




Diabetic renal lesions can only be diagnosed by kidney biopsy. These biopsies have a high prevalence of non-diabetic lesions. The aims of the study were to determine the predictability of non-diabetic nephropathy (NDN) in diabetics and study differences in survival and renal prognosis. In addition, we evaluated histological lesions and the effect of proteinuria on survival and renal prognosis in patients with diabetic nephropathy (DN).
Material and methodsA descriptive, retrospective study of kidney biopsies of diabetics between 1990 and 2013 in our centre.
Results110 patients were included in the study: 87 men (79%), mean age 62 years (50–74), mean serum creatinine 2.6mg/dl (0.9–4.3) and proteinuria 3.5g/24hours (0.5–6.5). 61.8% showed NDN, 34.5% showed DN and 3.6% showed DN+NDN. The most common NDN was IgA nephropathy (13.2%). In the multivariate analysis, creatinine (OR: 1.48, 1.011–2.172, p=0.044), proteinuria/24hours (OR: 0.813, 0.679–0.974, p=0.025), duration of diabetes (OR: 0.992, 0.987–0.998, p=0.004), age (OR: 1.068, 95% CI: 1.010–1.129, p=0.022), and diabetic retinopathy (OR: 0.23, 0.066–0.808, p=0.022) were independently associated with NDN. We did not find any differences in survival or renal prognosis. Concerning patients with DN, increased nodular mesangial expansion (p=0.02) and worse renal prognosis (p=0.004) were observed in nephrotic proteinuria as compared to non-nephrotic proteinuria. We did not find differences in patient survival.
ConclusionsThe most common cause of NDN was IgA nephropathy. Higher creatinine levels, shorter duration of diabetes, absence of diabetic retinopathy, lower proteinuria, and older age were risk factors for NDN. Patients with DN and nephrotic-range proteinuria had worse renal prognosis.
La afectación renal del diabético solo puede determinarse mediante biopsia renal, que presenta una elevada prevalencia de lesiones no diabéticas. Los objetivos del estudio fueron determinar la predictibilidad de nefropatía no diabética (NND) en diabéticos, estudiar diferencias de supervivencia y pronóstico renal, evaluar las lesiones histológicas en nefropatía diabética (ND) y el efecto de la proteinuria en la supervivencia y pronóstico renal en esta población.
Material y métodosEstudio descriptivo y retrospectivo de las biopsias renales de diabéticos entre 1990 y 2013 en nuestro centro.
ResultadosIncluimos a 110 pacientes: 87 hombres (79%), con una edad media de 62 años (50-74), creatinina sérica media de 2,6mg/dl (0,9-4,3) y proteinuria de 3,5g/24h (0,5-6,5). El 34,5% presentaban ND, el 61,8% NND y el 3,6% ND+NND. La NND más frecuente fue nefropatía IgA (13,2%). En el análisis multivariado, se asociaron de forma independiente a NND: edad (OR 1,068; IC 95%: 1,010-1,129; p=0,022), años de diabetes (OR: 0,992; 0,987-0,998; p=0,004), creatinina (OR: 1,48; 1,011-2,172; p=0,044), proteinuria de 24h (OR: 0.813; 0,679-0,974; p=0,025) y retinopatía diabética (OR: 0,23; 0,066-0,808; p=0,022). No hallamos diferencias de supervivencia ni de pronóstico renal. Entre los pacientes con ND, presentaban mayor expansión nodular mesangial los que tenían proteinuria nefrótica (p=0,02), así como peor pronóstico renal (p=0,004) comparado con proteinuria no nefrótica. No evidenciamos diferencias en la supervivencia del paciente.
ConclusionesLa causa más frecuente de NND fue nefropatía IgA. Los pacientes con mayor edad, creatinina, menor duración de diabetes, ausencia de retinopatía diabética y menor proteinuria presentan mayor riesgo de NND. Los pacientes con ND y proteinuria en rango nefrótico tuvieron peor pronóstico renal.
Diabetes mellitus (DM) is one of the most important health problems worldwide. In recent years, the prevalence of type 2 DM has increased in parallel to obesity and unhealthy lifestyles. In Spain, between 6% and 10% of the general population has DM. Between 6.3% and 7.4% of the Spanish healthcare budget is spent on diabetes care; this represents an annual cost of €1290–1476 per patient.1,2
Since the prevalence of DM has increased to epidemic proportions, the number of renal biopsies is also increasing. The lesions observed in these biopsies confirm either isolated diabetic nephropathy (DN), DN with non-diabetic nephropathy (NDN) or isolated NDN. Identification of these conditions affects patient's management and prognosis, especially if the diagnosis of NDN leads to a change in a patient's therapeutic strategy.3,4 Most prevalent NDN conditions in patients with DM are, focal and segmental glomerulosclerosis, IgA nephropathy and the membranous nephropathy.5 Therefore, research work has been conducted to find clinical factors that predict NDN in this population. Previous studies have observed that level of proteinuria, absence of diabetic retinopathy (DR), higher levels of haemoglobin, shorter duration of DM, acute renal failure at the time of renal biopsy, microhaematuria, DM treated with oral hypoglycaemics, lower blood sugar and less intima-media thickness are risk factors for NDN.3,5–9
Several studies have observed that renal survival was decreased in diabetic patients diagnosed of DN compared with patients with NDN.10,11 Moreover, the importance of renal biopsy in diabetic patients lies not only in the fact of differentiating DN from NDN, but also in studying histological lesions within DN.12 Amongst the different types of DN, the most advanced (type IV) presents higher proteinuria with a worse renal prognosis (RRT).13
The main aim of our study is to evaluate the prevalence and types of NDN in a consecutive cohort of biopsied diabetic patients and to find out whether there are factors that predict NDN. In addition, we plan to study whether there are differences in renal and patient survival according to the diagnosis obtained from the renal biopsy.
Material and methodsPatientsObservational retrospective study of pathological outcomes of patients with type 2 DM biopsied at Hospital del Mar from January 1990 to November 2013. In that period, a total of 565 renal biopsies of native kidneys were performed, 110 of which were from diabetic patients (19.4%).
These biopsies were processed by optical microscopy, immunofluorescence and electron microscopy, and they were performed by a renal pathologist. Renal biopsies were classified into 3 categories according to the findings: Isolated DN, NDN and the two conditions together.
Variables studiedA total of 113 variables were analysed: 58 (51.3%) were clinical and 55 laboratory values (48.7%). Patients demographic characteristics were recorded (age, gender and race), history of hypertension, dyslipidaemia, duration of DM, presence or absence of DR, diabetic neuropathy, ischaemic heart disease, previous stroke, peripheral vascular disease, malignancy, systemic disease, treatment with RAAS blockers, oral antidiabetics, insulin, statins and aldosterone antagonists.
While performing the renal biopsy, variables such as weight, height, systolic blood pressure and diastolic blood pressure were recorded. As for the laboratory data, renal function (serum creatinine in mg/dL and glomerular filtration rate (GFR) according to the MDRD-4ml/min/m2), urea in mg/dl, fasting blood glucose in mg/dL, HbA1c as a %, proteinuria (g/24h), microalbuminuria, urine protein/creatinine ratio, microhaematuria, autoimmune markers (ANA, anti-DNA, ANCA, anti-GBM and cryoglobulins) and viral serology (HCV, HBV and HIV) were all examined.
Also, the reasons for obtaining the renal biopsy were reviewed, together with the morphological characteristics found in the biopsy (number of glomeruli, method used in microscopy, diffuse or nodular mesangial expansion, global or segmental sclerosis, percentage of glomerulosclerosis and average GBM thickness) as well as the final diagnoses.
Finally, follow-up was done at 1, 3, 5 and 10 years post-biopsy. The variables evaluated were renal function as serum creatinine level and glomerular filtration rate (based on the MDRD), concentration of urea, fasting blood glucose, glycosylated haemoglobin (HbA1c), 24h proteinuria, microalbuminuria, urine protein/creatinine ratio, death and need for renal replacement therapy (RRT).
Statistical analysisFor the statistical analysis, IBM's SPSS Statistics version 19.0 was used. The inter-group comparison using univariate analysis was performed using a Student's t-test (continuous quantitative parametric variables) and the Wilcoxon signed-rank test (qualitative [categorical] paired variables).
In addition, a multivariate analysis of binary logistic regression was performed, using the diagnosis of NDN in the renal biopsy as a dependent variable. A ROC curve was calculated for potentially predictive variables for NDN compared with DN.
In relation with the survival analysis and commencement of renal replacement therapy, Kaplan–Meier curves and a log-rank test were used. Quantitative variables are expressed as mean and standard deviation and qualitative variables as a percentage. A p-value<0.05 was considered a statistically significant difference.
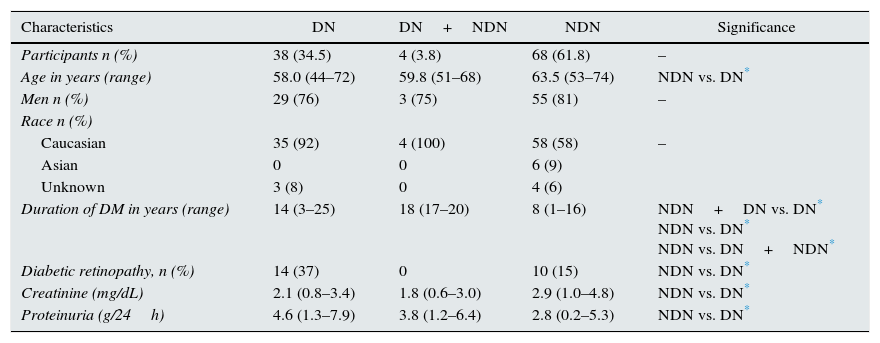
ResultsBaseline characteristics of the populationThe cohort's clinical and laboratory data were classified according to the renal biopsy result: DN, NDN or DN+NDN (Table 1). Mean age in the cohort was 62 (50–74), although the patients with DN were slightly younger. 79% (n=87) of the patients were men. Only 2.7% (n=3) of the patients had type 1 DM. The Caucasian race was the predominant one (n=97; 88%), followed by Asian (n=6; 5.5%). No statistically significant differences were observed between the 3 groups studied. Mean duration of DM was 10.6 (1.3–19.9) years. The patients with DN had a longer duration of diabetes compared with NDN patients (see Table 1).
Characteristics of the population.
| Characteristics | DN | DN+NDN | NDN | Significance |
|---|---|---|---|---|
| Participants n (%) | 38 (34.5) | 4 (3.8) | 68 (61.8) | – |
| Age in years (range) | 58.0 (44–72) | 59.8 (51–68) | 63.5 (53–74) | NDN vs. DN* |
| Men n (%) | 29 (76) | 3 (75) | 55 (81) | – |
| Race n (%) | ||||
| Caucasian | 35 (92) | 4 (100) | 58 (58) | – |
| Asian | 0 | 0 | 6 (9) | |
| Unknown | 3 (8) | 0 | 4 (6) | |
| Duration of DM in years (range) | 14 (3–25) | 18 (17–20) | 8 (1–16) | NDN+DN vs. DN* NDN vs. DN* NDN vs. DN+NDN* |
| Diabetic retinopathy, n (%) | 14 (37) | 0 | 10 (15) | NDN vs. DN* |
| Creatinine (mg/dL) | 2.1 (0.8–3.4) | 1.8 (0.6–3.0) | 2.9 (1.0–4.8) | NDN vs. DN* |
| Proteinuria (g/24h) | 4.6 (1.3–7.9) | 3.8 (1.2–6.4) | 2.8 (0.2–5.3) | NDN vs. DN* |
DN: diabetic nephropathy; NDN: non-diabetic nephropathy.
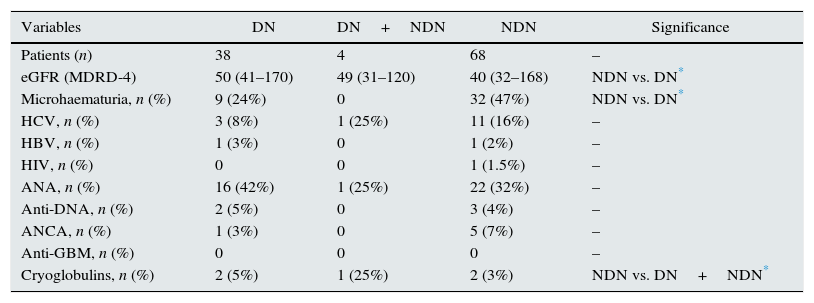
As for the lab data of systemic disease, no statistically significant differences were observed between the DN group and the NDN group (Table 2). As expected, the presence of microhaematuria was higher in the NDN as compared with the DN group (47.1 vs. 23.7%; p<0.05).
Urine sediment and relevant lab data from renal prebiopsy.
| Variables | DN | DN+NDN | NDN | Significance |
|---|---|---|---|---|
| Patients (n) | 38 | 4 | 68 | – |
| eGFR (MDRD-4) | 50 (41–170) | 49 (31–120) | 40 (32–168) | NDN vs. DN* |
| Microhaematuria, n (%) | 9 (24%) | 0 | 32 (47%) | NDN vs. DN* |
| HCV, n (%) | 3 (8%) | 1 (25%) | 11 (16%) | – |
| HBV, n (%) | 1 (3%) | 0 | 1 (2%) | – |
| HIV, n (%) | 0 | 0 | 1 (1.5%) | – |
| ANA, n (%) | 16 (42%) | 1 (25%) | 22 (32%) | – |
| Anti-DNA, n (%) | 2 (5%) | 0 | 3 (4%) | – |
| ANCA, n (%) | 1 (3%) | 0 | 5 (7%) | – |
| Anti-GBM, n (%) | 0 | 0 | 0 | – |
| Cryoglobulins, n (%) | 2 (5%) | 1 (25%) | 2 (3%) | NDN vs. DN+NDN* |
DN: diabetic nephropathy; NDN: non-diabetic nephropathy.
Overall, the main reason for renal biopsy was nephrotic syndrome or elevated proteinuria (n=27; 25%), followed by suddenly impaired renal function in patients with stable renal function (n=15; 14%), nephrotic proteinuria without DR (n=14; 13%) and proteinuria greater than 1g in diabetics with less than 5 years’ history of diabetes (n=12; 11%), amongst others (Fig. 1). It should be noted that acute renal failure was observed in 7 patients (6.4%), but only in the NDN group.
Results of renal biopsies in non-diabetic nephropathy
Isolated DN was detected in 38 of 110 diabetic patients biopsied. In the rest (72 patients), NDN was detected. The most common diagnosis of NDN was IgA nephropathy (n=9; 13.2%), followed by benign nephrosclerosis (n=6; 8.8%), focal and segmental glomerulonephritis (n=5; 7.4%), membranous glomerulonephritis (n=4; 5.9%), chronic interstitial nephropathy (n=4; 5.9%) and other less common ones (Fig. 2). 13.6% (n=15) of the renal biopsies were unclassifiable due to insufficient sample for diagnosis.

Diagnoses from renal biopsy: distribution of the number of patients according to diagnosis in renal biopsy. F&S: focal and segmental; GN: glomerulonephritis; MPGN: membranoproliferative glomerulonephritis; NAS: nephroangiosclerosis; AIN: acute interstitial nephritis; CIN: chronic interstitial nephritis; ATN: acute tubular necrosis.
The cohort of patients diagnosed with DN in the renal biopsy was studied. Regarding histological findings in the renal biopsy, patients with DN showed diffuse mesangial expansion (n=35; 83.3%), nodular mesangial expansion (n=22; 52.4%), global sclerosis (n=32, 76.2%), segmental sclerosis (n=11; 26.2%) and glomerulosclerosis (n=35; 83.3%).
Renal biopsies were distributed as classified based on the study by Fioretto et al.14 Thus, we found that a total of 9 patients (22%) were in category CI, 22 patients (53.7%) in category CII and 10 patients (24.4%) in category CIII. One patient was impossible to classify.
We studied the differences between groups depending on the degree of proteinuria (nephrotic≥3.5g/24h [n=2] and non-nephrotic<3.5g/24h [n=17]), and found that patients with nephrotic proteinuria had more nodular expansion as compared with those who had non-nephrotic proteinuria (69.5 vs. 29.4%; p=0.02).
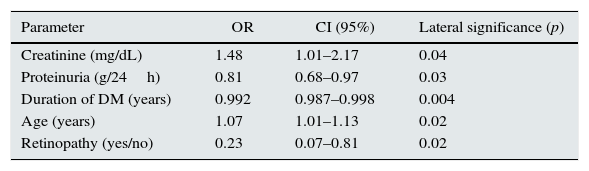
Predictive factors for non-diabetic nephropathyIn order to identify predictive factors of NDN, a multivariate binary logistic regression analysis (Table 3) was performed. Risk factors included a high level of serum creatinine, age of the patient, less proteinuria in 24h collection, shorter duration of diabetes and no DR (Table 3). Although we found significant differences in presence of haematuria (DN 9 vs. 32 cases) in the multivariate analysis, it was not significant.
Predictive factors for non-diabetic nephropathy in diabetic patients.
| Parameter | OR | CI (95%) | Lateral significance (p) |
|---|---|---|---|
| Creatinine (mg/dL) | 1.48 | 1.01–2.17 | 0.04 |
| Proteinuria (g/24h) | 0.81 | 0.68–0.97 | 0.03 |
| Duration of DM (years) | 0.992 | 0.987–0.998 | 0.004 |
| Age (years) | 1.07 | 1.01–1.13 | 0.02 |
| Retinopathy (yes/no) | 0.23 | 0.07–0.81 | 0.02 |
Multivariate binary logistic regression analysis. Dependent variable: non-diabetic nephropathy.
95% CI: confidence interval of 95%; OR: odds ratio.
The discriminative ability of the model showed an ROC curve 0.805 (95% CI: 0.708–0.902) (Fig. 3).

An analysis using ROC curves for each of the variables was performed, showing the cut-off point of each one with greater specificity and sensitivity. We therefore obtained an increased risk of NDN when creatinine was greater than 1.58mg/dL, proteinuria under 3.15g/24, age over 53 years and duration of DM under 10 years.
Renal prognosis and survivalA survival analysis of patients with diabetes and renal prognosis (need for RRT) was performed. The need for RRT was 33%. It was twice as much in NDN compared with DN (11% n=4 vs. 22% n=16), without statistical significance. At the time of renal biopsy, one patient (2.6%) in the DN group and 9 (12.5%) in the NDN group started haemodialysis. During the follow-up period, 5 patients in the DN group required RRT (13.2%), 20 in the NDN group (29.4%), and none in the group with both conditions. Overall patient mortality was 23% (n=25), 5% (n=5) of these in the DN group and 18% (n=20) in the NDN group. No deaths were observed in the DN+NDN group in the follow-up period. No differences in renal or patient survival, or between cohorts studied, were observed (Fig. 4A and B).
 Start of RRT. (B) Mortality. No statistically significant differences were observed between the groups. DN: diabetic nephropathy; NDN: non-diabetic nephropathy; RRT: renal replacement therapy. Renal and patient survival curve according to proteinuria in patients with DN. Analysis using Kaplan–Meier curves of the different groups of diabetics with diabetic nephropathy divided according to range of proteinuria (nephrotic or non-nephrotic). (C) Start of RRT. (D) Mortality. Statistically significant differences (p=0.004) were observed at start of RRT, observing a higher incidence in the group with nephrotic proteinuria. As for patient survival, no statistically significant differences were observed.")
Renal and patient survival curves in all groups studied. Analysis using Kaplan–Meier curves of the different groups divided according to renal biopsy diagnoses. (A) Start of RRT. (B) Mortality. No statistically significant differences were observed between the groups. DN: diabetic nephropathy; NDN: non-diabetic nephropathy; RRT: renal replacement therapy. Renal and patient survival curve according to proteinuria in patients with DN. Analysis using Kaplan–Meier curves of the different groups of diabetics with diabetic nephropathy divided according to range of proteinuria (nephrotic or non-nephrotic). (C) Start of RRT. (D) Mortality. Statistically significant differences (p=0.004) were observed at start of RRT, observing a higher incidence in the group with nephrotic proteinuria. As for patient survival, no statistically significant differences were observed.
Next, the group of patients diagnosed with DN based on Fioretto's scheme was analysed, and no differences between the various categories of renal and patient survival were observed.
Proteinuria at the time of biopsy in patients with DN was then studied (n=41). 58.5% (n=24) had nephrotic-range proteinuria (≥3.5g/24h) and 39.5% (n=17) had non-nephrotic proteinuria. 41.5% (n=17) required RRT. As expected, the patients with nephrotic-range proteinuria had an increased incidence of end-stage kidney disease as compared with the group of patients with non-nephrotic proteinuria (45.8% n=11 vs. 6.6% n=1; p=0.004). No statistically significant differences in patient mortality were observed (12.5% n=3, vs. 11.8% n=2; p=NS) (Fig. 4C and D).
DiscussionIn our population of patients with DM and with a renal biopsy, the majority had NDN. The most common diagnosis of NDN was IgA nephropathy. Elevated serum creatinine, lower degree of 24h proteinuria, shorter duration of diabetes, absence of DR and older age were risk factors for NDN in diabetic patients in whom a renal biopsy was performed. No differences in patient survival or renal prognosis were observed based on the result of the renal biopsy. Patients with nephrotic proteinuria had a worse renal prognosis as compared with the group with non-nephrotic proteinuria.
Sharma et al.3 studied 620 patients with DM biopsied at 2 centres in the United States, and found that 37% showed isolated DN, 26.4% DN and NDN, and 35.4% isolated NDN. In our study, the percentage of patients with isolated DN was similar (34.5%); however, 61.8% had isolated NDN, and the percentage of combined diagnoses of DN and NDN was minimal.
In patients with diabetes, a renal biopsy is usually performed when NDN is suspected.15,16 The most common reasons for indicating renal biopsy in our series were similar to those already known and published: impaired renal function with no apparent cause, presence of microhaematuria, increased proteinuria in the absence of DR, presence of nephrotic syndrome, increased proteinuria with DM of less than 5 years’ history and presence of nephritic syndrome.17–19
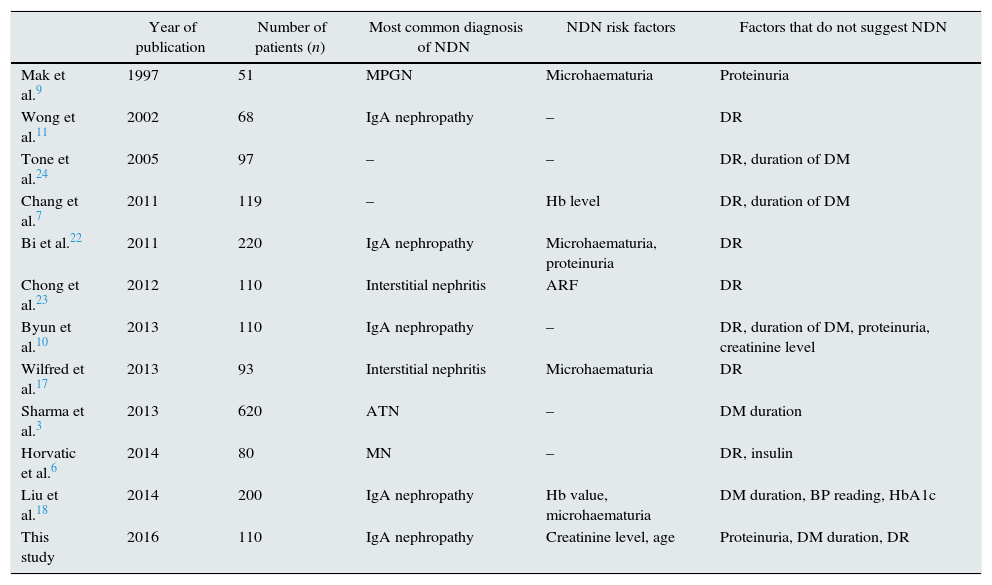
As for the results in the renal biopsy, in the studies published, the conditions most frequently found in diabetic patients with NDN are: IgA nephropathy10,11,18,20–22 and interstitial nephritis7,17,19,23 (see Table 4). In our cohort, the most common condition of NDN was IgA nephropathy. However, Sharma et al., who analysed the largest cohort to date with a total of 620 patients, found that the most common finding was acute tubular necrosis. These results may be attributed to the high rate at which renal biopsies are indicated for acute renal failure.3
Comparison of previous studies in which NDN was studied in diabetic patients diagnosed by renal biopsy.
| Year of publication | Number of patients (n) | Most common diagnosis of NDN | NDN risk factors | Factors that do not suggest NDN | |
|---|---|---|---|---|---|
| Mak et al.9 | 1997 | 51 | MPGN | Microhaematuria | Proteinuria |
| Wong et al.11 | 2002 | 68 | IgA nephropathy | – | DR |
| Tone et al.24 | 2005 | 97 | – | – | DR, duration of DM |
| Chang et al.7 | 2011 | 119 | – | Hb level | DR, duration of DM |
| Bi et al.22 | 2011 | 220 | IgA nephropathy | Microhaematuria, proteinuria | DR |
| Chong et al.23 | 2012 | 110 | Interstitial nephritis | ARF | DR |
| Byun et al.10 | 2013 | 110 | IgA nephropathy | – | DR, duration of DM, proteinuria, creatinine level |
| Wilfred et al.17 | 2013 | 93 | Interstitial nephritis | Microhaematuria | DR |
| Sharma et al.3 | 2013 | 620 | ATN | – | DM duration |
| Horvatic et al.6 | 2014 | 80 | MN | – | DR, insulin |
| Liu et al.18 | 2014 | 200 | IgA nephropathy | Hb value, microhaematuria | DM duration, BP reading, HbA1c |
| This study | 2016 | 110 | IgA nephropathy | Creatinine level, age | Proteinuria, DM duration, DR |
DM: diabetes mellitus; MPGN: membranoproliferative glomerulonephritis; Hb: haemoglobin; MN: membranous nephropathy; NDN: non-diabetic nephropathy; ATN: acute tubular necrosis; BP: blood pressure; DR: diabetic retinopathy.
Several studies have focused on analysing the risk factors for NDN in biopsied diabetic patients and confirmed a shorter duration of diabetes,3,6,7,10,11,17,18,24 lower blood pressure,17 absence of retinopathy,7,10,18,22,23 elevated haemoglobin,7,18 lower glycosylated haemoglobin,18 presence of microhaematuria,9,10,17,18,22 elevated proteinuria,22 decreased serum creatinine,10 or treatment with oral hypoglycaemics.11,24 In other studies, however, NDN was associated with the presence of acute renal failure23 or lower proteinuria.9,10 In our study we observed that NDN risk factors are elevated serum creatinine and advanced age.
We found that independent protective factors against development of NDN were, low degree of proteinuria over 24h, the long duration of diabetes and the presence of DR. Our model obtained an ROC curve with an area under the curve greater than 0.80, thus confirming its reliability. Liang et al. performed a meta-analysis that included a total of 63 studies with 2322 patients to study the risk factors for developing NDN. As with our study, they found that absence of DR, shorter duration of DM and a low level of glycosylated haemoglobin were predictors of NDN. Moreover, in their study, lower blood pressure and lower serum cholesterol also proved to be predictors of NDN.25
The presence of microhaematuria is risk factor of NDN in biopsied patients with DM.9,10,17,18,22 In our study, although the number of patients presenting with haematuria in the NDN group was higher than in the DN group; however by multivariate analysis this factor was not significant as an independent factor in developing NDN.
Several studies have focused on the renal prognosis in diabetic patients with DN vs. NDN.7,10,11,26 In these studies, patients with renal NDN had a better prognosis in terms of progression to chronic renal disease requiring RRT. Our results are the opposed since in our cohort, biopsied diabetic patients diagnosed with NDN had a tendency towards a worse renal prognosis.
In our patients at the time of the biopsy, the creatinine level in the NDN group was higher than in the DN group. This is in contrast to previous studies7,11 in which patients with DN the initial renal function was worse than with NDN. In one of these studies, although the creatinine level in the NDN group was higher than in the DN group, renal prognosis was worse in the DN group.10 One possible explanation might be that the DN group had a higher degree of proteinuria compared with the NDN group, although the differences were not significant.
In the study of differences in patient survival in the NDN group vs. the DN group, no differences were observed. To date, there are no studies focused on analysing survival in diabetic patients based on the diagnosis from a renal biopsy.
One-third of the patients in our cohort were diagnosed with DN. The natural history of DN in type 2 DM is not well established, unlike that of type 1 DM. Changes in indolent glucose metabolism up to the diagnosis of DM are used to establish various periods of time from change to change. This is why at the time of diagnosis of type 2 DM, DN may manifest as micro- or macroalbuminuria.
However, 20 years after the onset of microalbuminuria, only 20% will progress to chronic kidney disease.1 Risk factors for progression to end-stage kidney disease in diabetic kidney disease have been described, and include a family history of DM, smoking, blood glucose and lipid levels, blood pressure and urinary albumin excretion, as well as new emerging biochemical markers.27
In 2010, Taervert et al. performed a histological classification of DM in which a total of 5 classes were differentiated, ranging from absence of lesions under a light microscope to diffuse glomerulosclerosis.28 By specifically analysing which kind of lesions are evident based on degree of proteinuria, it has been shown that an increase in the mesangial area occurs when the degree of proteinuria increases.12 In this regard, in our study, the most common histological lesion was diffuse mesangial expansion. In addition, we observed that patients with DN having a renal biopsy with nephrotic proteinuria showed greater nodular expansion compared with those with non-nephrotic proteinuria in the population diagnosed with DN. All of this is consistent with previous results published by others.12
Several studies have examined the difference in renal prognosis, as classified by Taervert, in patients with DN. Amongst them, Mise et al., with a total of 205 biopsies with a DN diagnosis, and then An et al., with a total of 396 biopsies, showed that patients who in their renal biopsy have DN class IV had a worse renal prognosis than the other classes.13,29
In addition, renal prognosis was analysed according to degree of proteinuria. As with the results of the two studies mentioned above, in our cohort we saw that patients with nephrotic proteinuria have a worse renal prognosis, which probably corresponds to nephropathy class III–IV, where a higher degree of proteinuria is observed. Shimizu et al., in a cohort of 260 diabetic nephropathy cases, analysed the difference in renal prognosis depending on degree of proteinuria, finding that the greater the degree of proteinuria, the higher the incidence of renal events in patients with a glomerular filtration rate greater than 60ml/min as well as in those with less than 60ml/min.30 All of this is consistent with our results. In the same study mentioned above, the differences in mortality were also analysed according to degree of proteinuria, and an increase in mortality with proteinuria in patients with a glomerular filtration rate less than 60ml/min/m2 was observed. However, this increase was not observed in patients with a glomerular filtration rate greater than 60ml/min/m2. In contrast, in our study we observed no differences according to glomerular filtration rate or serum creatinine level.
Finally, biopsies were classified according Fioretto's scheme (categories CI, CII and CIII), but there were no significant differences in either patient or renal survival.
ConclusionsA significant percentage of patients with diabetes (2/3) presented with NDN in renal biopsy. Amongst diabetic patients with renal involvement it is necessary to detect those with NDN, as they have a different prognosis for kidney disease and may benefit from different therapeutic strategies. Classically and according to the guidelines for managing diabetic patients, renal biopsy is indicated when the presence of another condition is suspected according to the clinical course and serum and urinary lab data.31 However, a better understanding of diabetic patients treated by renal biopsy and their clinical and laboratory characteristics may help in decision-making in routine clinical practice. The prognosis for DN differs depending on the type of lesions found in a renal biopsy. Few studies have focused on the study of routine renal biopsy in patients with DM. We believe that further studies are necessary to elucidate the importance and renal prognosis of biopsies in diabetic patients with suspected DN.
Authors/contributorsSB and MJS have also contributed to the study.
Conflicts of interestThe authors declare that they have no conflicts of interest.
Part of this study received funding from ISCIII-FEDER PI14/00557 and ISCIII-RETICS REDinREN RD12/0021/0024.
Please cite this article as: Bermejo S, Soler MJ, Gimeno J, Barrios C, Rodríguez E, Mojal S, et al. Factores predictivos de nefropatía no diabética en pacientes diabéticos. Utilidad de la biopsia renal. Nefrologia. 2016;36:535–544.



