,22 along with more marked abnormalities in bone metabolism and a greater degree of VC.23,24 As well as all the previously stated mechanisms, the biochemical changes produced during HD could play an important role in such marked development of VC.25 In fact, in vitro studies using rat aortas have shown that changes in calcium and phosphorus concentrations and alkalinisation are precipitating factors for VC.16,26 It is also known that acidosis protects against VC,27 therefore a high pH could have the unfavourable opposite effect.
AimsThe aim of this study was to analyse the biochemical changes in the parameters of mineral metabolism and acid–base balance that take place during HD.
Materials and methodsStudy designWe prospectively studied the changes in mineral metabolism and acid–base metabolism that occurred during haemodialysis sessions. We selected 26 stable patients with CKD who attended HD 3 times per week at our hospital centre. Mean patient age was 73.15 years±12.56 years, and 57.69% were men. Time on HD was 1871 days (standard deviation [SD] 2516.82 days; range, 45–12325 days). During the sessions it was not permitted to administer medication that would interfere with mineral metabolism or acid–base balance. All patients gave informed consent to participate in the study.
Thirteen patients (50%) were randomly allocated to receive dialysis with a calcium bath concentration of 1.25mM; the other 13 patients received dialysis with a calcium bath concentration was 1.5mM. The dialysis fluid in both groups had the same concentrations of bicarbonate, 35mM; magnesium, 0.5mM; potassium, 1.5mM; and sodium, 140mM.
All patients were conventionally dialysed over 4h with high flow Helixona® (Fx CorDiax 80®, Fresenius Medical Care, AG, Bad Homburg, Germany) with an ultrafiltration coefficient of 64mL/h/mmHg or with Evodial® (HeprAN Gambro) with ultrafiltration coefficient of 50mL/h/mmHg.
Biochemical parameters studiedBlood samples were taken at the start of the session and subsequently at 15, 30, 60, and 120min, and at 4h, coinciding with the end of the session, to evaluate the changes produced in the variables of mineral metabolism and acid–base metabolism over the course of the HD session.
Blood pH and ionised calcium normalised for pH (Ca++) were measured using direct potentiometry with an ion-selective electrode (ABL80 FLEX auto-analyser). Creatinine, urea, phosphorus, magnesium, and bicarbonate were measured using colourimetry (ADVIA 2400 auto-analyser. Siemens). Intact PTH levels in the baseline sample and final sample were measured using immunoassay (IDS-iSYS auto-analyser).
The calcium–phosphorus product is expressed in mg2/dL2. The values obtained for ionised calcium in mM were converted to mg/dL according to the molecular weight of calcium (Ca++ 1mM=4mg/dL).
Statistical analysisResults are expressed as mean and SD and 95% confidence interval. Statistical analysis was performed using Student's t test for independent data and a chi-square test.
ResultsThe 26 patients were classified according to their baseline calcium level, into hypocalcaemic and normocalcaemic, using the normal lower limit of Ca++ in out laboratory as a reference (range, 1.16–1.3mM). The normal limits of phosphataemia used were 2.5–4.5mg/dL. The main characteristics of the sample can be seen in Table 1, with patients grouped according to calcium bath used and baseline calcaemia. There were no significant differences between the groups regarding sex, age, days on HD, ultrafiltration, calcium bath used, or type of vascular access.
Patient characteristics, grouped by baseline calcaemia.
| Calcium bath | Baseline calcaemia | |||
|---|---|---|---|---|
| 1.25mM | 1.5mM | <1.16mM | >1.16mM | |
| n | 13 | 13 | 13 | 13 |
| Women/Men | 6/7 | 5/8 | 7/6 | 4/9 |
| Ca++ bath 1.25mM | X | X | 7 | 6 |
| Ca++ bath 1.5mM | X | X | 6 | 7 |
| Age, years | 70.23±16.18 | 76.08±6.95 | 72±13.13 | 74.31±12.38 |
| Days on HD | 2.410.92±3.323.29 | 1.331.08±1.233.21 | 1.114.23±1.432.07 | 2.627.77±3.147.22 |
| UF, mL | 18.54.58±830.59 | 2.002.50±720.95 | 2.075.18±543.13 | 1.804.46±915.19 |
| AVF/CVC | 6/7 | 7/6 | 4/9 | 9/4 |
Age, days on haemodialysis, and ultrafiltration are expressed as mean±standard deviation. There were no statistically significant differences between groups for any of the variables. AVF, ateriovenous fistula; CVC, central venous catheter.
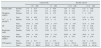
Table 2 shows the baseline and final values of the different parameters, grouped by calcium bath used and baseline calcium level. Table 3 shows the overall increase of each parameter assessed, which corresponds to the difference between the mean final and mean baseline values. All results are expressed as mean and SD.
Mean baseline and final levels of ionised calcium, phosphorus, Ca++×P product, pH, bicarbonate, magnesium, and PTH.
| Calcium bath | Baseline calcium | ||||
|---|---|---|---|---|---|
| 1.25mM | 1.5mM | <1.16mM | >1.16mM | ||
| Calcium (mM) | Baseline | 1.17±0.14 | 1.14±0.09 | 1.07±0.08 | 1.23±0.08 |
| Final | 1.25±0.09a | 1.37±0.04a | 1.28±0.10 | 1.34±0.08 | |
| Phosphorus (mg/dL) | Baseline | 5.05±1.74 | 5.04±1.70 | 5.08±1.55 | 5±1.87 |
| Final | 2.01±0.68 | 2.55±0.82 | 2.31±0.78 | 2.25±0.83 | |
| Ca++×P (mg2/dL2) | Baseline | 23.89±9.22 | 22.73±7.2 | 21.86±6.90 | 24.76±9.25 |
| Final | 10.10±3.84a | 13.99±4.41a | 11.94±4.55 | 12.15±4.65 | |
| pH | Baseline | 7.38±0.06 | 7.38±0.06 | 7.37±0.06 | 7.39±0.06 |
| Final | 7.48±0.04 | 7.45±0.06 | 7.46±0.04 | 7.47±0.06 | |
| Bicarbonate (mM) | Baseline | 24.88±3.31 | 25.82±3.57 | 25.59±3.9 | 25.12±2.97 |
| Final | 29.84±2.01 | 29.98±2.38 | 29.89±2.66 | 29.92±1.62 | |
| Magnesium (mg/dL) | Baseline | 2.43±0.39 | 2.32±0.42 | 2.38±0.43 | 2.38±0.39 |
| Final | 1.97±0.17 | 2.04±0.24 | 2±0.23 | 2.01±0.18 | |
| iPTH (pg/mL) | Baseline | 574.69±379.75a | 321.15±244.46a | 441±293.44 | 454.85±390.61 |
| Final | 496.23±400.61a | 229.62±236.18a | 296.31±338.36 | 429.54±361.48 | |
Expressed as mean and standard deviation.
Changes in ionised calcium, phosphorus, Ca++×P product, bicarbonate, pH, and magnesium, from start until end of haemodialysis session, by calcium bath and baseline calcaemia.
| Calcium bath | Baseline calcaemia | |||
|---|---|---|---|---|
| 1.25mM | 1.5mM | <1.16mM | >1.16mM | |
| ΔCa++ (mM) | 0.08±0.091 | 0.23±0.08a | 0.2±0.11b | 0.11±0.11b |
| ΔP (mg/dL) | −3.04±1.36 | −2.48±1.15 | −2.78±0.89 | −2.75±1.59 |
| ΔCa++×P (mg2/dL2) | −13.79±7.09a | −8.74±4.17a | −9.92±3.37 | −12.61±8.13 |
| ΔHCO3− (mM) | 4.95±2.03 | 4.15±2.39 | 4.30±2.05 | 4.81±2.41 |
| ΔpH | 0.10±0.08 | 0.07±0.07 | 0.09±0.06 | 0.08±0.09 |
| ΔMg++ (mg/dL) | −0.46±0.33 | −0.28±0.27 | −0.38±0.35 | −0.37±0.27 |
| ΔPTH (pg/mL) | −78.46±245.44 | −91.54±227.45 | −144.69±244 | −25.31±211.68 |
Expressed as mean and standard deviation.
In Figs. 1–5, the temporal changes in patient plasma calcium (mM), phosphorus (mg/dL), Ca×P product (mg2/dL2), bicarbonate (mM), and pH can be seen graphically, grouped by baseline calcium (above/below 1.16mM) and calcium bath (1.25 or 1.5mM). Below, we describe individually the changes in each of the parameters analysed.
 during haemodialysis sessions. Patients are grouped according to baseline ionised calcium and calcium bath used. 100% of patients dialysed with Ca++ bath of 1.5mM ended the session with plasma levels >1.3mM, independently of the baseline calcaemia, whilst only 15% of those with a Ca++ bath of 1.25mM reached that level (P<.001).")
Temporal changes in plasma ionised calcium (mM) during haemodialysis sessions. Patients are grouped according to baseline ionised calcium and calcium bath used. 100% of patients dialysed with Ca++ bath of 1.5mM ended the session with plasma levels >1.3mM, independently of the baseline calcaemia, whilst only 15% of those with a Ca++ bath of 1.25mM reached that level (P<.001).
 during haemodialysis sessions. Patients are grouped according to baseline calcium and calcium bath used. Changes in phosphorus were independent of the calcium bath used and the baseline calcaemia: there were no significant differences between groups.")
Temporal changes in plasma phosphorus (mg/dL) during haemodialysis sessions. Patients are grouped according to baseline calcium and calcium bath used. Changes in phosphorus were independent of the calcium bath used and the baseline calcaemia: there were no significant differences between groups.
 during haemodialysis sessions. Patients are grouped according to baseline calcium and calcium bath used. Those dialysed with Ca++ bath 1.25mM had final Ca++×P products significantly lower than those of the 1.5mM group (10.1±3.84 vs 13.99±4.41; P=.029). In the 1.25mM group, the reduction in the Ca++×P product was significantly greater (−13.79±7.09 vs −8.74±4.17; P=.04).")
Temporal changes in plasma Ca++×P product (mg2/dL2) during haemodialysis sessions. Patients are grouped according to baseline calcium and calcium bath used. Those dialysed with Ca++ bath 1.25mM had final Ca++×P products significantly lower than those of the 1.5mM group (10.1±3.84 vs 13.99±4.41; P=.029). In the 1.25mM group, the reduction in the Ca++×P product was significantly greater (−13.79±7.09 vs −8.74±4.17; P=.04).
 during haemodialysis sessions. Patients are grouped according to baseline calcium and calcium bath used. Baseline and final values of bicarbonate were independent of the calcium bath used and the baseline calcaemia: there were no significant differences between groups. 50% of patients ended the session with baseline bicarbonate levels >30mM.")
Temporal changes in plasma bicarbonate (mM) during haemodialysis sessions. Patients are grouped according to baseline calcium and calcium bath used. Baseline and final values of bicarbonate were independent of the calcium bath used and the baseline calcaemia: there were no significant differences between groups. 50% of patients ended the session with baseline bicarbonate levels >30mM.

Temporal changes in plasma pH during haemodialysis sessions. Patients are grouped according to baseline calcium and calcium bath used. The baseline and final values were independent of the calcium bath used and the baseline calcaemia: there were no significant differences between groups. Overall, 23% of patients ended the session with pH >7.5.
Independently of the baseline calcium level or calcium bath used, in both groups there was an increase in calcaemia on finishing dialysis (Table 2). Over the course of the session there was a progressive, uniform increase in calcium (Fig. 1), which was significantly higher in the group of patients dialysed with a 1.5mM Ca++ bath than in the 1.25mM group (0.23±0.08 vs 0.08±0.09, P<.001) (Table 3). In the 1.5mM group, 100% of patients finished dialysis with plasma calcium values >1.3mM, independently of the baseline calcaemia, whereas in the 1.25mM group this only happened in 15% (P<.001). The overall calcium increase was significantly higher in patients with a baseline calcium <1.16mM than in those with baseline calcium >1.16mM (0.2±0.11 vs 0.11±0.11, P=.03) (Table 3). Lastly, calcium increase and mean final serum calcium levels were independent of the vascular access used, and of baseline phosphataemia: there were no statistically significant differences between those groups.
PhosphorusThere were no statistically significant differences in baseline phosphorus levels or final phosphorus levels between groups according to the baseline calcium or the calcium bath used (Table 2). During the session, there was a progressive decrease in phosphorus, which was more marked in the first hours of dialysis (Fig. 2). There were no significant differences between groups in the overall phosphorus decrease (Table 3). As previously mentioned, the final serum calcium levels and the calcium increase were independent of baseline phosphorus levels: there were no significant differences between groups (normal range 2.5–4.5mg/dL).
Ca×P productThe baseline calcium phosphorus product was independent of the baseline calcium and calcium bath used: there were no significant differences between groups (Table 2). Over the session, there was a fall in the Ca++×P, which was more marked in the first hour (Fig. 3). Patients dialysed with a 1.25mM Ca++ bath had significantly lower final Ca++×P products than those dialysed with a 1.5mM Ca++ bath (10.1±3.84 vs 13.99±4.41, P=.02). Furthermore, in the 1.25mM group, the overall decrease in the Ca++×P product was significantly greater than in the 1.5mM group (13.79±7.09 vs 8.74±4.17, P=.04) (Table 3).
Bicarbonate and pHThe baseline and final values of bicarbonate and pH were independent of the baseline calcium and calcium bath used; there were no significant differences between groups (Table 2). Over the session, bicarbonate increased progressively (Fig. 4). The pH decreased initially in the first 30min, with subsequent alkalinisation (Fig. 5). Overall, 50% of patients ended the session with bicarbonate levels >30mM and 23% with pH >7.5. The overall increase in bicarbonate and the alkalinisation were similar between groups, independently of the baseline calcium or the calcium bath used (Table 3).
MagnesiumThe baseline and final values of magnesium were independent of the baseline calcium and calcium bath used; there were no significant differences between groups (Table 2). Over the session, there was a homogenous decrease in all groups, with no significant differences between groups (Table 3).
Intact parathyroid hormoneThe baseline and final levels of intact parathyroid hormone (iPTH) were lower in patients dialysed with a 1.5mM calcium bath than with a 1.25mM bath (baseline iPHT 574±379.75 vs 321.15±244.46; P=.05) (final iPHT: 496.23±400.61 vs 223.62±236.18; P=.05) (Table 2). However, there were no differences in the changes in PTH in relation to the calcium bath used or the baseline calcaemia (Tables 2 and 3).
DiscussionIn this study we analysed the changes produced in calcium, phosphorus, magnesium, pH, and bicarbonate, during HD sessions. The induction of alkalinisation, along with the increase in serum calcium in the presence of hyperphosphataemia in the initial phases of HD constitutes a perfect environment for the development of VC.
The physiochemical mechanisms responsible for VC have been studied in vitro. Lomashvili16 demonstrated that the calcification of rat aortas in vitro required increased calcium and phosphorus, but was not related to the calcium–phosphorus product. Also, De Solís et al. observed that calcification was potentiated by alkalinisation in the presence of uraemic serum and even more so with the alkalinisation of the extracellular medium (pH of 7.42–7.53).26 Furthermore, in in vivo studies, aortic calcification was proven to increase significantly in alkalinised animals. This is precisely what occurs during HD and what we have observed in our study. Haemodialysis sessions produce these physiochemical changes, which could be responsible, along with other factors, for the development of VC. It is the “perfect biochemical storm”, with high calcium levels and alkalinisation despite a progressive reduction in the calcium–phosphorus product. In many patients, phosphorus normalisation is not achieved until after 2h of HD, adding another factor as there is hyperphosphataemia in the first hours. What occurs post-dialysis can be considered even more critical, as at 2h there is a phosphorus rebound of up to 40%. To that could be added that the magnesium concentrations used in the dialysis fluid (0.5mM) produce a reduction in serum magnesium values during HD (Tables 2 and 3), which could augment even more this “perfect storm” of calcification during HD sessions. Several studies, both in vitro and in animals, have shown a protective effect of magnesium against VC through multiple mechanisms, and clinical studies also demonstrate evidence of this protective effect of magnesium against VC.28,29
In our study we used dialysis fluid with a concentration of 35mM of bicarbonate, with plasma bicarbonate increasing from 25.35±3.4mM to 29.91±2.16mM and pH from 7.38±0.06 baseline value to 7.47±0.05 final value, with an increase to above 7.50 in 23% of patients (independently of the calcium bath used). These values are similar to, or even higher than, the degree of alkalinisation that led to increased calcification in rat aortas in vitro.16,26 One of the most debatable points of this study is: if the calcium–phosphorus product is reduced during dialysis, why does the idea remain that dialysis induces VC. In the studies by Lomashvili, the concentrations of Ca++ and P were changed inversely to maintain a constant [Ca++]×[P] product, and it was observed that VC increased directly as calcium increased, despite a decrease in phosphorus. That is, calcification is not a function of the calcium–phosphorus product, but depends more on the individual concentrations of calcium and phosphorus.
If the hypothesis of VC during HD is reasonable, we should progress to how to control the physiochemical factors responsible. Or rather, how to avoid the precipitating factors being present at the same time. The first change would relate to the calcium concentration of the dialysis bath. The changes in serum calcium that occur during dialysis depend on the initial serum calcium concentration, the ultrafiltration volume, and the calcium concentration of the dialysis fluid. Calcium kinetics during HD sessions have already been studied by various authors, using different calcium bath concentrations and different HD tecnhiques30,31: serum calcium increased to 1.32 and 1.45mM during HD sessions with dialysis fluid calcium concentrations of 1.25 and 1.5mM, respectively. Conversely, in patients with baseline calcaemia in the normal range, the calcium balance is neutral or negative with dialysis fluid concentrations of 1.25mM.32 However, as in our study, in patients with a low baseline calcium, ionised calcium can increase during dialysis with a 1.25mM concentration. In reality, the KDIGO guidelines suggest a dialysis fluid calcium concentration of between 1.25 and 1.50mM,33 based on the theory that a concentration of 1.25mM means a neutral calcium balance. However, Gotch et al. demonstrated very different results with 2 kinetic models. By analysing calcium transport across the dialyser during dialysis, they observed that each session induced more than 500mg of calcium transport. In the kinetic analysis of intestinal absorption of calcium in 320 patients on HD, the study by Gotch concluded that calcium absorption was strongly dependent on the dose of vitamin D analogues and much less so on ingested calcium. The most important conclusion to relate to our study about possible VC during HD was that 70% of patients who received calcium binders and between 20% and 50% of those who take non-calcium binders required a dialysis fluid calcium concentration lower than 1.25mM to prevent long-term calcium build-up.34,35 However, it must be considered that the concept of calcium gain might not be correct, because plasma calcium is the result of several factors involved in the homeostasis of calcium. Changes in pH modify ionised Ca++, and alkalosis reduces free Ca++ by increasing the binding of Ca++ to albumin. Furthermore, it must be taken into account that PTH releases calcium from bone. In our study we analysed ionised calcium, and therefore the increase did not depend on calcium bound to albumin. Also, since PTH decreased during HD, it would not be responsible for an increase in release of bone calcium, so, in line with the observations of Gotch,34,35 there would be calcium transport during dialysis that could favour the calcification process, although the reduction in phosphorus could have a certain protective effect. All of this means that the calcium concentration in dialysis fluid should be individualised36 and, if we want to avoid calcium gain during the dialysis session, we should also consider measures to increase the intestinal absorption of calcium (oral Ca++ or vitamin D) to maintain a neutral balance.
During HD there is a decrease in plasma phosphorus as it diffuses across the dialyser. This plasma decrease, in conventional HD, leads to a nadir in approximately the first hour; later the phosphorus level is more stable, as seen in our study.37,38 This seems to be due to the kinetics of phosphate in response to the extracellular decrease, depending on the predialysis concentration.39 Therefore, during the first hour and a half, we could individually programme dialysis, so as to avoid calcium gain while serum phosphorus has not yet reached its nadir. If we add to that the absence of alkalinisation with dialysis bath bicarbonate concentrations similar to, or slightly higher than, predialysis concentrations, we would avoid the concurrent combination of “alkalinisation+calcium gain+hyperphosphataemia”, which, combined with a decrease in magnesium is the “perfect storm” for VC.
The hypothesis that the practice of HD sessions can induce VC is also supported by the fact that patients who end up on dialysis have from 2 to 5 times more coronary artery calcification than matched nonrenal patients. Also, as coronary calcification is closely correlated with the number of years on HD, calcification could well be due to long duration of CKD or long treatments with calcification inducers, such as calcium-based phosphate binders or vitamin D compounds.40,41
This study has some weaknesses. The most important weakness is that it was assumed that the biochemical changes that occurred in vitro and in vivo were applicable to patients during HD sessions. Of course, there are biological factors that interfere in the prevention of VC that we have not analysed.42–47 Studies would be required, directed at calcification during the process of HD, in addition to the existing studies on the progression of CKD. Another of the weaknesses of our study is the absence of gasometry. There was a decrease in pH at 15min from starting the session that theoretically could have a protective effect against calcification.27 It is a transient effect, which, coinciding with the increase in bicarbonate, logically is related to pCO2. In studies on respiratory function during HD with bicarbonate, similar changes were found that were explained by a pCO2 increase greater than the bicarbonate increase.48 However, as in our study, those authors also observed a progressive alkalinisation during HD sessions.
In conclusion, in all the studies on VC in patients with CKD, including international guidelines,33 classical and nonclassical factors were analysed, with special emphasis on the active cellular process that occurs, with osteogenic transformation and formation of hydroxyapatite in connection with abnormal calcification-inhibitory factors. Hyperphosphataemia and especially the role of calcium-based phosphate binders in the development of VC form a multitude of articles that defend the use of noncalcium-based binders. However, there is little more in-depth study of the biochemical phenomena that patients experience 156 times per year during HD sessions and that clearly induce calcification: calcium gain in the presence of hyperphosphataemia at the same time as progressive alkalinisation. Therefore, studies are needed that individualise HD according to the characteristics of each patient, especially their baseline calcium and phosphorus. A delay in calcium gain and alkalinisation until serum phosphorus has gone down to normal values during HD sessions could be the first step in modifying this “perfect storm”.
Conflicts of interestThe authors declare no potential conflicts of interest related to the contents of this article.
Please cite this article as: Seras M, Martín de Francisco ÁL, Piñera C, Gundin S, García-Unzueta M, Kislikova M, et al. Sesión de hemodiálisis: la tormenta perfecta para la calcificación vascular. Nefrologia. 2015;35:448–456.



