


Dear Editor:
Acute renal failure is a relatively frequent complication in patients with multiple myelomas (MM). This complication is associated with a poor prognosis and shortened survival time.
There are many factors in its aetiology, including reduced volume, hypercalcaemia, tubulointerstitial nephritis and more rarely, hyperviscosity syndrome. However, the main cause of kidney damage is the excess of monoclonal production of light chains that cause obstruction on the tubular level; this is known as myeloma kidney.2
The main treatment for these patients is chemotherapy, which aims to reduce production of light chains. In those cases where there is renal failure secondary to intratubular deposits, haemodialysis and plasmapheresis constitute an adjuvant treatment option. The objective of these techniques is to eliminate the greater part of the light chains circulating in the plasma.
In the literature, evidence for the benefits of treatment with plasma exchange techniques is limited, although several studies do exist that show that plasmapheresis is more effective than haemodialysis.1
We present a case of acute renal failure secondary to myeloma kidney, with a good response to plasmapheresis, which led to recovery of renal function.
Clinical case
Female patient aged 59 years, with a history of hypertension and type-2 diabetes mellitus, diagnosed with monoclonal IgG gammopathy with progression subsequent to IgG lambda multiple myeloma. From the moment of diagnosis, various chemotherapy treatment schemes were administered, with no response. Six years after diagnosis, we were consulted for acute renal failure with conserved diuresis. The patient was in stage IIIB, with analysis showing Bence Jones proteinuria and plasma creatinine of 7mg/dl.
Replacement therapy with combined conventional haemodialysis and plasmapheresis was initiated on a schedule of three sessions per week for one month, and one session per week thereafter. Initially, a plasma exchange volume of 3L was used, which was later increased to 4Lwhen the patient changed to weekly sessions. The substitution liquid used was 5% albumin. Treatment resulted in a reduction in plasma creatinine of more than 50% and stable values were maintained, which allowed us to discontinue replacement therapy with haemodialysis.
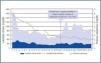
Plasma levels of lambda light chains at the moment when treatment began were higher than 1,750mg/dl. With the start of adjuvant treatment, reductions of more than 60% were obtained in each plasmapheresis session. As we observe from figure 1, a rebound effect occurs between sessions, but the pre-plasmapheresis values are lower each time.
At present, the patient continues with chemotherapy with little response, and is awaiting evaluation for a bone marrow transplant. Meanwhile, she is continuing with adjuvant treatment with plasmapheresis without major complications and with a stable renal function.
Discussion
The evidence when evaluating the effectiveness of plasmapheresis in patients with acute renal failure secondary to myeloma kidney is still debateable. However, many studies show an improvement in renal function and thus demonstrate the beneficial role played by plasmapheresis as an adjuvant treatment.
There is still no consensus in the literature regarding the number of sessions, the interval or the treatment dose.
In our patient’s case, it was determined according to the clinical evolution and it is still being maintained, as we still hope for a response to the chemotherapy.
Given the recovery of renal function, despite the persistent production of light chains, we can say that plasmapheresis is a treatment option for acute renal failure secondary to myeloma kidney.

Figure 1.



