

Peritoneal catheter displacement is one of the most common complications of peritoneal dialysis. The alpha manoeuvre has been proposed as a repositioning technique, which involves returning the catheter to its correct position using rigid guidewires under fluoroscopic guidance. The aim of this study is to analyse the 107 procedures performed at our Centre to identify factors that may predict the success of the technique.
Material and methodsThe alpha manoeuvre method was used in 86 patients, with a total of 107 procedures (70 patients underwent one manoeuvre only, 16 patients underwent two or more manoeuvres).
ResultsThe overall success rate of the technique was 60%. There were no differences in success rate in terms of gender (60% male vs 40% female, p = 0.104), time of catheter failure (early 60% vs late 62%, p = 0.849), type of catheter (75% self-locating vs 58% spiral, p = 0.633) or the initial position of the catheter. There was only one case of peritonitis related to the procedure.
ConclusionsThe alpha manoeuvre is an effective and safe method for correcting peritoneal catheter displacement.
La malposición del catéter peritoneal es una de las complicaciones más frecuentes de la diálisis peritoneal. Para recolocarlo se ha propuesto realizar la maniobra alfa que consiste en devolver al catéter a su correcta posición a través de unas guías rígidas bajo control fuoroscópico. El objetivo del presente estudio es analizar los 107 procedimientos realizados en nuestro Centro tratando de determinar factores que puedan predecir el éxito de la técnica.
Material y métodosEl método de la maniobra alfa fue utilizado en 86 pacientes con un total de 107 procedimientos (70 pacientes solo una maniobra, 16 pacientes 2 maniobras o más).
ResultadosEl éxito global de la técnica fue de un 60%. La tasa de éxito no mostró diferencias en cuanto al sexo (60% en varones frente a 40% mujeres, p = 0,104), tiempo de fallo del catéter (fallos precoces 60% frente a fallos tardíos 62%, p = 0,849), tipo de catéter (75% en autoposicionantes frente a 58% en espirales, p = 0,633), ni en cuanto a la posición inicial del catéter. Sólo hubo un caso de peritonitis secundaria al procedimiento.
ConclusionesLa maniobra alfa es un método eficaz y seguro en la corrección de la malposición del catéter peritoneal.
The term peritoneal dialysis encompasses all those replacement treatment techniques that use the peritoneal membrane as a dialysis membrane. The peritoneal membrane itself, the dialysis fluid and the catheter constitute the three basic elements of this technique.1,2 The catheter is the element that allows communication between the peritoneal cavity and the exterior. It is made of silicone or polyurethane, and the most distal part is housed in the peritoneal cavity. Some models include a tungsten end weight (self-positioning) which has the advantage of less displacement and poor function compared to other types of catheters.3,4
One of the most common complications in peritoneal dialysis is the malfunction of the catheter, due to mispositioning or blockage of the distal end. The ideal position of the peritoneal catheter is one in which the distal end is located in the cul-de-sac of Douglas. After taking an X-ray to see the location of the catheter, measures are prescribed to stimulate intestinal peristalsis (enemas). If it is not effective, the alpha maneuver is performed, consisting of repositioning the catheter through rigid guides using fluoroscopic control. Ultimately, if the catheter still doesn't work, a replacement is done. The objective is to review the 107 cases of the last 10 years trying to find factors that can predict the success of the technique.
Material and methodsRetrospective longitudinal observational study in which all alpha maneuvers performed at the Hospital Universitario Central de Asturias between 2008 and 2018 were analyzed. Clinical data of the patients (age, sex, etiology of kidney disease), related to the technique (start of the technique, time with the catheter, initial location of the catheter), date of performance of the maneuver, and if there were complications. The total number of procedures required by a patient was also taken into account, and in cases where more than one maneuver was performed, if there were re-maneuvers, that is, if a second maneuver was performed within a month after the first maneuver.
Early failure was considered when the malfunction occurred within a month or less from the placement of the catheter, and late failure when it occurred more than a month after placement.
The maneuver was performed in patients with decreased peritoneal effluent, once the malposition was verified on the plain abdominal X-ray, and the improvement with enemas was not observed.
Procedure: The alpha maneuver is a procedure that aims to reposition the peritoneal catheter through fluoroscopic control, in those that are mispositioned, in order to make them function again, without having to resort to a more invasive technique (such as the laparoscopic repositioning or surgical exchange). The procedure is performed in a Vascular Radiology room, covering the patient with sterile cloths, leaving a hole for the catheter that is cleaned with an antiseptic solution (in our case, povidone iodine if the patient is not allergic). Two 0.35 mm rigid hydrophilic guides with an angled end at 35 ° are inserted through the catheter that must protrude through the distal end until a resistance is found to serve as support so that, when exerting advance pressure, a loop is formed in the free peritoneal cavity to push back the catheter tip. The objective is that when the guides are withdrawn, the distal end of the catheter is housed in the lower pelvis or at least has a different position than the initial one (Fig. 1). After the procedure, 1 g of vancomycin is applied as antibiotic prophylaxis to all patients.5

The success of the technique has been defined as the good functioning of the catheter without the need for a new maneuver, replacement or removal of the same in the following 30 days. Therefore, a clinical criterion has been followed. The technical success or the final situation in the imaging test after the procedure has not been taken into account.
The database obtained from the patients' medical records was collected in a Microsoft Excel sheet and the data were analyzed using the SPSS 20.0 program (Chicago, IL). Values are expressed as mean ± standard deviation if the variables did not follow a normal distribution. To analyze the differences between successful and unsuccessful test maneuvers used X 2 for qualitative variables and t of Student or the Mann-Whitney test for quantitative variables with normal distribution or not Gaussian distribution respectively. We assume a statistically significant difference when p < 0.05.
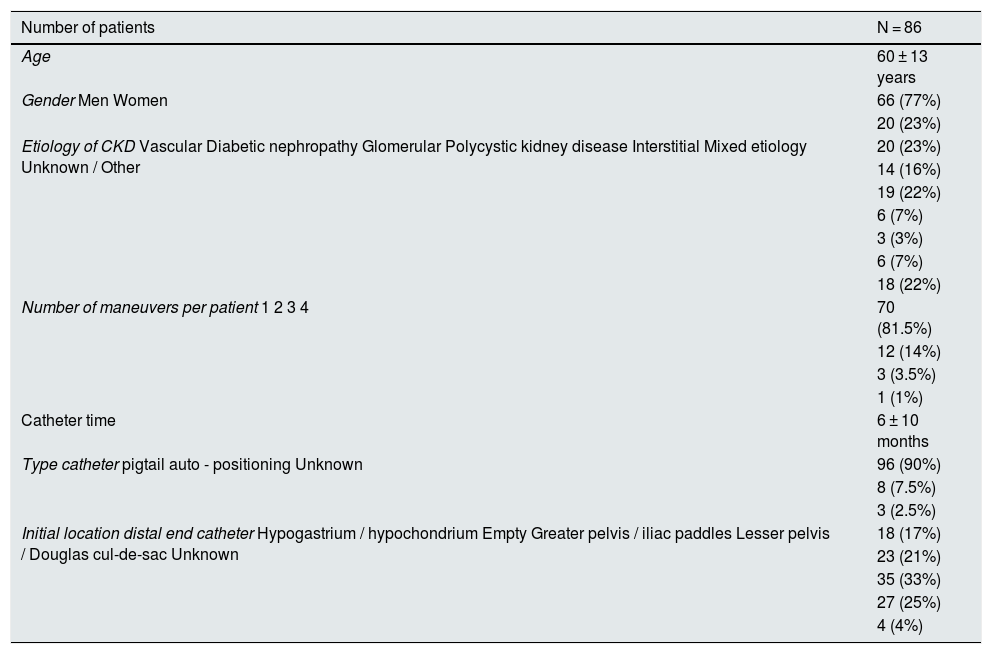
ResultsDuring the study period, 107 procedures were performed in 86 patients, of which 77% were men, with a mean age of 60 ± 13 years. Other clinical data of the patients can be seen in the Table 1. Of the 107 alpha maneuvers performed, 48% were early failures and 52% late, with a mean of 6 ± 10 months.
Patient characteristics and maneuvers.
| Number of patients | N = 86 |
|---|---|
| Age | 60 ± 13 years |
| Gender Men Women | 66 (77%) |
| 20 (23%) | |
| Etiology of CKD Vascular Diabetic nephropathy Glomerular Polycystic kidney disease Interstitial Mixed etiology Unknown / Other | 20 (23%) |
| 14 (16%) | |
| 19 (22%) | |
| 6 (7%) | |
| 3 (3%) | |
| 6 (7%) | |
| 18 (22%) | |
| Number of maneuvers per patient 1 2 3 4 | 70 (81.5%) |
| 12 (14%) | |
| 3 (3.5%) | |
| 1 (1%) | |
| Catheter time | 6 ± 10 months |
| Type catheter pigtail auto - positioning Unknown | 96 (90%) |
| 8 (7.5%) | |
| 3 (2.5%) | |
| Initial location distal end catheter Hypogastrium / hypochondrium Empty Greater pelvis / iliac paddles Lesser pelvis / Douglas cul-de-sac Unknown | 18 (17%) |
| 23 (21%) | |
| 35 (33%) | |
| 27 (25%) | |
| 4 (4%) |
CKD: Chronic kidney disease.
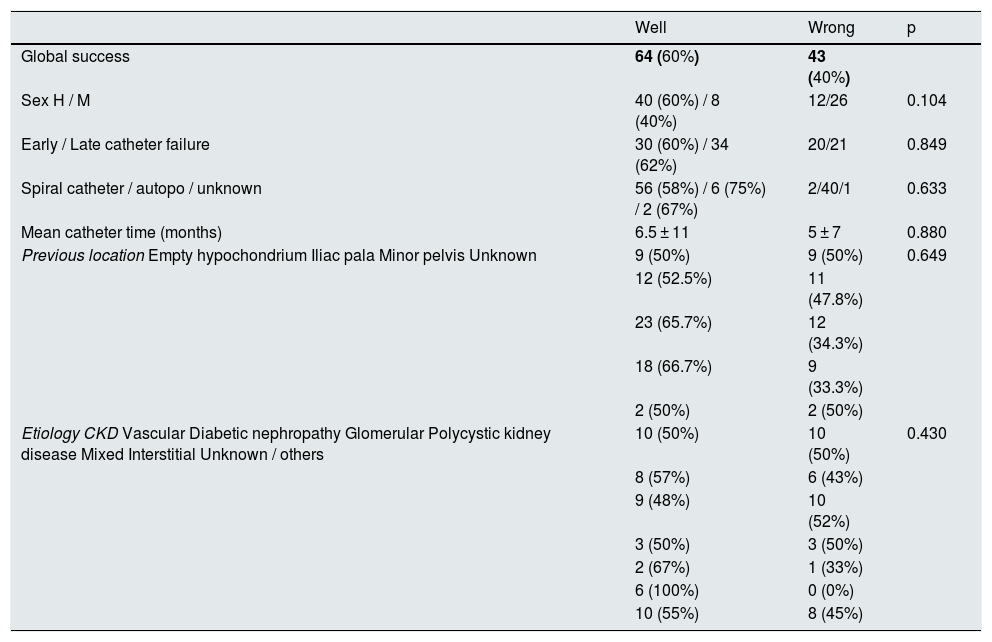
The overall success of the technique was 60%, as can be seen in the Table 2, as well as the rest of the results. There were no major differences between the time of evolution from the placement of the catheter to the maneuver (6.5 ± 11 months in which it was successful versus 5 ± 7 months in which it was not). Regarding the previous location of the catheter, the best results were found in cases in which the initial location was the lower pelvis/Douglas cul-de-sac with 66.7% success, followed by the greater pelvis/iliac paddles with 65, 7%, void zone with 52.5% and finally, hypochondrium/hypogastrium with 50% (p = 0.649).
Success of the alpha maneuver.
| Well | Wrong | p | |
|---|---|---|---|
| Global success | 64 (60%) | 43 (40%) | |
| Sex H / M | 40 (60%) / 8 (40%) | 12/26 | 0.104 |
| Early / Late catheter failure | 30 (60%) / 34 (62%) | 20/21 | 0.849 |
| Spiral catheter / autopo / unknown | 56 (58%) / 6 (75%) / 2 (67%) | 2/40/1 | 0.633 |
| Mean catheter time (months) | 6.5 ± 11 | 5 ± 7 | 0.880 |
| Previous location Empty hypochondrium Iliac pala Minor pelvis Unknown | 9 (50%) | 9 (50%) | 0.649 |
| 12 (52.5%) | 11 (47.8%) | ||
| 23 (65.7%) | 12 (34.3%) | ||
| 18 (66.7%) | 9 (33.3%) | ||
| 2 (50%) | 2 (50%) | ||
| Etiology CKD Vascular Diabetic nephropathy Glomerular Polycystic kidney disease Mixed Interstitial Unknown / others | 10 (50%) | 10 (50%) | 0.430 |
| 8 (57%) | 6 (43%) | ||
| 9 (48%) | 10 (52%) | ||
| 3 (50%) | 3 (50%) | ||
| 2 (67%) | 1 (33%) | ||
| 6 (100%) | 0 (0%) | ||
| 10 (55%) | 8 (45%) |
We only found two complications after the procedure, one consisting of peritonitis and the other that resulted in an episode of mild hemoperitoneum.
Of the 43 procedures that presented adverse results, in four cases the maneuver was repeated (new procedure within the following 30 days), in four it was repositioned laparoscopically, in 26 a replacement was performed, and in eight the catheter was removed to go to hemodialysis for other added reasons.
DiscussionWe present data on 107 procedures performed on 86 patients over 10 years, one of the longest series to date; This is due to the fact that we have a large population on dialysis in our center, some 603 patients during the decade of study.
We have found an overall success rate of the maneuver of 60%. Reviewing the bibliography we find that the success rate described by different authors ranges from 46 to 80%.6,7
The success rate based on sex has been higher in men (60%) than in women (40%), without having been able to find an explanation for this finding, although the results did not reach statistical significance.
Depending on the type of catheter, we have been able to observe that better results were obtained in self-positioning (75%) compared to spiral catheters in pig's tail (58%), however, we only had eight catheters of this type in the sample (7.5% of the sample). This is due to the fact that in our center of choice a gooseneck catheter with a spiral end or pig tail is placed, and only in selected cases a catheter with a tungsten end or self-positioning (in cases of patients with a history of abdominal surgeries or previous peritoneal catheter failure), accounting for approximately 10% of implanted catheters. All the catheters are placed by General Surgeons by performing a minilaparotomy, in the right paramedial line (except in cases in which a previous catheter had been implanted, which is placed on the left side) and under local anesthesia.
Regarding catheter failure, the best results have been obtained in the cases of late versus early failures, but without major differences (62% vs. 60%). In other works such as Moss et al.8 also found no correlation between the duration of catheter function before manipulation and subsequent patency. Other authors have found better results in those in which they were early failures compared to late failures of the catheter such as Siegel (75% vs 44%).9 Others have found an opposite trend, in which late failure catheters achieved higher success rates like the Degesys group's work (30% vs. 60%).10 Savader (25% vs 65%)11 or the Kwon group 31% vs 61.1%.12
The initial location of the catheter could be decisive when it comes to predicting success, we have found that the lower the initial position of the catheter, the greater the probability of success (66.7% when they were located in the smaller pelvis, 65, 7% in iliac paddles, and 52.5% empty, 50% hypochondria) although these results were not statistically significant. This hypothesis has been demonstrated in other studies, in which a higher percentage of success has been described in catheters located in the pelvis compared to those in the upper abdomen (73.5% vs. 42.9%, p = 0.01).13
Regarding complications, the rate of peritonitis associated with the procedure has been established between 0% 1, 2–2.9%.13 In our study we have only detected one case of peritonitis in the 107 procedures, which represents a rate of 0.93%.
ConclusionThe alpha maneuver is a simple, effective technique with few complications, which avoids the use of other more aggressive techniques in cases of mispositioning of the peritoneal catheter.
The best results were seen when lower is initially located the distal end of the catheter, in men, failure late catheter and catheter use auto - positioning, although unable to reach statistical significance, requiring studies with a sample size higher to confirm these findings. However, the technique is successful in 60% of cases, so we consider that it should be part of the usual management of the catheter in cases of malposition.
Please cite this article as: del Río García L, Bueno CM, Ledo LA, Santamarta LÁ, Suárez CR, Álvarez ES. Utilidad de la maniobra alfa en la malposición del catéter peritoneal: revisión y experiencia. Nefrologia. 2020;40:531–535.



