





High dietary salt intake was reported to increase blood pressure by numerous studies, but no study has investigated the effect of dietary salt intake on blood pressure variability (BPV). This study aimed to determine if daily salt intake is related to ambulatory BPV. The study included 136 primary hypertensive patients (92 male, 44 female) with a mean age of 50.7±11.1 years. All the patients underwent 24-h ambulatory blood pressure monitoring to determine both the 24-h systolic and 24-h diastolic BPV. 24-h urine sodium was measured. The correlation between BPV and 24-h urinary sodium was investigated. Logarithmic transformation of 24-h urinary sodium [log(24-h urinary sodium)] was positively correlated with the mean 24-h systolic ARV, and nighttime systolic ARV (r=0.371 and p=0.001, r=0.329 and p=0.028, respectively). Similarly, log(24-h urinary sodium) was positively correlated with mean 24-h diastolic ARV and nighttime diastolic ARV (r=0.381 and p=0.001, r=0.320 and p=0.020 respectively). Log(24-h urinary sodium) was an independent predictor of BPV based on multivariate regression analysis. Dietary salt intake might play a role in the pathogenesis of ambulatory BPV.
En numerosos estudios se ha señalado que el consumo elevado de sal aumenta la presión arterial; no obstante, no se ha investigado el efecto de la ingesta alimenticia de sal sobre la variabilidad de la presión arterial (VPA). El objetivo de este estudio fue determinar si el consumo diario de sal está relacionado con la VPA ambulatoria. En el estudio se incluyeron 136 pacientes hipertensos esenciales (92 hombres y 44 mujeres) con una edad media de 50,7±11,1años. Todos los pacientes se sometieron a una monitorización ambulatoria de la presión arterial de 24h para determinar la VPA sistólica y diastólica de 24h. Se midió la natriuria de 24h y se estudió la correlación de la misma con la VPA. La transformación logarítmica de la natriuria de 24h (log [natriuria 24h]) se relacionó con certeza con el índice Average Real Variability (ARV) sistólico de 24h y el ARV sistólico nocturno medios (r=0,371 y p=0,001, r=0,329 y p=0,028, respectivamente). De forma parecida, el log [natriuria 24h] se relacionó con seguridad con el ARV diastólico de 24h y el ARV diastólico nocturno medios (r=0,381 y p=0,001, r=0,320 y p=0,020, respectivamente). El log [natriuria 24h] fue una variable independiente de la VPA, según el análisis de regresión multivariante. Es posible que el consumo de sal intervenga en la patogénesis de la VPA ambulatoria.
Hypertension is a primary risk factor for cardiovascular and cerebrovascular diseases, and renal failure. It is well known that the quantity of dietary salt intake plays a role in the pathogenesis of primary hypertension. Increased sensitivity of blood pressure to excess sodium affects 50% of patients with primary hypertension.1,2 Dietary salt intake causes an increase in blood pressure, and is associated with renal and cardiovascular diseases, including left ventricular hypertrophy and microalbuminuria.3–5 Spontaneous variation in blood pressure is referred to as blood pressure variability (BPV), and is classified as short-term BPV and long-term BPV.6,7 Fluctuation during a 24-h period is referred to as short-term BPV and is based on 24-h ambulatory blood pressure monitoring (ABPM). Variation between successive ABPM measurements is known as average real variability (ARV), which is mathematically calculated.8,9 BPV was reported to be associated with hypertension-related target organ damage and cardiovascular mortality, independent of the blood pressure level. BPV, therefore, becomes more important day-by-day.10–13 The pathophysiology of BPV is not fully known; however, it was reported that short-term BPV is primarily indicative of the effects of central and reflex autonomic modulation, and is associated with humoral, rheological, emotional, and behavioral factors.9,14–18 The relationship between dietary salt intake and ambulatory BPV is not clearly known. Dietary salt intake is known to adversely affect the cardiovascular system, independent of the blood pressure level.3,5 Excretion of sodium in 24-h urine is a measurement with proven validity that is commonly used to measure daily salt intake.19,20 The aim of the present study was to determine if the quantity of daily salt intake is associated with ambulatory BPV.
Materials and methodsStudy populationThis study was performed at Ankara Numune Education and Research Hospital, Nephrology and Internal Medicine Clinic, Ankara, Turkey, and included 136 patients that presented between April 2013 and July 2013, and were diagnosed as primary hypertension. Exclusion criteria were diabetes mellitus, secondary hypertension, pregnancy, body mass index (BMI)>30kg/m2, malignancy, rheumatic diseases, acute/chronic infection, liver disease, thyroid gland disease, adrenal insufficiency, syndrome of inappropriate antidiuretic hormone secretion, nephritis with salt loss, renal tubular acidosis, and a glomerular filtration rate <70mL/min/1.73m2 and diuretic use. Duration of hypertension [years) was calculated based on patient self-reports of the date they were first diagnosed as hypertension to the date of inclusion in the study. The study was conducted in accordance with the Declaration of Helsinki and the study protocol was approved by the Ankara Numune Education and Research Hospital Ethics Committee. All the patients provided written informed consent to participate in the study.
Laboratory proceduresBlood samples were collected at 08.00–10.00, following overnight fasting. Laboratory evaluations included whole blood count, fasting blood glucose, urea, creatinine, sodium, potassium, total protein, and albumin. The GFR was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation: GFR=141×min (Scr/κ,1)α×max(Scr/κ,1)−1.209×0.993age×1.018 [if female]×1.159.21
24-h urine collectionPatients were asked to collect 24-h urine; they were instructed not to save the urine from their first urination the morning they started to collect their urine, and to urinate into a collection container every time thereafter, including the first urination the following morning, and then to bring all collected urine to the laboratory. Patients were told not to make any changes to their daily dietary salt intake and to follow their normal diet during the time of urine collection. Urine sodium was measured in the patients’ 24-h urine via the enzymatic colorimetric method using a Hitachi Modular P800 (Roche Diagnostic Corp. Indiana, USA) autoanalyzer. For each individual the 24-h sodium excretion value (mmol/d) was calculated as the concentration of sodium in the urine (mmol/L)×urinary volume (L/d).
Ambulatory blood pressure monitoring and its variabilityA WatchBP 03 device (Microlife WatchBP AG, Switzerland) was attached to all patients for 24-h ABPM the morning they began to collect 24-h urine. The ABPM device was set to take measurements every 20min between 08.00 and 23.00 (daytime), and every 30min between 23.00 and 08.00 (nighttime). Patients were told to perform their normal daily activities, but not to bend their arm during measurements. These measurements provided 24-h systolic and 24-h diastolic blood pressure values. The method was considered reliable if >70% of measurements were valid. BPV was mathematically calculated as the blood pressure values from 24-h ABPM and the ARV index, using the following formula:ARV=1N−1∑k=1N−1|BPk+1−BPk|where N is the number of valid blood pressure measurements, and BPk+1 and BPk represent 2 successive blood pressure measurements. The rationale for selecting the ARV index for BPV calculation was based on an earlier study that reported the ARV index was a more reliable index for establishing the prognostic significance of BPV.8
Statistical analysisStatistical analysis was performed using SPSS v.20.0 for Windows (SPSS, Inc., Chicago, USA) and STATA/SE v.12.0 for Windows (StataCorp LP, Texas, USA). The Kolmogorov–Smirnov test was used to determine the normality of the distribution of data. Continuous variables with normal distribution are expressed as mean±SD, and continuous variables without normal distribution are expressed as median (range). Categorical variables are presented as number and percentage. Is there was substantial skewing of urinary sodium values, logarithmic transformation (Log) was applied to subordinate the skewness of these values. Continuous variables were compared via the independent samples t-test or the Mann–Whitney U test, as appropriate. Categorical variables were compared using the chi-square test. Relationships between numeric parameters were analyzed via Pearson's and Spearman's correlation analysis. Stepwise multiple linear regression analysis was performed to identify independent determinants of 24-h systolic ARV, 24-h diastolic ARV, nighttime systolic ARV, and nighttime diastolic ARV. The level of statistical significance was set at p<0.05.
ResultsThe study included 136 patients (92 male and 44 female). Mean age of the patients was 50.78±11.1 years. Patient demographic characteristics, and laboratory and ABPM findings are shown in Table 1. BPV and mean 24-h blood pressure levels, and the correlations between other parameters are shown in Table 2.
Demographic, laboratory characteristics and ABPM results of all patients.
| Variables | All populations (n=136) |
|---|---|
| Age (years) | 50.78 (11.1) |
| Gender (n, %) | |
| Male | 92 (67.6) |
| Female | 44 (32.4) |
| BMI (kg/m2) | 29.16 (4.5) |
| Duration of HT (yeras) | 3 (1–20) |
| Anti-hypertensive drug class (n, %) | |
| RAS blocker | 66 (48.5) |
| Beta blocker | 24 (17.6) |
| Calcium channel blocker | 72 (52.9) |
| GFR (mL/min/1.73m2) | 97.57 (10.2) |
| Serum sodium | 141.11 (2.1) |
| Glucose (mg/dL) | 89.94 (5.7) |
| Albumin (g/dL) | 46.28 (2.8) |
| Creatinine (mg/dL) | 0.79 (0.1) |
| Triglyceride(mg/dL) | 157 (61–735) |
| LDL (mg/dL) | 122.52 (35.5) |
| 24-h urine sodium (mmol/d) | 152 (21–387) |
| 24-h urine protein (mg/d) | 89.63 (6–1949) |
| 24-h systolic ARV | 12.33 (3.4) |
| 24-h diastolic ARV | 9.77 (2.6) |
| Nighttime systolic ARV | 11.16 (3.9) |
| Nighttime diastolic ARV | 8.78 (2.9) |
| 24-h SBP (mmHg) | 122.48 (13.2) |
| 24-h DBP (mmHg) | 76.29 (8.50) |
Parameters were expressed as mean±SD or median. Abbreviations: ARV, average real variability; BMI, body mass index; DBP, diastolic blood pressure; GFR, glomerular filtration rate; LDL, low density lipoprotein; SBP, systolic blood pressure; RAS, renin angiotensin system.
The parameters which correlated with diastolic and systolic average real variability.
| Variables | 24-h diastolic ARV | Night diastolic ARV | 24-h systolic ARV | Night systolic ARV | ||||
|---|---|---|---|---|---|---|---|---|
| r | p | r | p | r | p | r | p | |
| Age | 0.092 | 0.287 | 0.036 | 0.675 | 0.046 | 0.591 | 0.034 | 0.697 |
| BMI | 0.222 | 0.009* | 0.114 | 0.188 | 0.156 | 0.071 | 0.135 | 0.117 |
| Duration of HT | −0.037 | 0.677 | −0.110 | 0.220 | 0.091 | 0.310 | 0.014 | 0.876 |
| 24-h SBP | 0.116 | 0.177 | 0.159 | 0.065 | 0.317 | 0.001* | 0.375 | 0.011* |
| 24-h DBP | 0.333 | 0.006* | 0.384 | 0.001* | 0.115 | 0.136 | 0.117 | 0.168 |
| Log(24-h urine sodium) | 0.381 | 0.001* | 0.320 | 0.020* | 0.371 | 0.001* | 0.329 | 0.028* |
| Log(24-h urine sodium)a | 0.338 | 0.004* | 0.315 | 0.031* | 0.342 | 0.002* | 0.323 | 0.025* |
| 24-h urine protein | −0.095 | 0.270 | 0.074 | 0.390 | 0.083 | 0.335 | 0.076 | 0.377 |
| Glucose | 0.048 | 0.661 | 0.175 | 0.110 | 0.074 | 0.501 | 0.114 | 0.299 |
| GFR | 0.164 | 0.066 | −0.029 | 0.740 | 0.109 | 0.064 | 0.008 | 0.925 |
| Albumin | −0.103 | 0.235 | −0.051 | 0.557 | −0.010 | 0.906 | −0.057 | 0.510 |
| Serum Sodium | 0.027 | 0.754 | 0.076 | 0.383 | 0.031 | 0.724 | 0.023 | 0.787 |
| Creatinine | 0.238 | 0.005* | 0.225 | 0.009* | 0.297 | 0.001* | 0.232 | 0.006* |
| Triglyceride | −0.002 | 0.984 | 0.170 | 0.072 | 0.002 | 0.980 | 0.055 | 0.532 |
| LDL | −0.068 | 0.438 | −0.018 | 0.838 | 0.047 | 0.593 | 0.028 | 0.748 |
Abbreviations: ARV, average real variability; BMI, body mass index; DBP, diastolic blood pressure; GFR, glomerular filtration rate; LDL, low-density lipoprotein; SBP, systolic blood pressure.
Systolic blood pressure level was positively correlated with log(24-h urinary sodium) (r=0.294, p=0.024), BMI (r=0.183, p=0.033), creatinine (r=0.226, p=0.008), 24-h systolic ARV (r=0.317, p=0.001), and nighttime systolic ARV (r=0.375, p=0.001).
Diastolic blood pressure level was positively correlated with log(24-h urinary sodium) (r=0.293, p=0.025), BMI (r=0.192, p=0.030), creatinine (r=0.201, p=0.019), 24-h diastolic ARV (r=0.333, p=0.006), and nighttime diastolic ARV (r=0.384, p=0.001).
Mean 24-h systolic ARV, mean nighttime systolic ARV, and mean systolic blood pressure did not significantly differ according gender. Mean 24-h systolic ARV, nighttime systolic ARV, and mean systolic blood pressure did not significantly differ between the patients that did and did not use anti-hypertensive drug.
Mean 24-h diastolic ARV, mean nighttime diastolic ARV blood pressure, and diastolic blood pressure did not significantly differ by gender. Mean 24-h diastolic ARV, mean nighttime diastolic ARV blood pressure, and diastolic blood pressure did not significantly differ between patients that did and did not use anti-hypertensive medication.
In evaluation of all patients for types of antihypertensive drugs used, means of blood pressure levels and ARVs for patients received renin angiotensin system blocker, calcium channel blocker, and beta blocker were similar (p>0.05).
Log(24-h urinary sodium) did not significantly differ according to gender, or anti-hypertensive drug class, and was not associated with other laboratory findings.
The positive correlation between log(24-h urinary sodium) and 24-h systolic ARV, and nighttime systolic ARV, 24-h diastolic ARV, nighttime diastolic ARV persisted when the effect of systolic and diastolic blood pressure levels were adjusted for.
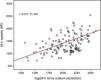
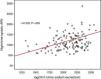
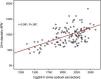
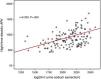
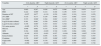
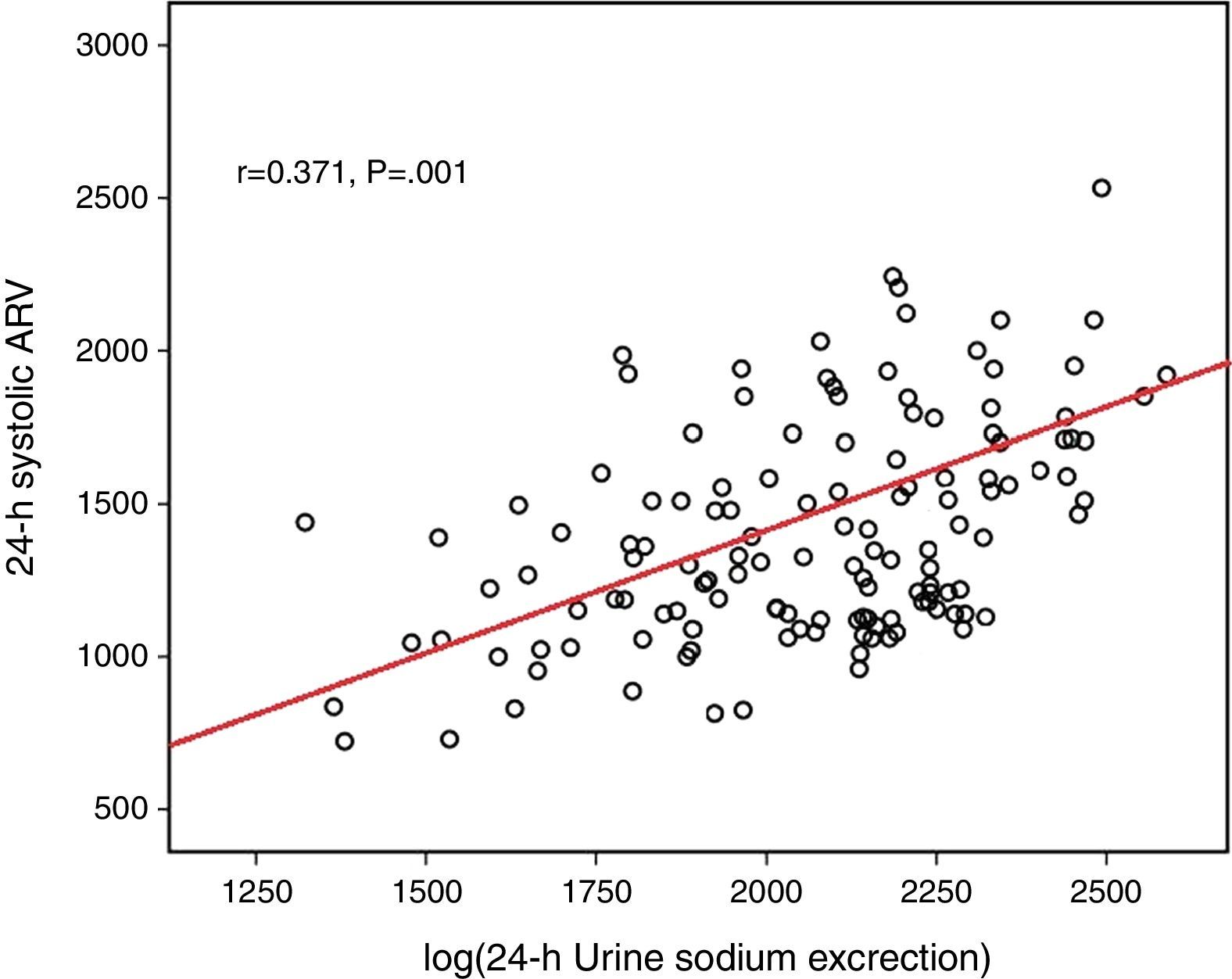
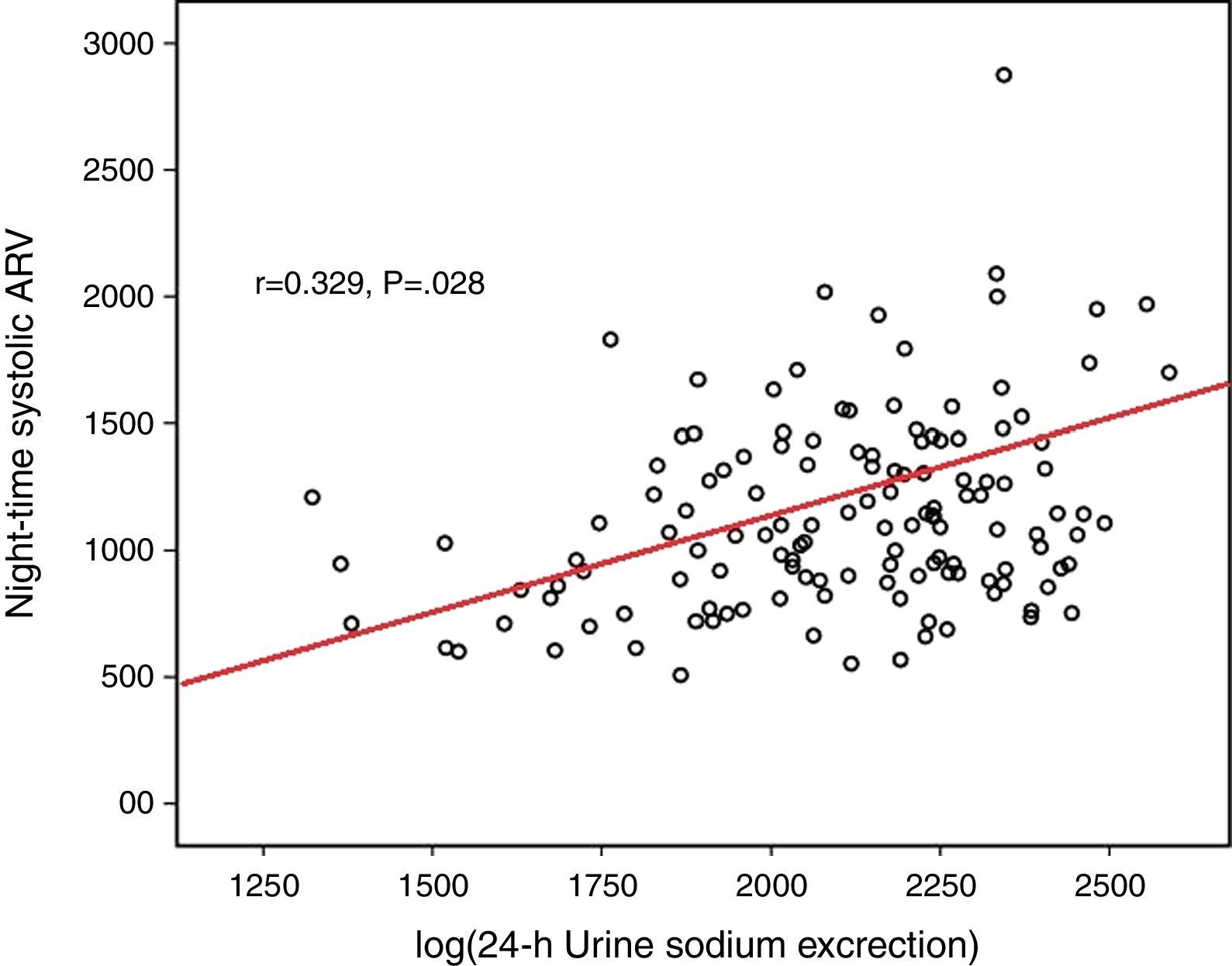
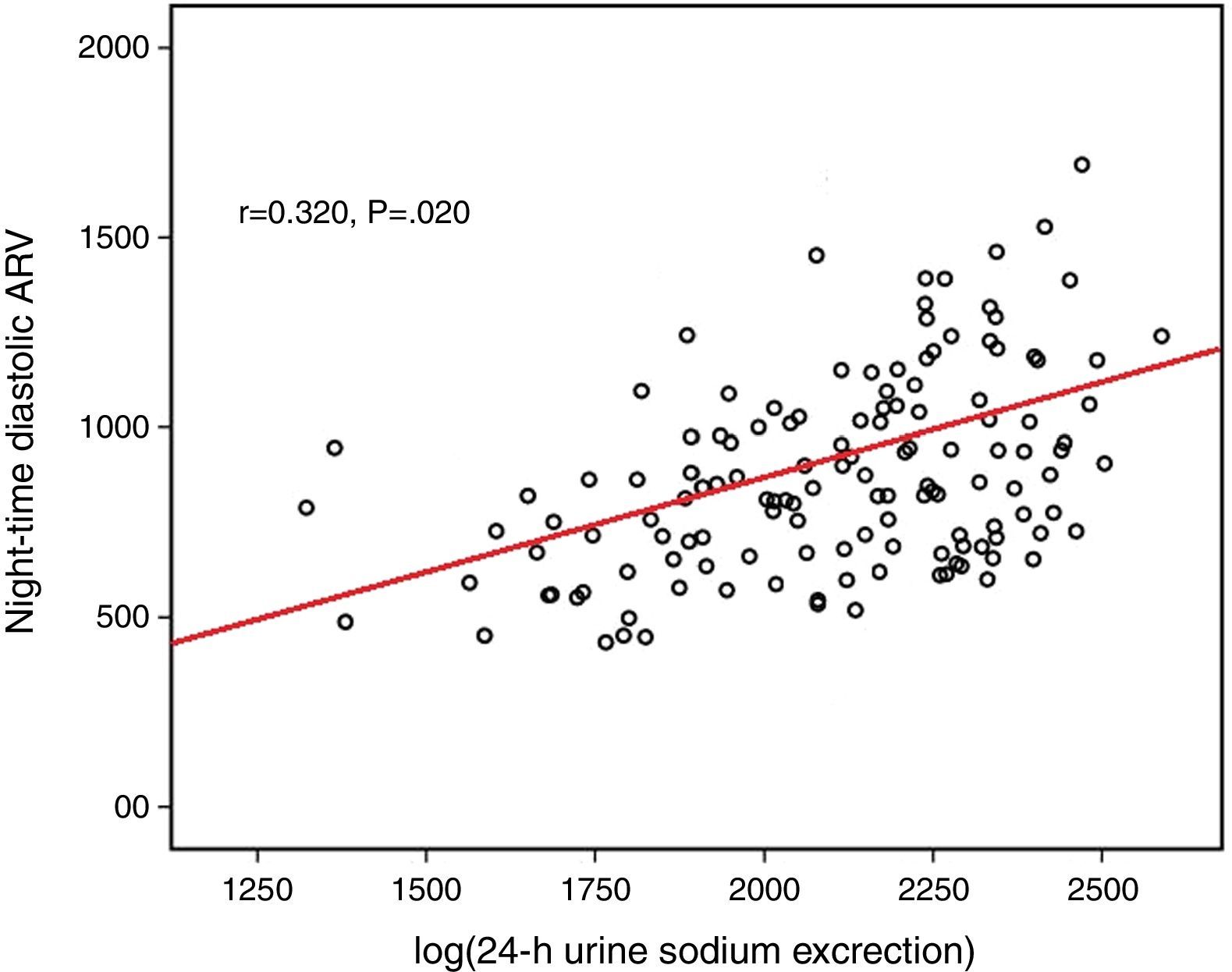
Log(24-h urinary sodium) was positively correlated with mean 24-h systolic ARV and nighttime systolic ARV (r=0.371 and p=0.001, r=0.329 and p=0.028, respectively) (Figs. 1 and 2). Similarly, log(24-h urinary sodium) was positively correlated with mean 24-h diastolic ARV and nighttime diastolic ARV (r=0.381 and p=0.001, r=0.320 and p=0.020, respectively) (Figs. 3 and 4). The positive correlation also persisted when systolic and diastolic blood pressures, gender and BMI were adjusted for.
Age, male gender, BMI, duration of hypertension, and anti-hypertensive drug class, systolic blood pressure, diastolic blood pressure, log(24-h urine sodium), 24-h urine microalbuminuria, 24-h urine protein excretion, glucose, GFR, albumin, serum sodium, creatinine, triglyceride, and LDL levels were included in a stepwise regression model. Log(24-h urine sodium) was observed to be an independent predictor of BPV based on multivariate regression analysis (Table 3).
Independent predictors for average real varibility by multivariate regression analysis.
| Characteristic | B±SE | 95C.I. | p value | ||
|---|---|---|---|---|---|
| 24-h diastolic ARV | R2=0.219, p<0.001 | ||||
| 24-h DBP | 0.043(0.015) | 0.010 | 0.091 | 0.009* | |
| Log(24-h urine sodium) | 2.601(0.852) | 0.916 | 4.285 | 0.003* | |
| Creatinine | 3.435(1.458) | 0.752 | 6.519 | 0.014* | |
| 24-h systolic ARV | R2=0.237, p<0.001 | ||||
| 24-h SBP | 0.054 (0.021) | 0.012 | 0.096 | 0.001* | |
| Log(24-h urine sodium) | 3.390 (1.094) | 1.226 | 5.554 | 0.010* | |
| Creatinine | 5.072 (1.867) | 1.379 | 8.764 | 0.007* | |
| Nighttime diastolic ARV | R2=0.225, p<0.001 | ||||
| 24-h DBP | 0.048 (0.019) | 0.029 | 0.101 | 0.003* | |
| Log(24-h urine sodium) | 2.431 (0.821) | 0.788 | 3.450 | 0.038* | |
| Creatinine | 3.626 (1.733) | 1.119 | 7.053 | 0.028* | |
| Nighttime systolic ARV | R2=0.229, p<0.001 | ||||
| 24-h SBP | 0.059 (0.025) | 0.010 | 0.109 | 0.021* | |
| Log(24-h urine sodium) | 2.462 (0.713) | 1.084 | 5.056 | 0.033* | |
| Creatinine | 4.448 (1.938) | 1.221 | 8.875 | 0.014* | |
Abbreviations: ARV, average real variability; DBP, diastolic blood pressure; SBP, systolic blood pressure.
In the present study there was a positive correlation between the 24-h urine sodium level and 24-h systolic and 24-h diastolic BPV derived from ABPM in patients diagnosed as primary hypertension. In addition, there was a positive correlation between 24-h urine sodium, and mean 24-h systolic and 24-h diastolic blood pressure levels based on ABPM. The effect of the quantity of dietary salt intake on blood pressure has been investigated in numerous epidemiological screening studies, clinical studies, and experimental animal trials1,22–24; however, to the best of our knowledge the present study is the first to investigate the relationship between the quantity of daily salt intake and ambulatory BPV in hypertensive patients.
Dietary salt intake is a rectifiable environmental factor associated with the pathogenesis of primary hypertension. Conclusive evidence shows that high-level dietary salt intake is closely associated with high blood pressure and the development of hypertension-related target organ damage20,24,25; however, many studies report that high dietary sodium intake negatively affects the cardiovascular and cerebrovascular systems, independent of elevated blood pressure.26 It has been suggested that high dietary salt intake adversely affects remodeling in central and peripheral arteries, and increases arterial stiffness, independent of increasing blood pressure.27,28 A study that included normotensive participants reported that sodium excretion in 24-h urine was positively correlated with CIMT, independent of blood pressure, which was suggested to be because a high-salt diet could result in a flow-related increase in shear stress and induce compensatory arterial wall thickening without increasing blood pressure.
Endothelium-dependent vascular function and arterial walls are negatively affected by salt load. These effects of high salt intake on target organs are linked to the fibrogenic activity of transforming growth factor (TGF)-beta1, as TGF-beta1 production has been shown to increase during high salt intake.29 High salt intake also stimulates vascular growth by increasing the response to angiotensin 2, vasopressin, and several growth factors. In general, BPV is considered to occur due to interaction between environmental, behavioral, neural (central or reflex), humoral (insulin, angiotensin II, bradykinin, endothelin-1, and nitric oxide), and myogenic factors14,15,30–32; however, the precise factors responsible for BPV remain unclear. Sympathovagal reflex has been shown to play a role in BPV in healthy individuals.32 Additionally, among the proposed vascular mechanisms of BPV is alteration in arterial distensibility.33 BPV was also associated with changes in arterial blood vessel walls, including a decrease in arterial compliance and an increase in arterial stiffness, in healthy young males and patients with cardiovascular disease.17,31
In the present study the observed correlation between 24-h urine sodium and ambulatory BPV might have been due to the effect of salt on the arterial system. Research has suggested that salt-sensitive hypertension was associated with the autonomic nervous system, and that the sympathetic nervous system was hyperactivated and the parasympathetic system was inhibited in such patients.34 These findings are consistent with experimental animal studies in which the blood pressure in rats decreased following sympathetic current blockade or severing of sympathetic nerves.35,36
The central nervous system is suggested to play an important role in producing and maintaining high blood pressure in individuals with salt-sensitive hypertension. Central and reflex autonomic modulation is known to play a role in the pathophysiology of BPV. Rat studies showed that BPV was associated with reduced cardiac baroreflex.37 A study on the association between BPV and daily salt intake in normotensive individuals reported that dietary salt intake negatively affected centrally mediated cardiovascular reflex, resulting in an increase in BPV. Several studies reported that BPV is regulated by sympathovagal balance and arterial distensibility.2–4 Based on these findings, several mechanisms might contribute to increased BPV in hypertensive patients with a high-salt diet. Increased BPV might be partially due to diminished baroreflex function associated with increased stiffness and reduced compliance in large elastic arteries.26,27 Dietary salt intake might directly regulate or activate sympathetic nerve activity, and might indirectly modulate BPV; however, the cross-sectional design of the present study limits the ability to conclude that there is a causal relationship between salt intake and BPV.
In conclusion, the major finding of the present study is that primary hypertensive patients with high dietary salt intake had high BPV. The relationship between high salt intake and an increase in BPV was independent of the blood pressure level. These findings suggest that under similar blood pressure levels high salt intake may be associated with increased BPV. Additional larger-scale prospective studies are needed to further clarify the relationship between salt intake, BPV, and cardiovascular disease. Patients with a high-salt diet could be at increased risk for cardiovascular disease due to the adverse effects of BPV on the cardiovascular system. High dietary salt intake in hypertensive patients can result in elevated blood pressure and might contribute to cardiovascular morbidity due to an increase in blood pressure.
Financial disclosureNone to declare.
Conflicts of interestThe authors report no conflicts of interest.
None.



