





Continuous ambulatory peritoneal dialysis (CAPD) is used as an alternative to hemodialysis and has very few complications which include abdominal hernia, peritonitis, processus vaginalis, pleural leakage, and those related to the catheter exit site.1 It may occasionally be complicated by leakage of dialysate fluid into the abnormal sites.2,3 We report a case of a woman who experienced vaginal leakage during CAPD and after peritonitis.
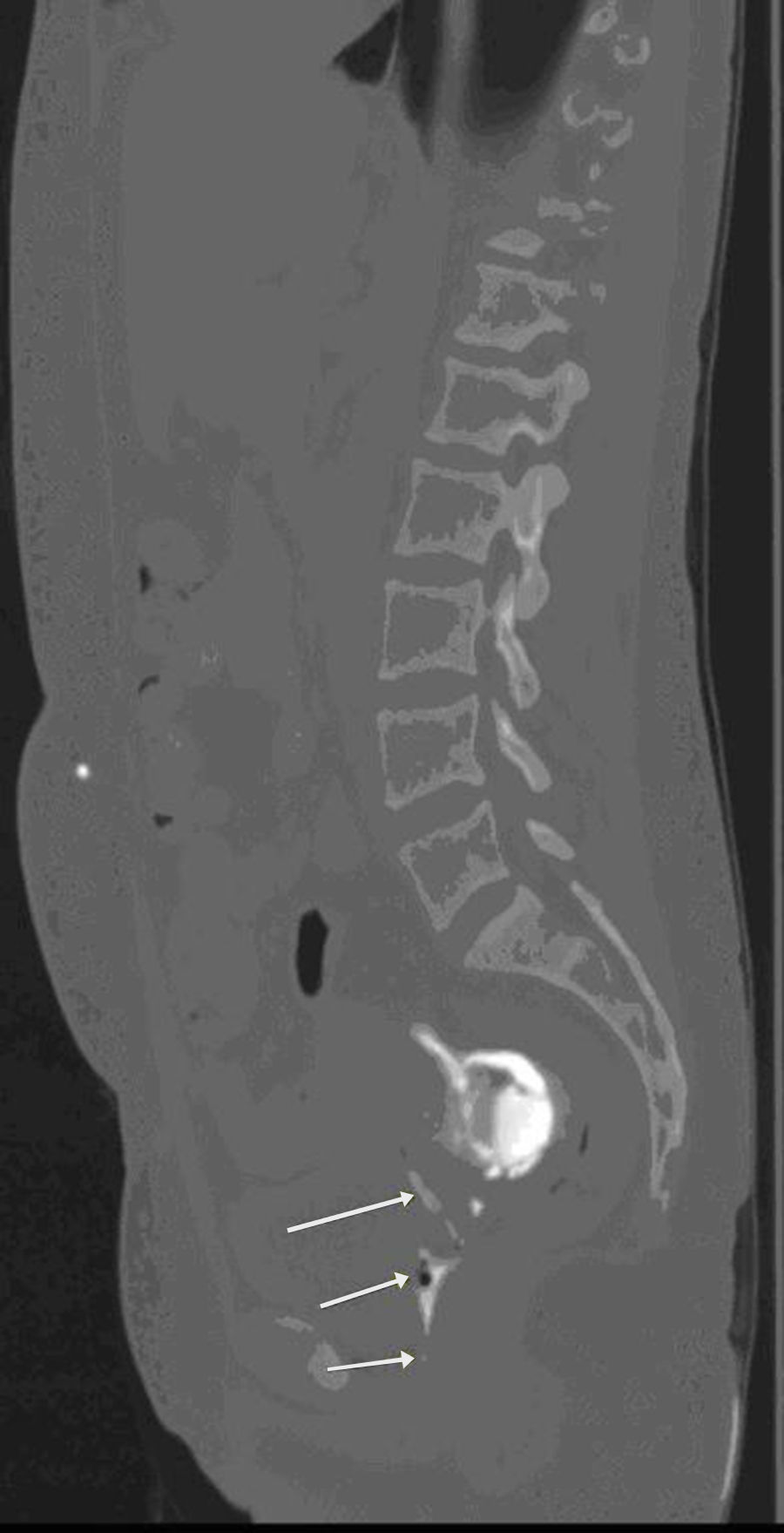
A 24 year old female patient was diagnosed with end stage renal disease during pregnancy. There was no other etiological factor, but hypertension. Patient was recommended 20hours of hemodialysis, but she refused and gave birth to a living child on the 38th gestational week. She has been on CAPD for the last 3 months. Since last week she has started to have abdominal pain accompanied with nausea and fever (>38°C). With these complaints she was referred to our policlinic and her peritoneal fluid cell count was found 4860/mm3 (95% polymorphonuclear leukocytes). Cultures were obtained and she was admitted to our hospital with the diagnosis of peritonitis. Blood analysis showed leucocytes 9000/mm3, hemoglobin: 8.8g/dl (11.5–16), C-reactive protein: 14.2mg/dl (0–0.5), sedimentation: 135mm/hour. Pseudomonas aeruginosa was detected in blood cultures. She was on empiric ceftazidime and cefazolin treatment and treatment was continued because P. aeruginosa was found sensitive to this treatment. Urine culture remained sterile. Patient stated that there is dialysate in her vagina. She was consulted with obstetrics and gynecology regarding any fistulas. A urine catheter was placed and it is understood that origin of dialysate was vagina. Contrast enhanced computerized tomography was done showing a vaginal fistula (Figs. 1 and 2). CAPD catheter was removed. Surgical operation was found unnecessary and hemodialysis was started. Patient was discharged after 3 weeks of ant biotherapy.

Patients on CAPD have an increased risk of both hernia formation and dialysate leakage as an intraperitoneal pressure related complications. One of the rare peritoneal fluid leakage is through processus vaginalis3 and main mechanisms include leakage through the fallopian tube and then the uterus and vagina, or leakage through a fistula between the uterus and the peritoneal cavity formed after surgery.3 One of the reason for fistula formation is peritonitis which is often caused by skin bacteria penetration via transvisceral, transvaginal or hematogenous spread of organisms, and the CAPD catheter can become colonized by bacteria creating a biofilm that repeatedly seeds the peritoneum.4
In our case, a rare entity; vaginal fistula and also another rarely seen clinic; peritonitis secondary to vaginal fluid were present. Probably secondary to the fistula, peritonitis developed and after peritonitis, fluid from fistula tract has increased and caused vaginal leakage.



