


Chronic kidney disease (CKD) is one of the most common noncommunicable diseases worldwide.1 Aging is one of the nonmodifiable risk factors for its development2–4 mainly because its association with the increase of presence of risk factors for CKD, a situation that results in a high prevalence of this disease in elderlies.5
The epidemiology and disease burden of CKD in elderly adults (EA) has been little researched in Peru, although this population group represented almost 10% of the population in 2016.6 A population study undertaken in two regions of Peru discovered an incidence rate of 16.8%, with more occurrences in adults aged over 65 years.7
In this regard, we aimed to estimate and compare the mortality rates specific to CKD in the elderly adult population of Peru by region and to determine the conditions related to the access to hemodialysis (HD) in the public health system.
A secondary analysis of the National Death Registry for the years 2009–2013, provided by the Office of General Statistics and Digital Records of the Peru's Ministry of Health (MINSA), was conducted. The registries included all the deaths of EA Peruvians with the codes N18.0–N18.9 of the tenth version of the International Statistical Classification of Diseases (CIE-10) according to region of residence. HD access for patients with CKD was evaluated according to the information provided by the Fondo Intangible Solidario de Salud (FISSAL, the largest public financer in Peru for high-cost diseases), including the number of health facilities that subscribed to the agreement for the financing of HD, the number of patients served by this fund, and the number of public facilities by region equipped with HD service during the year 2015. The 2012 Human Development Index and the 2013 Gross Domestic Product (GDP) by region were obtained using the portals of the United Nations Program for Development and the Instituto Nacional de Estadística e Informática (INEI), respectively, to understand the relationship between socioeconomic indicators and CKD. The statistics software used for obtaining specific regional death rates was Stata 14.1 (StataCorp LP, TX, USA). The rates were adjusted by sex and expressed for each 10,000 EA in each of the 25 political administrative regions of Peru by year.
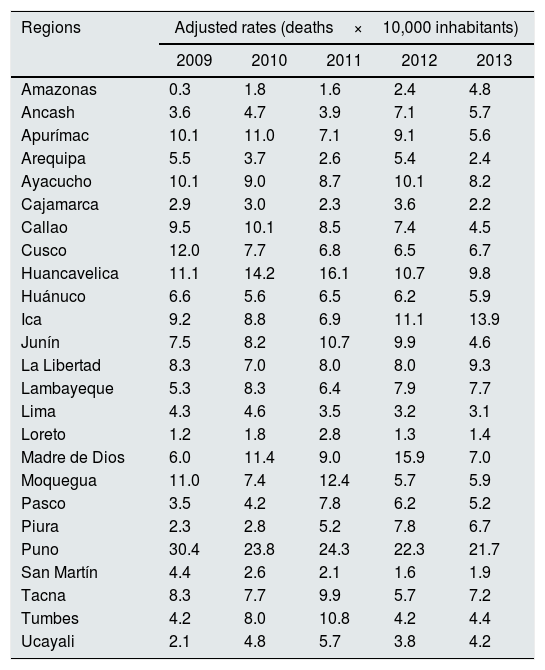
During the period of 2009–2013, 195,938 EA deaths were registered, of which 8175 cases (2.4%) were caused by CKD. Variability in the adjusted death rates was observed for CKD, showing higher and lower rates in different regions of Peru. The highest death rates were seen in 2009 in the Puno (30.4), Cusco (12.0), and Huancavelica (11.1) regions and in 2013 in the Puno (21.7), Ica (13.9), and Huancavelica (9.8) regions. The regions in the Andean zone of the country exhibited the highest CKD death rates during the range of years studied (Table 1). In this respect, a report from MINSA indicates that during the years 2000–2012, the Puno, Apurímac, Cusco, Ayacucho, and Moquegua regions exhibited the highest death rates, matching the results of the present study.8
Adjusted mortality rates according to region of Peru for elderly adults due to chronic kidney disease according to sex, 2009–2013.
| Regions | Adjusted rates (deaths×10,000 inhabitants) | ||||
|---|---|---|---|---|---|
| 2009 | 2010 | 2011 | 2012 | 2013 | |
| Amazonas | 0.3 | 1.8 | 1.6 | 2.4 | 4.8 |
| Ancash | 3.6 | 4.7 | 3.9 | 7.1 | 5.7 |
| Apurímac | 10.1 | 11.0 | 7.1 | 9.1 | 5.6 |
| Arequipa | 5.5 | 3.7 | 2.6 | 5.4 | 2.4 |
| Ayacucho | 10.1 | 9.0 | 8.7 | 10.1 | 8.2 |
| Cajamarca | 2.9 | 3.0 | 2.3 | 3.6 | 2.2 |
| Callao | 9.5 | 10.1 | 8.5 | 7.4 | 4.5 |
| Cusco | 12.0 | 7.7 | 6.8 | 6.5 | 6.7 |
| Huancavelica | 11.1 | 14.2 | 16.1 | 10.7 | 9.8 |
| Huánuco | 6.6 | 5.6 | 6.5 | 6.2 | 5.9 |
| Ica | 9.2 | 8.8 | 6.9 | 11.1 | 13.9 |
| Junín | 7.5 | 8.2 | 10.7 | 9.9 | 4.6 |
| La Libertad | 8.3 | 7.0 | 8.0 | 8.0 | 9.3 |
| Lambayeque | 5.3 | 8.3 | 6.4 | 7.9 | 7.7 |
| Lima | 4.3 | 4.6 | 3.5 | 3.2 | 3.1 |
| Loreto | 1.2 | 1.8 | 2.8 | 1.3 | 1.4 |
| Madre de Dios | 6.0 | 11.4 | 9.0 | 15.9 | 7.0 |
| Moquegua | 11.0 | 7.4 | 12.4 | 5.7 | 5.9 |
| Pasco | 3.5 | 4.2 | 7.8 | 6.2 | 5.2 |
| Piura | 2.3 | 2.8 | 5.2 | 7.8 | 6.7 |
| Puno | 30.4 | 23.8 | 24.3 | 22.3 | 21.7 |
| San Martín | 4.4 | 2.6 | 2.1 | 1.6 | 1.9 |
| Tacna | 8.3 | 7.7 | 9.9 | 5.7 | 7.2 |
| Tumbes | 4.2 | 8.0 | 10.8 | 4.2 | 4.4 |
| Ucayali | 2.1 | 4.8 | 5.7 | 3.8 | 4.2 |
Source: Compiled by the authors based on national death rates from the Office of General Statistics and Digital Records of the Ministry of Health of Peru.
Less than half of the regions of the countries (10 of 25) were equipped with health facilities offering HD services functioning under FISSAL, and most of the facilities having HD were located in regions in the coastal zone of Peru, which is characterized by its higher level of economic development. Most of the patients served with FISSAL coverage lived in coastal regions of the country such as Lima, Callao, and Lambayeque. Regarding GDP and IDH, in general, a correspondence was seen between higher levels of these indicators and a greater number of hospitals and medical centers covered by FISSAL, which offered HD service (Table 2).
Elderly adult population, mortality, socioeconomic indicators, and offer of hemodialysis services related to chronic kidney disease in Peru, according to the region.
| Regions | EA population 2013 | CKD EA death rates 2013a | HDI 2012 | GDP per capita 2013 | HD centers for FISSAL 2015 | HD care for EA FISSAL 2015 | MINSA hospitals offering HD care 2015 |
|---|---|---|---|---|---|---|---|
| Amazonas | 32,915 | 4.8 | 0.38 | 7689 | 0 | 0 | 1 |
| Ancash | 112,999 | 5.7 | 0.44 | 17,723 | 2 | 0 | 3 |
| Apurímac | 39,087 | 5.6 | 0.34 | 6427 | 0 | 0 | 2 |
| Arequipa | 133,456 | 2.4 | 0.58 | 21,087 | 2 | 96 | 3 |
| Ayacucho | 52,330 | 8.2 | 0.33 | 9559 | 0 | 0 | 1 |
| Cajamarca | 120,217 | 2.2 | 0.38 | 9854 | 1 | 3 | 1 |
| Callao | 101,960 | 4.5 | 0.59 | 22,655 | 1 | 156 | 3 |
| Cusco | 119,115 | 6.7 | 0.44 | 19,196 | 1 | 71 | 2 |
| Huancavelica | 32,079 | 9.8 | 0.30 | 7963 | 0 | 0 | 1 |
| Huánuco | 66,541 | 5.9 | 0.37 | 6624 | 1 | 45 | 1 |
| Ica | 77,140 | 13.9 | 0.54 | 23,359 | 0 | 82 | 2 |
| Junín | 113,712 | 4.6 | 0.45 | 9548 | 0 | 0 | 4 |
| La Libertad | 170,586 | 9.3 | 0.47 | 13,651 | 0 | 0 | 3 |
| Lambayeque | 108,291 | 7.7 | 0.46 | 9872 | 4 | 151 | 2 |
| Lima | 994,208 | 3.1 | 0.63 | 22,655 | 23 | 614 | 23 |
| Loreto | 63,398 | 1.4 | 0.40 | 10,080 | 0 | 33 | 2 |
| Madre de Dios | 6323 | 7.0 | 0.56 | 24,381 | 0 | 4 | 1 |
| Moquegua | 18,735 | 5.9 | 0.62 | 51,293 | 0 | 0 | 1 |
| Pasco | 20,462 | 5.2 | 0.41 | 17,597 | 0 | 0 | 0 |
| Piura | 153,207 | 6.7 | 0.44 | 12,316 | 6 | 23 | 2 |
| Puno | 126,681 | 21.7 | 0.39 | 7847 | 0 | 0 | 2 |
| San Martín | 53,850 | 1.9 | 0.44 | 6892 | 1 | 10 | 1 |
| Tacna | 26,973 | 7.2 | 0.56 | 18,652 | 0 | 0 | 1 |
| Tumbes | 15,934 | 4.4 | 0.52 | 12,704 | 0 | 0 | 1 |
| Ucayali | 33,655 | 4.2 | 0.43 | 9548 | 0 | 21 | 2 |
HD: hemodialysis; FISSAL: Intangible Solidarity Health Fund; MINSA: Peru's Ministry of Health; CKD: chronic kidney disease; EA: elderly adults; HDI: human development index; GDP: gross domestic product.
In sum, a high CKD death rate exists among EA in Peru. This rate is higher in the andean zone of the country, which is characterized by a low availability of HD services. The supply of adequate access to renal replacement therapies, including HD, requires that several important points be dealt with to benefit a growing population group in which multiple comorbidities are also present. The variability analysis of the death rates may be useful for focusing on taking action in the area of public health in those regions exhibiting a sustained increase in CKD mortality and providing reinforcement in those regions where it remains the same or is decreasing.
Authors’ contributionsGBQ and AHV participated in the conception, study design, data collection, quality control and data analysis. All the authors participated in the interpretation of the data, writing, review and approval of the final version of the manuscript.
FundingSelf-financed.



