
We read with interest the case recently published by De la Flor et al. “Efficacy and safety of semaglutide in a diabetic and obese patient on incremental hemodialysis. Does it also contribute to preserving residual renal function?”,1 to which we would like to contribute our experience in incremental peritoneal dialysis (PD).
Diabetic kidney disease is associated with an excessive increase in morbidity and mortality, especially of cardiovascular origin, and also increases progression of CKD.2
Glucagon-like peptide type 1 receptor agonists (GLP-1 ARs) are a family of antihyperglycemic drugs that have demonstrated strong reduction of HbA1c levels, low risk of hypoglycemia, weight reduction and cardiovascular and renal benefits.3 In addition, the authors also describe favorable effects on preservation of residual renal function (RRF) in a patient on incremental hemodialysis.1 However, experience in dialysis patients is limited.4
We present a 71-year-old male with type 2 diabetes mellitus, kidney disease secondary to diabetic nephropathy and repeated episodes of renal stones, arterial hypertension, dyslipidemia and a history of past tobacco use. His body mass index (BMI) was 32.9kg/m2 and his abdominal perimeter, 110cm.
He started PD in 2020 incrementally with two exchanges per day, one of 2000 cc of physioneal® 40 1.36% and one of nocturnal icodextrin; he was in temporary contraindication for kidney transplantation due to grade 1 obesity. Serum creatinine was 6.39mg/dl, glomerular filtration rate (GFR) measured by CKD-EPI was 8ml/min/1.73m2, creatinine clearance (ClCr) and urea clearance (KrU) were 12.2 and 6.1ml/min/1.73m2, respectively, both in 24-h urine; the GFR by mean level of ClCr and KrU was 9.2ml/min/1.73m2 and proteinuria was 1.680mg/24h.
Despite good glycemic control with 18 UI/day of insulin glargine, dulaglutide was added to the treatment due to its effect on weight reduction and to improve metabolic control in PD, with the expectation of making possible renal transplantation. The starting dose was 0.75mg subcutaneously weekly, increasing to 1.5mg/weekly at 1 month, with good tolerance and no hypoglycemia.
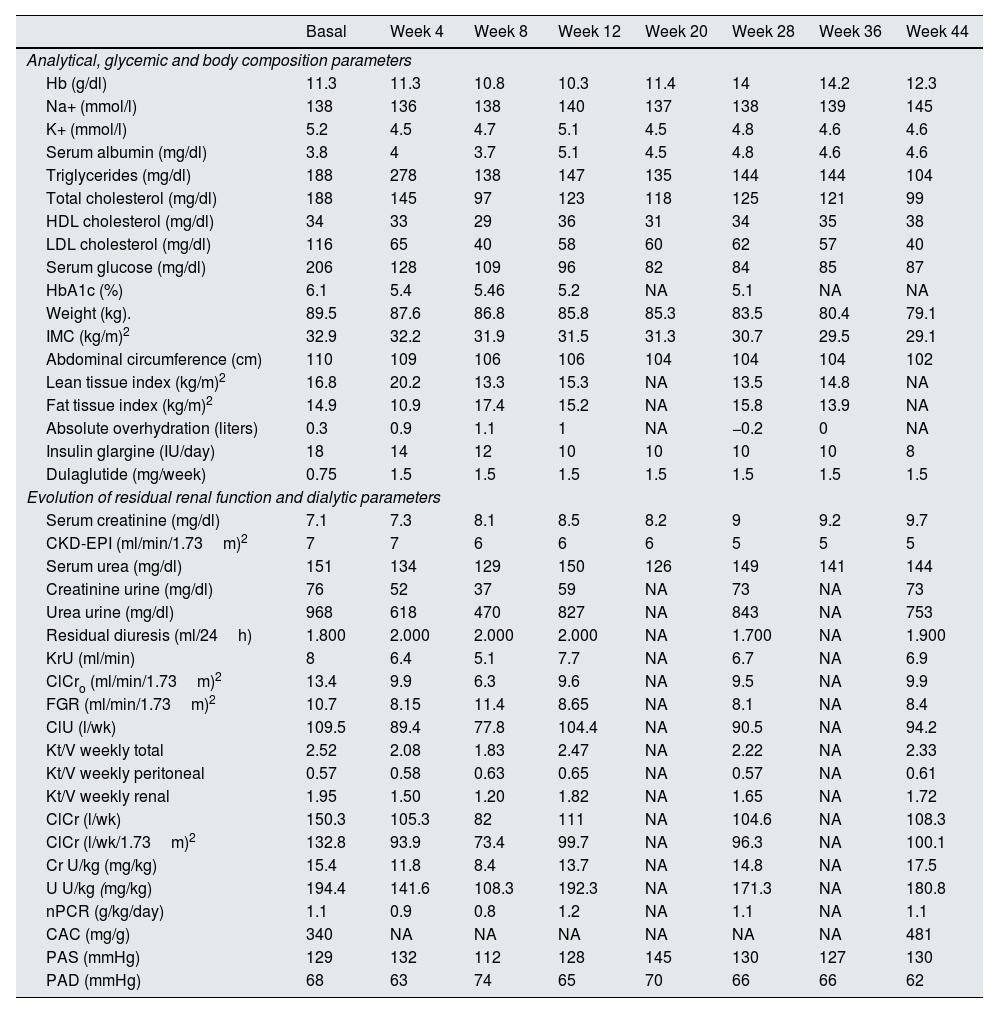
At the beginning of the treatment there were no data for hyperhydration. At 4 weeks there was a significant reduction in the percentage of fat mass (26.8%) and an increase in lean mass (20.2%). At 44 weeks the weight loss was 10.4kg, insulin requirements were reduced by more than 50%, glycated hemoglobin (HbA1c) was reduced by 16.4% and BMI by 11.6%; as for the lipid profile, triglycerides were reduced by 44.7%, total cholesterol by 47.3% and LDL by up to 65.5%. During follow-up, the dose of antihypertensive drugs was reduced, an effect that can probably be attributed to the decrease in weight, as well as the decrease in insulin therapy.
From the renal point of view, diuresis remained around 2L/day. ClCr and KrU initially fell, as did total weekly Kt/V (at the expense mainly of renal Kt/V) to gradually increase throughout the evolution until stabilizing. Urinary creatinine and urea excretion, normalized to kilo of weight, increased from week 12 of treatment. The normalized protein catabolism rate (nPCR) was stable (Table 1). The patient received a kidney transplant 14 months after starting treatment with dulaglutide.
Analytical evolution monitoring and parameters of peritoneal dialysis.
| Basal | Week 4 | Week 8 | Week 12 | Week 20 | Week 28 | Week 36 | Week 44 | |
|---|---|---|---|---|---|---|---|---|
| Analytical, glycemic and body composition parameters | ||||||||
| Hb (g/dl) | 11.3 | 11.3 | 10.8 | 10.3 | 11.4 | 14 | 14.2 | 12.3 |
| Na+ (mmol/l) | 138 | 136 | 138 | 140 | 137 | 138 | 139 | 145 |
| K+ (mmol/l) | 5.2 | 4.5 | 4.7 | 5.1 | 4.5 | 4.8 | 4.6 | 4.6 |
| Serum albumin (mg/dl) | 3.8 | 4 | 3.7 | 5.1 | 4.5 | 4.8 | 4.6 | 4.6 |
| Triglycerides (mg/dl) | 188 | 278 | 138 | 147 | 135 | 144 | 144 | 104 |
| Total cholesterol (mg/dl) | 188 | 145 | 97 | 123 | 118 | 125 | 121 | 99 |
| HDL cholesterol (mg/dl) | 34 | 33 | 29 | 36 | 31 | 34 | 35 | 38 |
| LDL cholesterol (mg/dl) | 116 | 65 | 40 | 58 | 60 | 62 | 57 | 40 |
| Serum glucose (mg/dl) | 206 | 128 | 109 | 96 | 82 | 84 | 85 | 87 |
| HbA1c (%) | 6.1 | 5.4 | 5.46 | 5.2 | NA | 5.1 | NA | NA |
| Weight (kg). | 89.5 | 87.6 | 86.8 | 85.8 | 85.3 | 83.5 | 80.4 | 79.1 |
| IMC (kg/m)2 | 32.9 | 32.2 | 31.9 | 31.5 | 31.3 | 30.7 | 29.5 | 29.1 |
| Abdominal circumference (cm) | 110 | 109 | 106 | 106 | 104 | 104 | 104 | 102 |
| Lean tissue index (kg/m)2 | 16.8 | 20.2 | 13.3 | 15.3 | NA | 13.5 | 14.8 | NA |
| Fat tissue index (kg/m)2 | 14.9 | 10.9 | 17.4 | 15.2 | NA | 15.8 | 13.9 | NA |
| Absolute overhydration (liters) | 0.3 | 0.9 | 1.1 | 1 | NA | −0.2 | 0 | NA |
| Insulin glargine (IU/day) | 18 | 14 | 12 | 10 | 10 | 10 | 10 | 8 |
| Dulaglutide (mg/week) | 0.75 | 1.5 | 1.5 | 1.5 | 1.5 | 1.5 | 1.5 | 1.5 |
| Evolution of residual renal function and dialytic parameters | ||||||||
| Serum creatinine (mg/dl) | 7.1 | 7.3 | 8.1 | 8.5 | 8.2 | 9 | 9.2 | 9.7 |
| CKD-EPI (ml/min/1.73m)2 | 7 | 7 | 6 | 6 | 6 | 5 | 5 | 5 |
| Serum urea (mg/dl) | 151 | 134 | 129 | 150 | 126 | 149 | 141 | 144 |
| Creatinine urine (mg/dl) | 76 | 52 | 37 | 59 | NA | 73 | NA | 73 |
| Urea urine (mg/dl) | 968 | 618 | 470 | 827 | NA | 843 | NA | 753 |
| Residual diuresis (ml/24h) | 1.800 | 2.000 | 2.000 | 2.000 | NA | 1.700 | NA | 1.900 |
| KrU (ml/min) | 8 | 6.4 | 5.1 | 7.7 | NA | 6.7 | NA | 6.9 |
| ClCro (ml/min/1.73m)2 | 13.4 | 9.9 | 6.3 | 9.6 | NA | 9.5 | NA | 9.9 |
| FGR (ml/min/1.73m)2 | 10.7 | 8.15 | 11.4 | 8.65 | NA | 8.1 | NA | 8.4 |
| ClU (l/wk) | 109.5 | 89.4 | 77.8 | 104.4 | NA | 90.5 | NA | 94.2 |
| Kt/V weekly total | 2.52 | 2.08 | 1.83 | 2.47 | NA | 2.22 | NA | 2.33 |
| Kt/V weekly peritoneal | 0.57 | 0.58 | 0.63 | 0.65 | NA | 0.57 | NA | 0.61 |
| Kt/V weekly renal | 1.95 | 1.50 | 1.20 | 1.82 | NA | 1.65 | NA | 1.72 |
| ClCr (l/wk) | 150.3 | 105.3 | 82 | 111 | NA | 104.6 | NA | 108.3 |
| ClCr (l/wk/1.73m)2 | 132.8 | 93.9 | 73.4 | 99.7 | NA | 96.3 | NA | 100.1 |
| Cr U/kg (mg/kg) | 15.4 | 11.8 | 8.4 | 13.7 | NA | 14.8 | NA | 17.5 |
| U U/kg (mg/kg) | 194.4 | 141.6 | 108.3 | 192.3 | NA | 171.3 | NA | 180.8 |
| nPCR (g/kg/day) | 1.1 | 0.9 | 0.8 | 1.2 | NA | 1.1 | NA | 1.1 |
| CAC (mg/g) | 340 | NA | NA | NA | NA | NA | NA | 481 |
| PAS (mmHg) | 129 | 132 | 112 | 128 | 145 | 130 | 127 | 130 |
| PAD (mmHg) | 68 | 63 | 74 | 65 | 70 | 66 | 66 | 62 |
CAC: albumin/creatinine ratio; CKD-EPI: Chronic Kidney Disease Epidemiology Collaboration estimate of glomerular filtration rate; ClCr: creatinine clearance; ClCro: creatinine clearance in 24h urine; ClU: urea clearance; Cr U/kg: urinary creatinine excretion per kilogram of body weight; Hb: hemoglobin; Hb1Ac: glycated hemoglobin; HDL: high-density lipoprotein cholesterol; GFR: glomerular filtration rate; BMI: body mass index; K+: plasma potassium; KrU: renal clearance of residual urea; Kt/V: dialysis treatment efficacy; LDL: low-density lipoprotein cholesterol; NA: not assigned; Na+: plasma sodium; nPCR: normalized protein catabolism rate; SBP: systolic blood pressure; DBP: diastolic blood pressure; U U/kg: urinary urea excretion per kilogram of body weight.
To date, case series have been published with GLP-1 ARs in PD that have proven their efficacy and safety, but to our knowledge there is no previous experience with these drugs in patients on incremental PD or their effect on RRF, which is important.5,6
As described by De la Flor et al.,1 we observed a significant decrease in weight, abdominal perimeter and HbA1c and an improvement in blood pressure control, lipid profile and preservation of RRF. In our group, we consider that RRF brings great benefits to dialysis patients, so we adjusted the dosage of GLP-1 ARs accordingly.7
The 2022 KDIGO (Kidney Disease: Improving Global Outcomes) guidelines on the management of diabetes emphasize the cardiovascular and renal benefits of GLP-1 ARs.2 Weight reduction is a fundamental objective in the nephroprotection of patients with diabetic RD and obesity is an important limitation for inclusion in the renal transplant waiting list.8 On the other hand, preservation of RRF is essential for the survival of the technique in PD.9 In addition to the cardiovascular benefits, GLP-1 ARs can be an excellent treatment option in diabetic and obese patients on PD.
In our experience, dulaglutide has proven to be an effective and safe option in obese diabetic patients on incremental PD with metabolic and RRF benefits.



