









The aims of the study were to determine the percentage of patients on regular hemodialysis (HD) in Serbia failing to meet KDOQI guidelines targets and find out factors associated with the risk of time to death and the association between guidelines adherence and patient outcome.
MethodsA cohort of 2153 patients on regular HD in 24 centers (55.7% of overall HD population) in Serbia were followed from January 2010 to December 2012. The percentage of patients failing to meet KDOQI guidelines targets of dialysis dose (Kt/V>1.2), hemoglobin (>110g/L), serum phosphorus (1.1–1.8mmol/L), calcium (2.1–2.4mmol/L) and iPTH (150–300pg/mL) was determined. Cox proportional hazards analysis was used to select variables significantly associated with the risk of time to death.
ResultsThe patients were on regular HD for 5.3±5.3 years, dialyzed 11.8±1.9h/week. Kt/V<1.2 had 42.4% of patients, hemoglobin <110g/L had 66.1%, s-phosphorus <1.1mmol/L had 21.7% and >1.8mmol/L 28.6%, s-calcium <2.1mmol/L had 11.7% and >2.4mmol/L 25.3%, iPTH <150pg/mL had 40% and >300pg/mL 39.7% of patients. Using Cox model (adjustment for patient age, gender, duration of HD treatment) age, duration of HD treatment, hemoglobin, iPTH and diabetic nephropathy were selected as significant independent predictors of time to death. When targets of five examined parameters were included in Cox model, target for KtV, hemoglobin and iPTH were found to be significant independent predictors of time to death.
ConclusionSubstantial proportion of patients examined failed to meet KDOQI guidelines targets. The relative risk of time to death was associated with being outside the targets for Kt/V, hemoglobin and iPTH.
Los objetivos del estudio fueron determinar el porcentaje de pacientes en tratamiento de hemodiálisis (HD) regular de Serbia en los que no se alcanzaron los objetivos de la guía KDOQI y determinar los factores asociados al riesgo de tiempo hasta la muerte, así como la asociación entre el cumplimiento de la guía y los resultados clínicos.
MétodosSe llevó a cabo un seguimiento de una cohorte de 2153 pacientes en HD regular de 24 centros de Serbia (un 55,7% de la población total en HD) entre enero de 2010 y diciembre de 2012. Se determinó el porcentaje de pacientes que no alcanzaron los objetivos establecidos en la guía KDOQI respecto a dosis de diálisis (Kt/V>1,2), hemoglobina (>110 g/L), fósforo en suero (1,1-1,8 mmol/L), calcio (2,1-2,4 mmol/L) e iPTH (150-300 pg/mL). Se utilizó un modelo de riesgos proporcionales de Cox para identificar las variables con una asociación significativa con el riesgo de tiempo hasta la muerte.
ResultadosLos pacientes habían estado en HD regular durante un periodo de 5,3±5,3 años, con un tiempo de diálisis de 11,8±1,9 horas/semana. Se observaron valores de Kt/V <1,2 en el 42,4% de los pacientes, hemoglobina <110 g/L en el 66,1%, fósforo en suero <1,1 mmol/L en el 21,7% y >1,8 mmol/L en el 28,6%, calcio en suero <2,1 mmol/l en el 11,7% y >2,4 mmol/L en el 25,3%, iPTH <150 pg/mL en el 40% y >300 pg/mL en el 39,7%. Con el empleo de un modelo de Cox (con ajuste respecto a edad del paciente, sexo y duración del tratamiento de HD) se seleccionaron las variables de edad, duración del tratamiento de HD, hemoglobina, iPTH y nefropatía diabética como factores predictivos independientes significativos del tiempo hasta la muerte. Al introducir los objetivos de los cinco parámetros examinados en un modelo de Cox, se observó que los objetivos de KtV, hemoglobina e iPTH eran factores predictivos independientes para el tiempo hasta la muerte.
ConclusiónUna parte sustancial de los pacientes examinados no alcanzaron los objetivos establecidos en la guía KDOQI. El riesgo relativo del tiempo hasta la muerte se asoció al hecho de no estar en el objetivo de Kt/V, hemoglobina e iPTH.
In the last few decades many guidelines for hemodialysis (HD) based on published evidence were developed by national and international associations.1–3 They defined standards of dialysis with the aim to improve results of HD treatment and patient outcomes. The publication of these guidelines was followed by a number of studies on the levels of guideline adherence. Most of these studies were carried out in developed countries with similar treatment options.4–8 Data about developing countries are insufficient.
In the previous decade, conditions for HD in Serbia have been considerably improved: new equipment for HD and reverse osmosis has been provided, synthetic membranes are used exclusively and agents for treatment of anemia and mineral metabolism disorders became more accessible. In the recent cross section study we showed that these more favorable dialysis treatment have brought about significant improvement in the treatment results.9 However, the guidelines adherence in our country and its comparison with those in developed country as well as the impact of guidelines adherence on patients’ outcome have not been studied.
In the present study a cohort of 2153 patients on regular HD in Serbia were examined with the aim to determine the percent of patients failing to meet KDOQI guidelines targets in five crucial HD practice areas: dialysis dose, anemia, serum phosphorus, serum calcium and iPTH. The second aim was to find out variables significantly associated with the risk of time to death and to examine the association of guideline adherence and patient outcome.
MethodsThe current study analyzed data of 2153 patients on regular HD in 24 centers in Serbia. Data were collected using a questionnaire sent to all 46 HD centers in Serbia with totally 3868 HD patients. The 24 centers responded and sent the data on all patients aged 18 years or older who were on regular HD for more than 3 months on January 1st 2010. Out of 2281 patients whose data were obtained 2153 (833 females, aged 18–90 years) with complete data were included in the study. The study was approved by The Ethics Committee of Zvezdara University Medical Center and appropriate patient consent was obtained at all study centers.
The majority of patients were on conventional HD and 340 on hemodialfiltration. Usually, patients were dialyzed three times weekly for 4h using dialyzers with polysulfone membrane mainly 1.3m2 up to 1.6m2. In all patients the bicarbonate dialysis solution was used containing 138mmol/L sodium, 2 or 3mmol/L potassium, 1.5–1.75mmol/L calcium, 0.5mmol/L magnesium, 1g/L glucose and bicarbonate 35mmol/L and dialysate flow was 500ml/min. Hemodiafiltration was performed using a volume-controlled dialysis machine with optional online-HDF mode (4008H, Fresenius Medical Care, Bad Homburg, Germany).
Vascular access was arteriovenous (AV) fistula in 1940 (90.1%) patients, AV graft in 65 (3.0%) of patients, tunneled central venous catheter in 67 (3.1%) and non-tunneled catheter in 82 (3.8%) of patients.
Hemoglobin, serum levels of urea, phosphorus, calcium, and albumin were measured by routine laboratory tests and iPTH by chemiluminescence essay (Diagnostic Product Corporation, USA). Measured calcium was corrected for level of serum albumin with the following formula: corrected total calcium (mmol/L)=TCa (mmol/L)+0.8 [40 (g/L)−albumin (g/L)]. Dialysis dose (spKt/V) was calculated from values of blood urea nitrogen pre- and post-dialysis, body weight, and dialysis duration using the second generation Daugirdas formula.10 Patients were followed from enrollment until their death, kidney transplantation, departure from the center or the end of the study on December 31, 2012.
Data on patient demographic characteristics, medical history, HD treatment and laboratory data were obtained from medical records at the onset of the study. Based on these data the percentage of patients whose values failed to meet the targets recommended by KDOQI Clinical Practice Guidelines1 was calculated in the following areas: dialysis dose (spKt/V>1.2), anemia (hemoglobin >110g/L), serum phosphorus (1.1–1.8mmol/L), serum calcium (2.1–2.4mmol/L) and plasma iPTH (150–300pg/mL).
Descriptive statistics were presented as mean values and standard deviation (SD) for the continuous variables, or as frequencies for categorical variables. Pearson correlation coefficients were used to detect correlation among variables. Univariate Cox proportional hazards analysis was used to select variables significantly associated with the risk of time to death. As independent variables patient age, gender, primary kidney disease, type of dialysis (HD – low-flux, high-flux, hemodiafiltration), duration of HD treatment (years), HD hours/week, Kt/V, hemoglobin, serum calcium, phosphorus, iPTH, systolic blood pressure, interdialytic weight gain, iron therapy, blood transfusion, use of phosphate binders, use of calcitriol were used. Variables: number of HD weekly, erythropoietin stimulating agents (ESA) dose/week, duration of Epo treatment (years), product of calcium and phosphorus were not included in analysis due to colinearity. Significant variables in univariate analysis (p<0.10) were tested in a multivariate Cox models using the backward stepwise method. The p values of less than 0.05 were considered as statistically significant. Models were adjusted for patient age, gender and duration of HD treatment (years).
All analyses were performed using the SPSS statistical software package (Version 10; SPSS). IBM Corp. Released 2012. IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp.
ResultsThe study involved 2153 patients with mean age of 59 years, but 436 (20.3%) patients were older than 70 years. Characteristics of patients and HD treatment at the onset of the study are presented in Table 1. Patients were on regular HD treatment for averagely 5.3 years and the most frequent cause of end-stage renal disease was hypertension. Dialyzers with polysulfone membranes were used in all patients: low-flux dialyzers in 29.8%, high-flux dialyzers in 54.4% and 15.7% of patients were on hemodiafiltration. Mean HD duration per week was 11.8h and majority of patients had 12 and more hours dialysis weekly (84.5%), but 213 (9.9%) of patients had less than 9h of HD weekly.
Characteristics of patients and hemodialysis treatment at the onset of the study.
| Number | 2153 |
| Gender | |
| Males | 1320 (61.3%) |
| Females | 833 (38.7%) |
| Age, years | |
| Range | 18–90 |
| Mean±SD | 59.0±12.5 |
| >70 years | 436 (20.3%) |
| Diagnosis | |
| Glomerulonephritis | 370 (18.4) |
| TIN (without Balkan nephropathy) | 117 (5.8) |
| Balkan nephropathy | 90 (4.5) |
| Hypertensive nephropathy | 540 (26.8) |
| Diabetic nephropathy | 276 (13.7) |
| Polycystic kidney disease | 168 (8.4) |
| Other | 253 (12.6) |
| Unknown | 195 (9.7) |
| Blood pressure, mmHg | |
| Systolic | 136±21 |
| Diastolic | 77±10 |
| Vintage, years | |
| Range | 0.5–35 |
| Mean±SD | 5.3±5.3 |
| Dialysis treatment | |
| Low-flux dialyzers | 642 (29.8%) |
| High-flux dialyzers | 1171 (54.4%) |
| Hemodiafiltration | 340 (15.8%) |
| Dialysis hours/week | 2.9±0.3 |
| Dialysis time | 11.8±1.9 |
| <9h/week | 213 (9.9%) |
| 9–12h/week | 119 (5.5%) |
| 12h/week | 1585 (73.6%) |
| >12h/week | 236 (10.9%) |
| ID weight gain, kg | |
| Range | 0–9 |
| Mean±SD | 2.8±1.1 |
ID – interdialytic.
Mean values (SD) are presented for continuous variables.
Table 2 shows that 65.1% of patients were treated with ESA, most of them with epoetin and 378 (17.6%) with darbepoetin alpha. Intravenous iron was used in 34.7% of patients and 13.7% patients received blood transfusions when it was necessary. At the onset of the study mean (SD) hemoglobin level was 102 (17) g/L, serum ferritin level 591.4 (557.5) ng/mL and transferrin saturation 30.2 (16.1)%. Phosphate binders were used by 95% of patients and it was mainly calcium carbonate in the mean daily dose of 3.15g±1.59g.
Treatment of anemia and mineral metabolism disorders.
| Iron, number (%) of treated patients | Phosphate binders, number (%)of treated patients | ||
| Oral | 247 (11.5%) | CaCO3 | 1602 (74.4%) |
| i.v. | 747 (34.7%) | Other | 108 (20.6%) |
| ESA use, number (%) | 1402a (65.1%) | Not treated | 443 (5.0%) |
| ESA dosage, U/week (mean±SD)a | 3574±2601 | Vitamin D3, number (%)of treated patients | |
| Transfusion | One-alphaD3 | 603 (28.0%) | |
| Number of patients receiving | 296 (13.7%) | 1,25 D3 | 349 (16.2%) |
| Units/year | 0.72±2.44 | Not treated | 1201 (55.8%) |
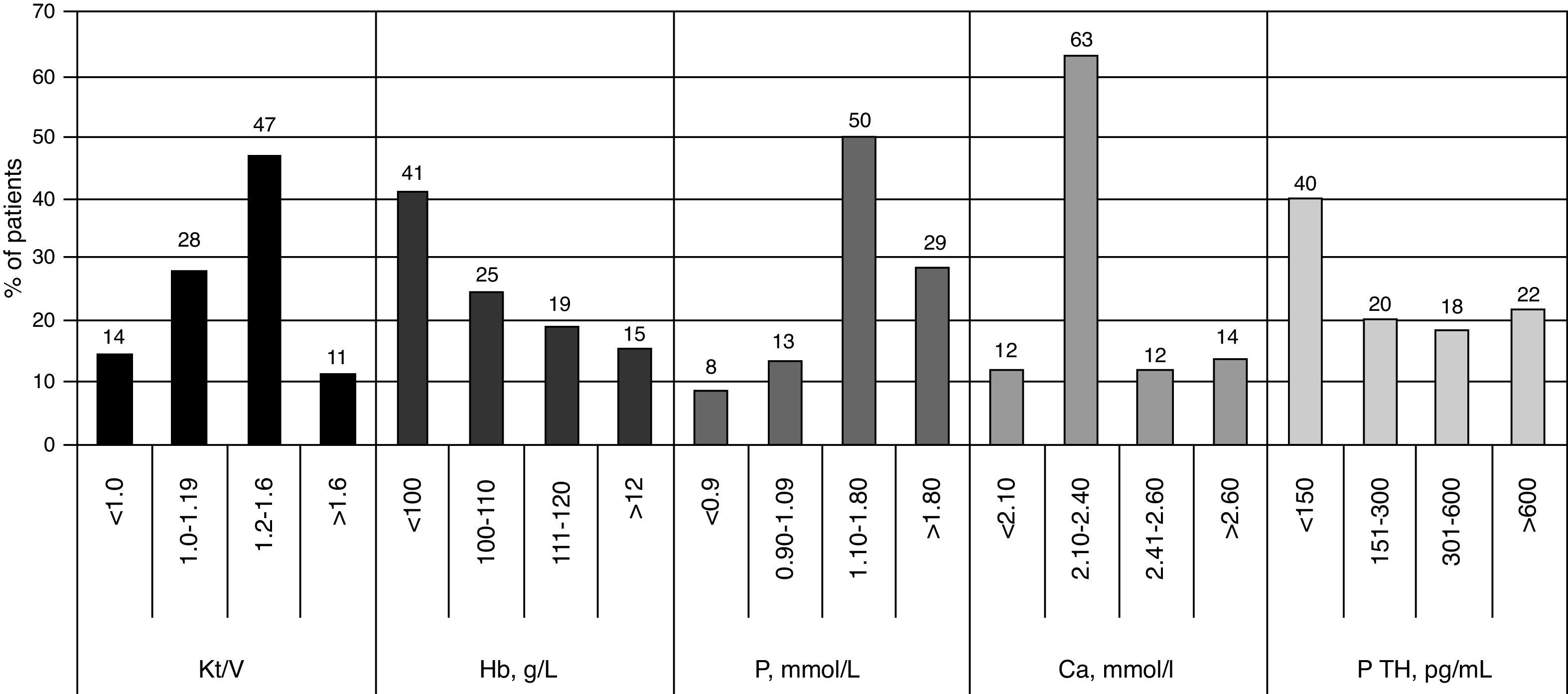
Results presented in Table 3 show that mean values of Kt/V, serum phosphorus and calcium levels and calcium-phosphorus product were in guidelines target ranges. On the other hand, substantial percentage of patients was outside guidelines targets and this percentage was the lowest for calcium-phosphorus product and the highest for serum iPTH level. Fig. 1 shows that among patients with individual values outside guidelines targets there were 14.4% of patients with Kt/V below 1.0, 41.4% patients with hemoglobin below 100g/L, 13.6% of patients with serum calcium above 2.6mmol/L and 21.5% of patients with iPTH above 600pg/mL.
Mean values (±SD) and ranges of variables examined and proportion of patients outside guidelines targets at the onset of the study.
| Single pool Kt/V | |
| Range | 0.64–2.84 |
| Mean±SD | 1.24±0.31 |
| <1.2, no. (%) of patients | 912 (42.4) |
| Hemoglobin, g/l | |
| Range | 55–142 |
| Mean±SD | 102±17 |
| <110g/L, no. (%) of patients | 1423 (66.1) |
| S-phosphorus, mmol/L | |
| Range | 0.42–4.9 |
| Mean±SD | 1.58±0.56 |
| <1.1mmol/L, no. (%) of patients | 467 (21.7) |
| >1.8mmol/L, no. (%) of patients | 616 (28.6) |
| s-clacium, mmol/L | |
| Range | 0.90–3.58 |
| Mean±SD | 2.31±0.29 |
| <2.1mmol/L, no. (%) of patients | 252 (11.7) |
| >2.4mmol/L, no. (%) of patients | 545 (25.3) |
| s-calcium×phsophorus, mmol2/L2 | |
| Range | 0.91–13.9 |
| Mean±SD | 3.74±1.39 |
| >4.4mmol2/L2, no. (%) of patients | 626 (29.1) |
| s-iPTH, pg/mL | |
| Range | 1.2–4480.0 |
| Mean±SD | 407.8±512.4 |
| <150pg/mL, no. (%) of patients | 861 (40.0) |
| >300pg/mL, no. (%) of patients | 855 (39.7) |
During the three-year follow-up period, 577 (26.7%) patients died, 44 (2%) were transplanted, 69 (3.2%) were lost from the follow-up and 1463 remained on regular HD. When parameters listed in methods were analyzed by univariate Cox proportional hazard model, the following variables were selected as significant predictors of time to death: age, gender, duration of HD treatment, underlying kidney disease (diabetic nephropathy, Balkan nephropathy, polycystic kidney disease), hours of HD/week, Kt/V, hemoglobin, s-phosphorus, s-calcium, iPTH, use of oral iron and number of transfusions per year. Combining these variables in multivariate Cox proportional hazard model with adjustment for patient age, gender and duration of HD treatment, the significant independent predictors of time to death were selected (Table 4).
Relative risk of mortality: multivariate Cox proportional hazard model.
| Variable | B | RR (CI) | p |
|---|---|---|---|
| Male gender | −0.139 | 0.87 (0.66−1.15) | 0.326 |
| Age, years | 0.054 | 1.06 (1.04−1.07) | <0.0001 |
| Duration of HD treatment, years | −0.660 | 0.52 (0.47−0.57) | <0.0001 |
| Hours of HD/week | −0.100 | 0.91 (0.82−1.01) | 0.062 |
| Hemoglobin, g/L | −0.010 | 0.99 (0.98−1.00) | 0.019 |
| iPTH, pg/mL | 0.001 | 1.00 (1.00−1.01) | <0.0001 |
| Diabetic nephropathy, yes | 0.672 | 1.96 (1.39−2.76) | <0.0001 |
RR – relative risk, Exp(B), CI – 95% confidence interval of Exp(B), p – significance of coefficient.
We also used a Cox proportional hazards model to investigate the association between mortality and satisfying the guidelines targets. When targets of Kt/V, hemoglobin, serum phosphorus, calcium and iPTH were included in multivariate Cox model with adjustment for patient age, gender and duration of HD treatment (years), target values for Kt/V, hemoglobin and iPTH were found to be the significant independent predictors of time to death (Table 5). When Cox model was adjusted for patient age, gender, duration of HD treatment (years) and diabetic nephropathy the same targets values were selected as significant independent predictors of time to death as well as diabetic nephropathy. The values of regression coefficient (B), relative risk (RR) and confidence interval of relative risk (CI) as well as significance of coefficient (p) were as follows: Kt/V [B=−0.18, RR(CI)=0.83 (0.68–1.01), p=0.042], hemoglobin [B=−0.22, RR(CI)=0.80 (0.66–0.96), p=0.012], iPTH [B=−0.35, RR(CI)=0.71 (0.51–0.98), p=0.042] and diabetic nephropathy [B=0.68, RR(CI)=1.98 (1.52–2.55), p<0.0001].
Relative risk of mortality: multivariate Cox proportional hazard model included guidelines target values as independent variables.
| Variable | B | RR (CI) | p |
|---|---|---|---|
| Male gender | −0.25 | 0.78 (0.63–0.95) | 0.017 |
| Age, years | 0.04 | 1.04 (1.03–1.05) | <0.0001 |
| Duration of HD treatment, years | −0.59 | 0.55 (0.51–0.59) | <0.0001 |
| Hours of HD/week | −0.04 | 0.96 (0.91–1.02) | 0.216 |
| Kt/V >1.2 | −0.21 | 0.81 (0.66–0.98) | 0.037 |
| Hemoglobin >110g/L | −0.70 | 0.51 (0.36–0.73) | <0.0001 |
| s-phosphorus 1.1–1.8mmol/L | −0.07 | 0.93 (0.77–1.12) | 0.442 |
| s-calcium 2.1–2.4mmol/L | −0.06 | 0.94 (0.78–1.13) | 0.531 |
| iPTH 150–300, pg/ml | −0.35 | 0.71 (0.50–0.99) | 0.045 |
RR – relative risk, Exp(B), CI – 95% confidence interval of Exp(B), p – significance of coefficient.
The study involved 2153 patients on regular HD for averagely 5.3 years, dialyzed averagely 11.8h weekly on dialyzers with polysulfone membranes (15.7% on hemodiafiltration). The study was carried out in order to determine the percentage of patients not reaching the KDOQI guidelines targets in the five areas of HD practice and to find out whether the compliance with these targets was associated with patient outcome. Percentage of patients outside KDOQI guidelines targets was 42.4% for Kt/V, 66.1% for hemoglobin, 50.3% for serum phosphorus, 37% for serum calcium and 79.7%, for serum iPTH levels. Cox proportional hazard model with adjustment for patient age, gender and duration of HD treatment (years) found age, duration of HD treatment, hemoglobin, iPTH and diabetic nephropathy as significant independent predictors of time to death. When targets of Kt/V, hemoglobin, serum phosphorus, calcium and iPTH were included in multivariate Cox model, target values for Kt/V, hemoglobin and iPTH were found to be the significant predictors of time to death.
During the last few decades, several guidelines have been developed recommending standards for health care of HD patients.1–3 Soon thereafter, it was obvious that guideline adherence is a very difficult task to manage. Numerous national and international studies were undertaken to find out the proportion of patients failing to meet guidelines targets as well as the association of guidelines compliance and patients’ outcome.4,6,7,11 Most of these studies were carried out in developed countries. In recent years, the number of papers presenting epidemiological data on RRT in developing countries increased, but papers on the results of HD treatment and compliance with guidelines in developing countries are scarce.12–14 Recently, DOPPS 5 including several developing countries was initiated and their first results were reported at this years's ERA-EDTA Congress.15–17 Serbia is one of the developing countries that overpassed heavy nineties and that now has satisfactory conditions for HD treatment. In addition, at numerous scientific and educative meetings of our society recommendation of guidelines and their updating were discussed. This prompted us to check guidelines adherence and HD patient outcome in our country and compare it with those in other developing as well as developed countries. We selected KDOQI guidelines for comparative analysis since they were traditionally used by the most of the HD centers until 2012 when KDIGO guidelines started to be adopted as a daily practice.
In examined cohort of HD patients mean Kt/V was 1.24±0.31 and 42.4% of patients had Kt/V below 1.2, the minimum adequate dose proposed by KDOQI guidelines. However, 14.4% of patients had Kt/V below 1.0. Results of DOPPS I and II showed great variation in percentage of patients with spKt/V below 1.25. Nevertheless, in all countries that participated in the study percent of patients with spKt/V below 1.2 was lower in DOPPS II (ranging between 10% and 31%) than in DOPPS I (14–42%). In our country percent of patients failing to meet Kt/V target decreased significantly during the last decade,9 but it is still higher than those reported in DOPPS II, although DOPPS II was finished six years before our study. Mean Kt/V for HD population presented here was comparable to those reported in several observation national studies from developed countries,6,18 but higher than in some developing countries.13,14 However, mean Kt/V reported recently for HD patients from Russia and Turkey, two developing countries included in DOPPS 5, was 1.49±0.33 and 1.60±0.31, respectively.15,16
Our study showed that Kt/V was a significant predictor of mortality that was reported previously and was the impetus for improvement of HD adequacy. Numerous studies indicated beneficial effect of increasing dialysis dose on patient survival,19–21 although it is still not proven that increasing the Kt/V above the guidelines target would reduce patient mortality.22,23 DOPPS study showed that not only dialysis dose but blood flow rate, duration of HD and type of dialysis had significant influence on patient survival.24,25 Nevertheless, for nephrologists in our country increasing of the HD adequacy and decreasing the percentage of patients failing to meet Kt/V target remains and important task. To achieve this it will be necessary to first carefully analyze the factors responsible for such high percentage of patients with Kt/V below recommended minimum of Kt/V. However, these factors were not objective of the present study. From the definition of Kt/V it is clear that it depends on dialyzer characteristics and dialysis time but increasing Kt/V depends primarily on the rate of blood flow through the dialyzer and a good vascular access is a key factor for achieving good blood flow and Kt/V. The vast majority of our patients had AV fistula but the data on blood flow as well as on many other factors influencing blood flow and Kt/V (comorbidities, hemodynamic stability during RRT, serum albumin, hematocrit, patient adherence to the prescribed regimen) were not available in the present study. The analysis of the factors influencing low Kt/V in 42.4% of our patients requires additional detailed study. Using available data from this study, we found significant correlation (p<0.0001) between Kt/V and age, body weight, hours of dialysis weekly, type of dialysis (low and high-flux dialyzers, hemodialfiltration).
After 2004, ESA has become more accessible in our HD units and hemoglobin levels increased significantly.9 However, at the onset of the present study 66.1% of patients had hemoglobin level below KDOQI guideline target of 110g/L and this percentage is lower than in most of developed countries26–28 but similar or even higher than in developing countries.29–31 Mean hemoglobin level was lower in HD patients examined here than in those treated in all countries participating in DOPPS I–III except in Japan.32 In Japan maximal ESA dose was limited by public reimbursement, but mean ESA dose in this country was about 50% higher than the mean dose used in our HD patients. Our Health Insurance Fund determined hemoglobin between 100 and 110g/L as target hemoglobin. However, 41.4% of patients had hemoglobin below this target that is much more than the percentage shown in our previous cross sectional study.9 That could be explained not only by the limitation of our Health Insurance Fund but also by occasional ESA shortages caused by irregular supply due to prolonged tender procedures. It shows that compliance with guidelines depends not only on their knowledge but also of local circumstances. The importance of achieving target hemoglobin levels derived from its significant association with mortality showed in the present study as well as in many others.5,33–35 Therefore, the continuous effort to increase the percentage of patients achieving target hemoglobin value remains an important task.
Percentage of patients who fell within K/DOQI recommended range for serum phosphorus (49.7%) and iPTH (20.3%) was comparable with those in the DOPPS studies.5,36 It is obvious that in our HD population like in many others7,30,36 patients with low iPTH level represent twice the bigger problem than those with severe hyperparathyroidism while the opposite is found in some other countries.31,37 Percentage of patients who achieved targets for serum calcium was higher (63%) than in DOPPS studies and similar to results presented in some recent studies.7,38
Numerous studies found a significant relationship between serum levels of phosphorus, calcium, PTH and mortality.39–41 However, several meta-analyses reported conflicting data: some found significant association between increased values of all three parameters and mortality,42 others found association only between high phosphorus serum level and mortality,43 while some found different relationship between mortality and these three parameters depending on whether their values were above or below recommended targets.44,45 Using univariate Cox proportional hazard model we found higher mortality risk in patients with higher phosphorus and iPTH and lower calcium serum levels. However, only iPTH appeared as a significant independent predictor of time to death in multivariate Cox proportional hazard model. Although majority of our patients had lower iPTH than that proposed by guideline, those with higher iPTH value are at higher risk of mortality. In addition, when targets of all five examined HD practice parameters were involved in Cox proportional hazard model, being outside target range for iPTH was also found to be associated with significantly higher risk for death.
This study has several limitations. Clinical and laboratory parameters measured only in the onset of the study were included in the analysis, although multiple measurements of these parameters would be more conclusive since interventions by nephrologist were guided by initial results.
The limitation of this study is that the data on comorbid conditions were not available and adjusting for these conditions in the Cox models was not possible. Comorbidity was found as a strong predictor of mortality in incident HD patients.46,47 However, the study performed in incident patients registered in European Renal Association–European Dialysis and Transplant Association Registry showed that after adjustment for age, gender, primary renal disease and treatment modality the influence of comorbidity was less important than expected.48 Analysis of results obtained in DOPPS study also showed that adjustment for patient demographics and comorbidities only partially reduced survival differences by location and other factors that might contribute to differing outcomes were described.49 Although these data suggest that our results would insignificantly change if comorbidity was accounted for, the impact of comorbidity required to be examined. The present study was aimed to find out compliance with KDOQI guidelines targets and it has been shown that substantial proportion of patients examined failed to meet these targets. Moreover, the noncompliance with guidelines targets was associated with an increased risk of death. This study as a starting point would be significant only if the research continues to find out all potential factors associated with the failure to achieve guidelines targets which is beyond the scope of this paper.
ConclusionAccording to the present analysis critical points of HD practice in Serbia included low dialysis dose (in 42.4% of patients), low hemoglobin level (in 66.1%), hyperphosphatemia (in 28.6%) and low (in 40%) and high (in 21.5%) iPTH levels. Age, duration of HD treatment, hemoglobin, iPTH and diabetic nephropathy were selected as significant independent predictors of time to death. The relative risk of time to death was associated with being outside the guidelines targets for Kt/V, hemoglobin and iPTH. The study suggests vast opportunities for the improvement of HD patient care and possibly patient outcome.
Conflict of interestThe authors declare no conflicts of interest.



