



















Introducción y objetivos: Actualmente no existe un registro que muestre en su conjunto y globalidad la realidad de la diálisis peritoneal (DP) en España. Sin embargo, para distintos congresos y reuniones se ha elaborado durante varios años un informe sobre la DP en España a partir de datos comunicados por cada uno de los registros de las comunidades autónomas y regiones. El objetivo fundamental del presente trabajo es analizar todos estos datos en forma agrupada y comparativa, con objeto de conseguir una muestra representativa de la población española en DP en los últimos años, para su análisis y resultados en cuanto a datos demográficos, penetración de la técnica, diferencias geográficas, incidencia y prevalencia, aspectos técnicos, indicadores intermedios, comorbilidad y resultados finales como supervivencia del paciente y de la técnica puedan ser extrapolables a todo el territorio nacional. Diseño, material y métodos: Estudio observacional de cohortes de registros autonómicos de DP, abarcando el mayor porcentaje posible de la población española adulta (mayores de 14 años) en DP, al menos en la última década (1999-2010), y en la mayor área geográfica que nos ha sido posible reclutar. Se ha seguido una estrategia precisa de recogida de información de cada registro autonómico. Una vez recibida la información y depurada, se integran como datos agregados, para su estudio estadístico. Resultados: Los registros autonómicos que han participado representan un área geográfica total que engloba a 32 853 251 habitantes mayores de 14 años, el 84 % de la población española total a partir de esa edad. La tasa anual media de incidentes por millón de habitantes (ppm) es variable (entre los 17,81 ppm de Andalucía y los 29,90 ppm del País Vasco), observándose en los últimos años un discreto y permanente aumento de la incidencia global en la DP en España. La prevalencia media anual por millón de población (ppm) es muy heterogénea (desde 42 a 99 ppm). Se observa un aumento progresivo medio en el uso de la diálisis peritoneal automática (DPA). La tasa de peritonitis es de aproximadamente un episodio cada 25-30 meses/paciente, observándose una ligera disminución en los años más recientes. Las causas de salida del programa de DP se distribuyen, de forma bastante homogénea entre las distintas comunidades, prácticamente en un tercio por muerte del paciente (media 28 %), un tercio por trasplante renal (media 39 %) y un tercio pasan a hemodiálisis (fracaso de la técnica: media 32 %). Las principales comorbilidades fueron la enfermedad cardiovascular (30,2 %) y la diabetes mellitus (24,2 %). La supervivencia global media acumulada ha sido del 92,2 %, 82,8 %, 74,2 %, 64,8 % y 57 %, al año, dos, tres, cuatro y cinco años, respectivamente. Proporcionaron de forma significativa e independiente una peor supervivencia para el paciente una mayor edad, la enfermedad cardiovascular, la diabetes mellitus, la técnica de diálisis peritoneal continua ambulatoria (frente a DPA), el inicio de la DP antes de 2004 (analizado en Andalucía y Cataluña) y la menor función renal residual al inicio de la DP (analizado en el registro de Levante). De igual forma, actualmente ha mejorado la supervivencia de la técnica, presentando unas cifras promedio superiores al 50 % a los 5 años. Conclusiones: La incidencia y la prevalencia de la DP en España están creciendo moderadamente de forma generalizada, si bien siguen manteniendo una distribución por comunidades autónomas irregular. Tanto la supervivencia del paciente como de la técnica es superior al 50 % a los 5 años, habiendo mejorado en los últimos años, y siendo comparable a los países de mejores resultados en este tratamiento.
Introduction and objectives: There is currently no registry that gives a complete and overall view of the peritoneal dialysis (PD) situation in Spain. However, a report on PD in Spain was developed for various conferences and meetings over several years from data provided by each registry in the autonomous communities and regions. The main objective of this study is to analyse this data in aggregate and comparatively to obtain a representative sample of the Spanish population on PD in recent years, in order that analysis and results in terms of demographic data, penetration of the technique, geographical differences, incidence and prevalence, technical aspects, intermediate indicators, comorbidity, and outcomes such as patient and technique survival may be extrapolated to the whole country. Design, material and method: Observational cohort study of autonomous PD registries, covering the largest possible percentage of the adult Spanish population (over 14 years of age) on PD, at least in the last decade (1999-2010), and in the largest possible geographical area in which we were able to recruit. A precise data collection strategy was followed for each regional registry. Once the information was received and clarified, they were added as aggregate data for statistical study. Results: The regional registries that participated represent a total geographical area that encompasses 32,853,251 inhabitants over 14 years of age, 84% of the total Spanish population older than that age. The mean annual rate of incidents per million inhabitants (ppm) was variable (between 17.81ppm in Andalusia and 29.90ppm in the Basque Country), with a discrete and permanent increase in the overall PD incidence in Spain being observed in recent years. The mean annual prevalence per million population (ppm) was very heterogeneous (from 42 to 99ppm). A mean progressive increase in the use of automated peritoneal dialysis (APD) was observed. The peritonitis rate was approximately one episode every 25-30 months/patient, with a slight decrease being observed in recent years. The causes of discontinuing PD were distributed fairly evenly between communities; almost a third was due to patient death (mean 28%), a third was due to renal transplantation (mean 39%) and a third was due to transfer to haemodialysis (technique failure: mean 32%). The main comorbidities were cardiovascular disease (30.2%) and diabetes mellitus (24.2%). The overall accumulated mean survival was 92.2%, 82.8%, 74.2%, 64.8% and 57% after one, two, three, four and five years respectively. There was significantly and independently worse survival for older patients and those with cardiovascular disease, patients with diabetes mellitus, those on continuous ambulatory peritoneal dialysis (vs. APD), those who started PD before 2004 (analysed in Andalusia and Catalonia), and patients with lower residual renal function at the start of PD (analysed in the Levante registry). Similarly, the technique survival has improved, showing a mean figure above 50% after 5 years. Conclusions: The incidence and prevalence of PD in Spain are growing moderately and in a generalised manner and continue to maintain an irregular distribution by autonomous community. Both patient and technique survival were greater than 50% after 5 years, with an improvement being observed in recent years, and are comparable to countries with better results in this treatment.
INTRODUCTION
Currently, the use of home peritoneal dialysis (PD) as a dialysis technique in Spain is clearly disproportionate with respect to haemodialysis (HD). PD, despite being a technique performed by the patient in their own home and requiring fewer resources, is poorly developed in our country, although there are very significant differences among autonomous communities.
Some of these communities have separately reported the results of their PD registries, such as the Eastern region, Madrid and Centre and Andalusia,1 but there is currently, unlike the case for kidney patients as a whole,2 no registry that gives a complete and overall view of the PD situation in Spain.
After some years spent developing a report on PD in Spain from separate data from each regional registry and society, which were presented at different Spanish PD meetings, we made an effort to compile and analyse all these data in aggregate and comparatively, in order to better understand the situation of this renal replacement therapy (RRT) technique in Spain, and we achieved a sample which may be considered representative and which may be extrapolated to the whole of Spain. This was the main objective of this study, which may be broken down into three parts as follows:
As we will discuss in the corresponding section, we encountered significant methodological difficulties in this report, mainly due to the different developmental processes of the autonomous community registries that contributed data.
PATIENTS AND METHOD
Study design and population
This was a descriptive, observational cohort study whose aim was to understand the PD situation in Spain, covering the largest possible percentage of the Spanish adult population (over 14 years of age) that we could recruit, at least over the last decade (1999-2010), and over the largest possible geographic area, in terms of demographic data, technique penetration, geographic differences, incidence and prevalence, technical aspects, intermediate indicators, comorbidity and final outcomes, such as patient and technique survival.
Information collection strategies
A. Identification of the main autonomous and/or local/regional PD registries in Spain:
Not all autonomous communities have these registries. From previous publications and reports at conferences, we identified the following communities and/or areas that could participate in the study:
- Autonomous Community of Andalusia: through the Autonomous Transplant Coordination Information System.
- Autonomous Communities of Galicia and Asturias.
- Autonomous Community of the Basque Country.
- Eastern registry: Valencian Community, Community of Murcia and Cuenca and Albacete provinces.
- Central registry: Autonomous Community of Madrid and Cáceres, Ciudad Real, Guadalajara, Ávila, Valladolid, Segovia, Burgos, Soria, Palencia and Zaragoza provinces.
- Autonomous Community of Catalonia: through the Registre de Malalts Renals de Catalunya, Organització Catalana de Trasplantaments.
B. Communication with heads of the different autonomous PD registries and requests to share their data in the single registry that is the subject of this project-report.
To guarantee the maximum number of positive responses and minimise losses, we developed an information strategy for the registry heads via electronic and telephone communication and at meetings before we sent and they completed the questionnaires in the different PD forums already existing in Spain (the National Peritoneal Dialysis Conference, the National Conference of the Spanish Society of Nephrology and the Support Group for Peritoneal Dialysis Development in Spain, etc.).
C. Authorisation for data transfer by the competent registry heads.
D. The sending, completion and return of the questionnaire for data collection.
Data processing strategies
Once the information had been received and processed, it was included as aggregate data, to be studied and compared as described in the following analysis section, which could also be used for future needs (various future projects).
Data analysis
In this section, we include all PD data from the last decade in Spain (1999 to 2010). Some registries may not have provided data for the whole period, in which case, data corresponding to the years they provided were included in the analysis.
- The start of follow-up for each patient was defined as the date in which they were included in the PD programme. Patients diagnosed with acute renal failure were excluded.
- The end of follow-up for each patient was defined as the time when they discontinued the PD technique, either due to transplantation, death or transfer to HD. Those who were still on the technique at the end of the study period (31 December 2010), were described as “living and on PD”.
- INCIDENCE was defined as the number of new PD patients per year.
- PREVALENCE was defined as the number of patients on PD on 31 December of each year.
- Causes of chronic kidney disease and death were defined in accordance with the European Dialysis and Transplant Association codification system.
- In the survival analysis, the starting point was defined as the first day of PD.
- The final events for survival analysis were:
- Patient death (patient survival studies): patients who were withdrawn due to transplantation, transfer to HD or loss to follow-up were excluded from this analysis.
- Transfer to HD (technique survival studies): patients who were withdrawn due to transplantation, death or loss to follow-up were excluded from this analysis.
Variables
The variables analysed were demographic variables, such as sex, age at the start of the technique, kidney disease aetiology, technique aspects, such as whether the patient was on automatic PD (APD) or continuous ambulatory PD (CAPD), type of solutions (lactate or bicarbonate with low glucose degradation products, icodextrin), implantation technique and type of catheter, initial comorbidity (diabetes, high blood pressure, cardiovascular disease, old age, etc.), Charlson index, mean technique duration time, condition at the end of follow-up (deceased, received a transplant, transferred to HD, or living and on PD) and cause of death, if applicable.
Statistical methodology
The data were analysed using the SPSS statistical software. We used central tendency and dispersion measurements (means, standard deviation) for quantitative variables and frequencies for qualitative variables; for inferential statistics, data comparison using the χ2 test and the Student’s t-test according to the types of variables, risk identification and 95% confidence intervals, Kaplan-Meier survival curves and the log-rank test for curve comparison. For multivariate analysis, we used the Cox proportional hazards model.
RESULTS
Descriptive and population characteristics
The data collected by the different autonomous registries, over a maximum period from 1 January 1999 to 31 December 2010, were taken from 6445 patients.
Table 1 lists the incident patients in each registry in the period studied, the mean annual incidence per million inhabitants, prevalent patients at 31 December 2010 (2095 patients in total), as well as the rate of prevalent patients per million inhabitants and by geographical area on this date.
It should be noted that not all communities provided patient data for the whole period, which was due to the difficulties involved in homogenising the databases, as well as the registry structure of each community, the time at which they started collecting data and their degree of availability.
However, we were able to collect data from a total geographic area covering32,853,251 inhabitants older than 14 years of age, that is, 84% of the total Spanish population of this age, which provided us with results that are highly representative of the situation in our country with regard to PD technique, and these results can be extrapolated to the whole of Spain (Figure 1).
Incidence: Figure 2 displays a slight increase in overall incidence in PD in Spain (broken red arrow), particularly in recent years, and in almost all autonomous communities, with Madrid-Centre, Catalonia and Andalusia showing a moderate and continuous increase from the start of the period studied.
As we can see in Table 1, the mean annual rate of incident patients per million inhabitants (ppm) varied between the different communities, with values between 17.81ppm in Andalusia and 29.90ppm in the Basque Country being observed.
In a mean 78.5% of these incident patients, PD was the first RRT, with the mean treatment background percentages for HD and transplantation being 16.4% and 5.1%, respectively. These frequencies were fairly homogeneous for all communities (Figure 3).
On average, in 80% of cases, PD was freely chosen by patients (range between values of 83% in Andalusia and 92% in Madrid-Centre and values of around 70%-73% in the Eastern region and the Basque Country); in the remaining 20%, there was a medical cause, mainly vascular access problems (impossibility or exhaustion) and heart diseases, that prevented PD from being selected
Prevalence (Table 1 and Figure 4): the mean annual prevalence per million inhabitants was very heterogeneous and varied between different geographic regions. PD had a higher penetration in communities such as Galicia-Asturias (99ppm) and the Basque Country (86ppm), medium penetration in the Eastern region (58.3ppm) and a relatively low penetration in communities such as Andalusia (42ppm), Madrid-Centre (45ppm) and Catalonia (42.5ppm). These differences have been reduced in recent years and, as such, in the last year (at 31 December 2010) we observed an increase in prevalence in the latter communities (51-55ppm) with respect to the mean for the whole study period.
Figure 5 shows distribution by age and sex, which was very homogeneous for all communities, with a higher concentration of patients between 40-60 and 60-80 years of age being observed. There was a higher number of males with respect to females, with a male index ranging from 1.27 in the Eastern region to 1.81 in Catalonia.
We observed a quite high degree of homogeneity in the aetiology of kidney disease (Figure 6); glomerular diseases, diabetic nephropathy, vascular nephropathy (hypertensive-arteriosclerotic) and polycystic kidney disease were the most common aetiologies.
The percentage of our patients included in the kidney transplant waiting list was quite high, with a mean value of 43%. Old age and associated comorbidities were the main reasons for exclusion.
Data on the technique
In recent years, we observed a progressive mean increase in APD use with respect to CAPD use, reaching almost 50% (range between 25%-65%). The broken red arrow in Figure 7 illustrates this fact. This increase in the use of an automatic technique was practically constant for all autonomous communities, although there were notable differences in its use amongst those with more extreme values (25% Eastern region and 65% Madrid-Centre).
The most commonly used catheters were Swan-Neck and double-cuff straight Tenckhoff catheters. The implantation technique was surgical in almost 80% of patients, although in the last few years, percutaneous implantation by the nephrologist has increased. The location was predominantly paramedian (80%).
Peritonitis: peritonitis rate per patient and year (Figure 8) varied between the different communities, although in general, it decreased slightly during the period studied (broken red line).
With respect to the causative germ, overall (mean of all data reported), the culture was positive for gram-positive germs in 57.3% and for gram-negative germs in 22%. Peritonitis was polymicrobial in 2.4% of patients, fungal in 2.7% and no growth was detected (sterile peritonitis) in 14.2%. These data were displayed by community in Figure 9.
Peritonitis (Figure 10) was mostly cured (80%), 8% had recurrences and it was necessary to withdraw the catheter in approximately 11% of cases. In just over 1% of cases, patients died due to peritoneal infection.
The reasons for withdrawing from the PD programme were distributed quite homogeneously between the different communities (Figure 11). In almost a third of cases, withdrawal was due to patient death (mean 28%), in a third, it was due to renal transplantation (mean 39%) and a third were transferred to HD (technique failure: mean 32%). The main reasons known/reported for transfer to HD continue to be peritonitis (in almost one third of cases: 31.1%), followed by ultrafiltration problems, insufficient dialysis or problems related to the peritoneal catheter (26%) (Figure 12).
Comorbidity and patient and technique survival
The main comorbidities at the start of the technique were cardiovascular disease (30.2%) and diabetes mellitus (24.2%). The mean Charlson Index was 4.6. We observed a slight increase in diabetic nephropathy in the latter years. All these data are presented as means and separately by autonomous community in Figure 13, which also displays diabetic nephropathy prevalence progression during the period studied and by geographic area.
The gross annual mortality rate for patients on PD has decreased continuously in recent years (Figure 14, broken red line) in almost all geographic areas that provided these data.
There was consistency between communities with regard to causes of death, cardiovascular disease (mean 39%) and infection (mean 22.5%) being the main causes.
Patient survival
Table 2 displays annual accumulated survival (in percentages) of patients by autonomous community. Bearing in mind that the data contributed by the Madrid-Centre and Basque Country regions only referred to patients with PD as the first RRT and that these data were taken into account for the calculation, mean survival was 92.2%, 82.8%, 74.2%, 64.8% and 57% after one, two, three, four and five years, respectively.
To analyse the influence of risk factors for patient survival present at the time the technique was introduced, we compared survival curves using the log-rank test in some communities and geographic regions such as Andalusia, Catalonia and the Eastern region (Figure 15). We observed that the presence of diabetes mellitus or cardiovascular disease at that time (p<.001 for Andalusia and Catalonia; p<.05 for the Eastern region) significantly influenced survival. Likewise, the period in which PD was started (before or after 2004) also had a statistically significant influence.
To assess the independence of the different factors on their influence on survival, the Cox multivariate proportional hazards model (Figure 15) was used both in Andalusia and in the Eastern region. The following factors significantly and independently had the worst survival rates: a) age (Andalusia and the Eastern region), b) cardiovascular disease (Andalusia and the Eastern region), c) diabetes mellitus (Andalusia and the Eastern region), d) CAPD compared to APD (Andalusia), e) starting PD in the first period studied, before 2004 (Andalusia) and f) residual renal function at the start of PD (the Eastern region).
Technique survival
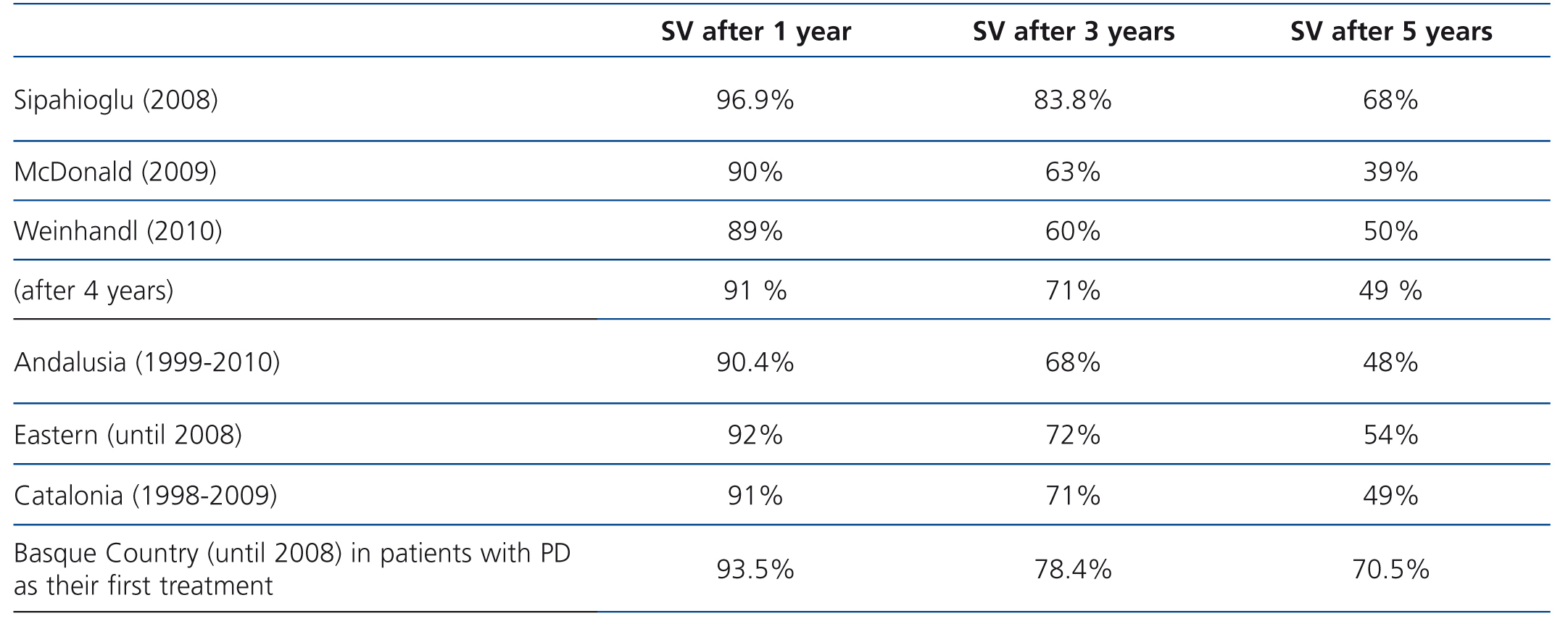
Lastly, Table 3 displays annual accumulated survival rates (in percentages) of the technique (patients were excluded for withdrawal due to death [apart from in Catalonia] or transplantation) and survival rates by autonomous community.
DISCUSSION
For the first time, this study collected a sufficient amount of data on RRT with PD, highly representative of the progression of this technique in Spain over the last decade and obtained a snapshot of the present day situation, showing epidemiological, demographic, technical, comorbidity and survival results, both for patients and technique. Methodological difficulties were mainly due to the different developmental processes of the autonomous registries that contributed data and this was the report’s main limitation.
PD growth in our country is discrete but clear. It is not homogeneous but it is universal for the different communities, with a 3.7% increase in the mean annual incidence rate between 2004 and 2010. This trend has been maintained over the last six years and is steady, without intermittent decreases. The Registry of the Spanish Society of Nephrology also observed this increase in PD incidence in recent years, although a slight decrease in HD incidence has also been observed, since transplantation has increased thanks to living donor and early transplantation.2 Likewise, an increased prevalence has been observed.
The mean overall age of the PD population, 54.7 years, is lower than that reported for HD patients. In terms of age distribution, there is prevalence in the 40-60 and 60-80 year old groups, as is the case for the other national and international registries.2-7
The most common known aetiologies of kidney disease in PD patients were glomerulonephritis (20.1 %), followed by diabetic nephropathy (17.2%), unlike in the National Registry for all RRT, which displays diabetes as an aetiology in 25% of patients. This difference may be explained by communities in the north of Spain, which are those that most use PD, having a lower incidence of diabetes.8 We can also argue that PD is being indicated less in older diabetic patients, given the lower survival rate communicated for this group in some studies, such as those of the American Registry9 or the Australia-New Zealand Registry.10
In the aetiology of our cooperative study, there was some discrepancy between communities in terms of labelling an aetiology as “unknown” or “other”, which may have corresponded to differences with regard to the definition of these concepts, and even to their inclusion within these groups or the vascular nephropathy group.
The inclusion of PD patients on transplant waiting lists is high and higher than for HD,1 which may be explained by the population being younger and having less comorbidity.
During the period observed, there was initially an increase in APD, and in the last few years, its use has stabilised at around 50%. These data are very similar to those of most developed countries.
The mean peritonitis rate in 2010 was 0.49 episodes/patient/year (approximately one episode every 25 months/patient), an incidence that had been decreasing slightly since previous years. These rates were lower than those indicated as the maximum amount acceptable by the Guidelines of the International Society for Peritoneal Dialysis, which is one episode every 18 months (0.67 per year at risk).11 Although the peritonitis rate depends on the characteristics of the population being treated, they are still above levels considered optimal of one episode every 40 to 50 months published by some authors.12,13
The most common reasons for discontinuing PD were distributed almost in three thirds, corresponding to patient death, renal transplantation and technique failure. This distribution in patient withdrawal was consistent with that reported previously by other authors.14 The fact that two registries (the Basque Country and Madrid-Centre) only collected data for patients who started RRT with PD logically resulted in noticeably higher withdrawal due to transplantation and lower mortality, and probably less technique failure, since there was greater residual renal function. We were not able to carry out a differential analysis of incident patients whose first treatment was PD because we did not have this data for many registries.
PD patient survival in Spain, measured both by the gross mortality rate and annual survival probability, has seen an overall improvement in the last decade. Overall survival is similar to that published by most European registries15-17 and higher than that of the American9,18 and Australia-New Zealand10 registries (Table 4).
Several factors have a more significant influence on this better prognosis. We know, due to multivariate studies carried out in some of the participating communities (Andalusia and the Eastern region), that comorbidities at the start of the technique, such as the patient’s age, diabetes, cardiovascular disease or loss of residual renal function have an unfavourable influence. By contrast, patient inclusion in PD programmes in more recent years has had a positive influence on survival. This is probably due to a better protection of the peritoneal membrane and its ultrafiltration capacity, the use of more biocompatible solutions that have a lower glucose concentration as an osmotic agent, such as icodextrin,19 particularly indicated in patients with a temporary or permanent hyperpermeable peritoneum or in patients with PD of long duration (both in CAPD and APD), or as a strategy in overhydrated patients, and lastly, due to better quality in the general practice of the technique: appropriate dialysis dose, patient monitoring, prevention and management of complications (peritonitis, etc.), prevention and treatment of metabolic and cardiovascular risks (dyslipidaemia, high blood pressure, fluid overload control, etc.).20-22
Likewise, technique survival has also increased, with mean figures above 50% after 5 years being observed, which is comparable to results of other registries and studies (Table 5).23,24 We understand that, as well as the better protection of the peritoneal membrane referred to above and the use of these solutions, accumulated experience on the technique, better patient selection for PD in hospitals, the decrease in peritonitis rates and its better treatment have also had an influence, amongst others.
KEY POINTS
Conflicts of interest
The authors declare that they have no conflicts of interest related to the contents of this article.

Table 1. Mean number of incident and prevalent patients and rate per million inhabitants by registry for the whole study period.

Table 2. Annual accumulated patient survival (%) by year and community.

Table 3. Accumulated annual technique survival (%) by year and community.

Table 4. Table comparing patient survival.

Table 5. International comparison. Accumulated annual technique survival (%) by year.

Figure 1. Population

Figure 10. Peritonitis progression by year and registry.

Figure 11. Percentages of the three main causes of withdrawal from peritoneal dialysis treatment by registry.

Figure 12. Reasons for transfer to haemodialysis.

Figure 13. Percentage of cardiovascular disease and diabetes at the start of the technique, and the Charlson index and percentage progression of diabetic nephropathy by year and community.

Figure 14. Progression of the gross annual mortality rate by year and registry.

Figure 15. Survival study (Andalusia, Catalonia and Eastern registries); survival curves by the log-rank test, in accordance with presence of diabetes, cardiovascular disease and the start period. Multivariate Cox proportional hazards model.

Figure 2. Number of new patients by year and registry (incidence).

Figure 3. Treatment background of peritoneal dialysis patients by different registries and the mean.

Figure 4. Prevalence by year and per million inhabitants. Comparison of the mean for the whole period with the year 2010.

Figure 5. Mean age and standard deviation, patient distribution by age and sex in accordance with the different registries.

Figure 6. Kidney disease aetiologies. Means for the whole period studied and by registry.

Figure 7. Progression in the use of automatic peritoneal dialysis for the whole period in the different registries.

Figure 8. Progression in peritonitis rate; patient/year means by registry. Mean rate in the last year.

Figure 9. Mean percentages of the different germs that cause peritonitis by community.



