



Steroid minimization after kidney transplantation has become more widely practiced as transplant clinicians seek the potential benefits such as reduced cardiovascular risk factors, improved growth in pediatric patients, and improved compliance with the immunosuppression regimen. Steroid avoidance (i.e. no steroids after the first week) is generally favored compared to later withdrawal. Induction therapy is routine in this setting, frequently rabbit antithymocyte globulin (rATG, Thymoglobulin®) or off-license use of alemtuzumab. Direct comparisons of steroid minimization regimens versus standard steroid regimens are rare. However, the available data show that the risk of acute rejection is low when rATG or alemtuzumab induction is given to support steroid-avoidance regimens after kidney transplantation. Steroid avoidance may be inadvisable in patients at high immunological risk or at risk of recurrent glomerular disease. Steroid withdrawal after day 8 may be possible without additional risk of rejection in patients given rATG induction, but while encouraging, the data are too sparse for firm conclusions. In summary, steroid avoidance may be beneficial for patients after renal transplantation, with the potential to avoid or reduce steroid-related comorbidities. Whilst depleting induction therapy could be the treatment of choice, results of prospective randomized, controlled studies are eagerly awaited.
La minimización de esteroides después del trasplante renal constituye una práctica muy extendida en la búsqueda de potenciales beneficios cardiovasculares, mejor crecimiento en pacientes pediátricos o aumento de la adherencia al tratamiento inmunosupresor. El uso de inducción depletiva con ATG de conejo o alemtuzumab puede contribuir a evitar el uso de esteroides o, al menos, a permitir su suspensión precoz. Esta estrategia se ha revisado en la literatura, añadiendo la opinión de expertos al análisis. La suspensión de esteroides muy precoz (antes de la primera semana) parece preferirse a la suspensión más tardía. En ese contexto, la inducción preventiva es la práctica más utilizada, habitualmente con globulina antitimocítica de conejo (rATG, timoglobulina) o alemtuzumab (en uso fuera de indicación). Son raras las comparaciones directas de los regímenes de minimización de esteroides con los de uso estándar. Sin embargo, los datos disponibles muestran que el riesgo de rechazo agudo es bajo cuando se administra rATG o alemtuzumab para facilitar la suspensión muy precoz de esteroides. Esta práctica puede ser menos aconsejable en pacientes con alto riesgo inmunológico o predispuestos a una recurrencia de la enfermedad glomerular de base. La suspensión de esteroides a partir del día 8 es factible sin que el riesgo de rechazo aumente en pacientes tratados con rATG. No obstante, y aunque los datos disponibles así lo indican, requieren confirmación definitiva. En conclusión, la minimización extrema de esteroides puede ser beneficiosa en pacientes que reciben un trasplante renal, con la ventaja que supone evitar o reducir la comorbilidad asociada con ese tratamiento. Si bien la inducción depletiva podría ser el tratamiento de elección en ese contexto, son necesarios nuevos ensayos aleatorizados controlados que lo confirmen.
Steroid-sparing immunosuppressive regimens are widely used after kidney transplantation as clinicians seek to minimize steroid-related adverse events.1 Rapid steroid discontinuation lowers the rates of cataracts, vascular necrosis and cytomegalovirus infection2 and may improve growth in children.3 Cardiovascular benefits are less well established, although positive effects have been observed for lipid profile and weight gain.4,5 Generally, it is difficult to demonstrate differences in randomized trials in unselected populations, and studies of steroid minimization regimens have often not reported steroid-related side effects, or were underpowered to demonstrate a significant difference. However, even if data remain unconvincing about reduced cardiovascular risk, the non-cardiovascular side effects of chronic steroid therapy require costly management6 and some, such as weight gain, can adversely affect patient compliance7,8 with potential consequences for graft outcomes.
Strategies for steroid minimization comprise either ‘steroid avoidance’ (or ‘steroid-free’) regimens, which will be defined here as no intravenous (i.v.) or oral steroids after the first 1–2 weeks post-transplant, or steroid withdrawal, i.e. steroid discontinuation after weeks 1–2.4,9,10
Steroid avoidance protocols have become increasingly popular in recent years. Steroid-free immunosuppression without induction therapy has been attempted after kidney transplantation using a calcineurin inhibitor (CNI)-based maintenance regimen, but randomized trials showed acute rejection to be significantly more frequent4,11,12 or more severe13 than with standard steroids. A series of randomized trials comparing steroid avoidance versus ongoing steroid therapy in selected populations receiving interleukin-2 receptor (IL-2R) induction have reported mixed results.14–18 High rates of biopsy-proven acute rejection (BPAR) were observed in the FREEDOM study for patients given basiliximab induction with cyclosporine (CsA), mycophenolic acid (MPA) and either a single i.v. dose of steroids (31.5% BPAR at 1 year) or steroids to day 7 (26.1%).19 Other researchers have found no significant effect on BPAR using steroid avoidance with IL-2R antagonist induction, especially with concomitant tacrolimus,15,16 although BPAR may occur earlier.16
Many centers, particularly in the US, instead employ lymphocyte-depleting induction when steroid-free therapy is planned, an approach that may be partly based on experience from conventional immunosuppressive regimens. Randomized trials of patients at low or moderate immunological risk given standard steroids have shown comparable rejection rates using induction with an IL-2R antagonist or rabbit antithymocyte globulin (rATG),19–22 but for high-immunologic risk populations both the overall rejection rate and the incidence of steroid-resistant rejection is lower with rATG.23,24 This may have encouraged more frequent selection of rATG or another depleting agent when attempting steroid avoidance: almost 90% of kidney transplantation patients who are discharged on a steroid-free regimen in the US receive a lymphocyte-depleting induction agent,25 with the remaining 10% given IL-2R antagonist induction.
Steroid withdrawal after the first week post-transplant tends to be regarded with more caution. A meta-analysis of eight randomized trials found that steroid withdrawal after week 1 significantly increased both acute rejection and graft loss.26 In a further meta-analysis, in which only those trials that included CNI therapy with mycophenolate mofetil (MMF) were analyzed, graft loss was minimized, but the risk of acute rejection was still higher following steroid withdrawal.27 The Kidney Disease: Improving Global Outcomes (KDIGO) recommendations suggest that in low-risk patients given induction therapy, steroids can be discontinued during week 1.28 If steroids are administered beyond the first week post-transplant, however, KDIGO suggests that they be maintained thereafter.28 This may, however, be an oversimplification. A recent Cochrane systematic review concluded that although late (month 3–6) steroid withdrawal is associated with increased rejection rates in CsA-treated patients (risk ratio 1.61, p=0.0018), this does not appear to be the case when tacrolimus is given with MMF (risk ratio 0.82, p=0.29).9,10,29,30 Equally, the safety of steroid withdrawal may be affected by the choice of induction therapy.
This article reviews the evidence relating to lymphocyte-depleting induction with rATG or alemtuzumab to support steroid avoidance or withdrawal in kidney transplant recipients. It should be borne in mind that alemtuzumab in solid organ transplantation is used off-label, and the indication is not likely to be forthcoming.
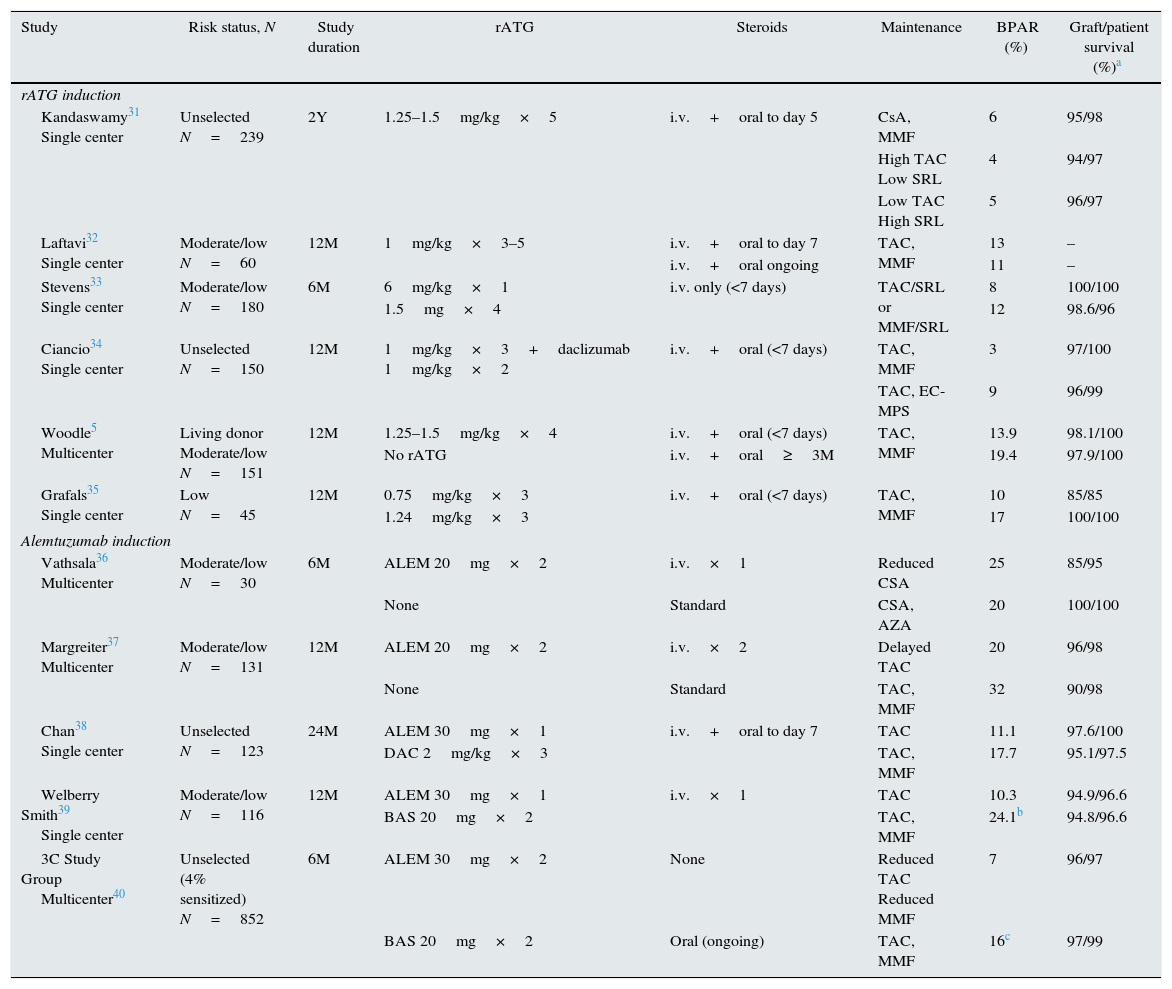
Lymphocyte-depleting induction and steroid-free immunosuppressionrATG inductionRandomized trials relating to steroid-free treatment of kidney transplant patients given rATG induction are relatively rare, with only sparse data directly comparing steroid-free therapy versus standard steroids (Table 1). One may deduce, however, that steroid-free immunosuppression is safe, as shown in trials such as the one published in 2005 by Kandaswamy et al.31 In that study, 239 first or second kidney transplant recipients all received rATG (1.25–1.5mg/kg for five doses) with a single dose of i.v. steroids then oral steroids to day 5.31 The trial did not compare steroid-free with steroid conventional therapy: instead, all patients received the very short five-day steroid regimen. They were randomized to one of three maintenance regimens: CsA with MMF, high tacrolimus (trough level 8–12ng/mL) with low sirolimus (3–7ng/mL), or low tacrolimus (3–7ng/mL) with high sirolimus (8–12ng/mL), and followed to month 24. Rates of BPAR were low and similar in all groups (4–6%); graft and patient survival was also excellent (Table 1). At month 24, 75%, 90% and 83% of patients, respectively, remained steroid-free, and the incidence of steroid-related events (post-lymphoproliferative disease, new-onset diabetes mellitus [NODAT], osteonecrosis and viral infection) was encouragingly low. There were no major differences in complications between groups, other than a higher rate of wound healing complications in the high sirolimus arm (p=0.02).31 These results suggest that any of these steroid-free maintenance protocols is effective when given with rATG induction, even in an unselected cohort of patients.
Randomized trials of rATG or alemtuzumab induction with steroid avoidance in kidney transplantation.
| Study | Risk status, N | Study duration | rATG | Steroids | Maintenance | BPAR (%) | Graft/patient survival (%)a |
|---|---|---|---|---|---|---|---|
| rATG induction | |||||||
| Kandaswamy31 Single center | Unselected N=239 | 2Y | 1.25–1.5mg/kg×5 | i.v.+oral to day 5 | CsA, MMF | 6 | 95/98 |
| High TAC Low SRL | 4 | 94/97 | |||||
| Low TAC High SRL | 5 | 96/97 | |||||
| Laftavi32 Single center | Moderate/low N=60 | 12M | 1mg/kg×3–5 | i.v.+oral to day 7 | TAC, MMF | 13 | – |
| i.v.+oral ongoing | 11 | – | |||||
| Stevens33 Single center | Moderate/low N=180 | 6M | 6mg/kg×1 | i.v. only (<7 days) | TAC/SRL or MMF/SRL | 8 | 100/100 |
| 1.5mg×4 | 12 | 98.6/96 | |||||
| Ciancio34 Single center | Unselected N=150 | 12M | 1mg/kg×3+daclizumab 1mg/kg×2 | i.v.+oral (<7 days) | TAC, MMF | 3 | 97/100 |
| TAC, EC-MPS | 9 | 96/99 | |||||
| Woodle5 Multicenter | Living donor Moderate/low N=151 | 12M | 1.25–1.5mg/kg×4 | i.v.+oral (<7 days) | TAC, MMF | 13.9 | 98.1/100 |
| No rATG | i.v.+oral≥3M | 19.4 | 97.9/100 | ||||
| Grafals35 Single center | Low N=45 | 12M | 0.75mg/kg×3 | i.v.+oral (<7 days) | TAC, MMF | 10 | 85/85 |
| 1.24mg/kg×3 | 17 | 100/100 | |||||
| Alemtuzumab induction | |||||||
| Vathsala36 Multicenter | Moderate/low N=30 | 6M | ALEM 20mg×2 | i.v.×1 | Reduced CSA | 25 | 85/95 |
| None | Standard | CSA, AZA | 20 | 100/100 | |||
| Margreiter37 Multicenter | Moderate/low N=131 | 12M | ALEM 20mg×2 | i.v.×2 | Delayed TAC | 20 | 96/98 |
| None | Standard | TAC, MMF | 32 | 90/98 | |||
| Chan38 Single center | Unselected N=123 | 24M | ALEM 30mg×1 | i.v.+oral to day 7 | TAC | 11.1 | 97.6/100 |
| DAC 2mg/kg×3 | TAC, MMF | 17.7 | 95.1/97.5 | ||||
| Welberry Smith39 Single center | Moderate/low N=116 | 12M | ALEM 30mg×1 | i.v.×1 | TAC | 10.3 | 94.9/96.6 |
| BAS 20mg×2 | TAC, MMF | 24.1b | 94.8/96.6 | ||||
| 3C Study Group Multicenter40 | Unselected (4% sensitized) N=852 | 6M | ALEM 30mg×2 | None | Reduced TAC Reduced MMF | 7 | 96/97 |
| BAS 20mg×2 | Oral (ongoing) | TAC, MMF | 16c | 97/99 | |||
ALEM, alemtuzumab; AZA, azathioprine; BAS, basiliximab; BPAR, biopsy-proven acute rejection; CsA, cyclosporine; DAC, daclizumab; EC-MPS, enteric-coated mycophenolate sodium; i.v., intravenous; MMF, mycophenolate mofetil; rATG, rabbit antithymocyte globulin; SRL, sirolimus; TAC, tacrolimus.
One randomized trial that compared rATG induction with or without ongoing steroids was a 12-month single-center study in 60 first or second kidney transplant recipients.32 In fact, what made this trial unique is that it compared steroid-free versus standard steroids as the single variation between the comparative arms. The rATG dose was 1mg/kg, for three to five doses, with a seven-day course of i.v. steroids. Patients received tacrolimus with MMF, with or without oral steroids. Graft function and rates of clinical rejection (13% versus 11% in controls) were unaffected by the absence of steroid therapy. Protocol biopsies were undertaken in 19 patients at month 12, and although subclinical rejection rates were similar in both arms, the increase in fibrosis at 6 and especially at 12 months was significantly greater in the steroid-avoidance group (p<0.001), a potential cause for concern although in most patients fibrosis was mild (grade 1). Assessment of subclinical changes by protocol biopsies may be an important focus in future studies of steroid avoidance.
Woodle et al. undertook a multicenter, randomized trial in which 151 living-donor kidney transplant patients were given either rATG (1.25–1.5mg/kg for four days) with steroids discontinued by day 6, or to no induction with standard i.v. and oral steroids until at least month 3 post-transplant.5 All patients were given tacrolimus and MMF, and dosing was similar in both treatment groups. By month 12, 72% of rATG-treated patients remained steroid-free, while in the control arm only 12% of patients managed to stop steroids. The 12-month incidence of BPAR was 13.9% versus 19.4% for the rATG/steroid-free group versus the control arm (n.s.) (Fig. 1). In terms of steroid-related adverse events, levels of total cholesterol was significantly lower in the steroid-free group at 12 months post-transplant, with a trend to less weight gain (p=0.07).5
, in moderate- or low-risk living donor kidney transplant patients randomized to rabbit antithymocyte globulin (rATG) with intravenous steroids only, or to no steroids with intravenous steroids and oral steroids for ≥3 months, both with tacrolimus (TAC) and mycophenolate mofetil (MMF) (Kaplan–Meier estimates). No statistical analysis was provided (observed rates of BPAR: 13.9% for rATG/TAC/MMF versus 19.4% for TAC/MMF/steroids; p=NS).")
Freedom from biopsy-proven acute rejection (BPAR), in moderate- or low-risk living donor kidney transplant patients randomized to rabbit antithymocyte globulin (rATG) with intravenous steroids only, or to no steroids with intravenous steroids and oral steroids for ≥3 months, both with tacrolimus (TAC) and mycophenolate mofetil (MMF) (Kaplan–Meier estimates). No statistical analysis was provided (observed rates of BPAR: 13.9% for rATG/TAC/MMF versus 19.4% for TAC/MMF/steroids; p=NS).
Other randomized trials have employed different rATG regimens with various maintenance protocols.33–35 Each of these has shown good graft and patient survival rates, with no indication of increased rejection when steroid avoidance is supported by rATG induction (Table 1).
Whether early steroid withdrawal after rATG induction could lead to an increased risk of donor-specific antibody (DSA) development was first studied by Delgado et al.41 in low-immunologic risk kidney transplant recipients. In this longitudinal study, performed in 37 patients randomized to early corticosteroid withdrawal at day 7 post-transplant (n=21 patients), or to maintenance steroid therapy (n=16) – with all patients receiving rATG induction – there was no difference between the two groups in terms of DSA development during five years’ follow-up. Interestingly, only one patient developed DSA (in the control group). This is fewer than would be expected, suggesting a protective role for rATG in DSA occurrence. Supportive data were recently published in a study by Brokhof et al.42 undertaken in a population of 114 consecutive moderately sensitized recipients who were divided into two groups based on induction immunosuppression (rATG versus basiliximab). At month 36 post-transplant, there was a lower incidence of de novo DSA and antibody-mediated rejection in the rATG group when compared with basiliximab. However, in this study standard maintenance steroids were given to all patients.
Alemtuzumab inductionSeveral randomized trials of steroid-free therapy have employed alemtuzumab induction, at a dose of 30mg given either once or twice (Table 1). Vathsala et al. performed a small, six-month study in which 30 patients were randomized to alemtuzumab with reduced-exposure CsA monotherapy and no oral steroids or to no induction with a conventional CsA-based regimen with steroids and azathioprine.36 Graft survival was 85% at month 6 in the alemtuzumab group versus 100% in the control arm, but larger studies of alemtuzumab with reduced-CNI,37 delayed CNI37 or tacrolimus monotherapy38,39 have not shown any deleterious effect on graft survival when alemtuzumab has been used to support steroid avoidance (Table 1). Consistently, the incidence of BPAR at 12 months post-transplant has been lower with alemtuzumab induction, a reduced-intensity maintenance regimen and a steroid-free protocol versus conventional regimens with36,37,40 or without38,39 steroids.
The largest trial in this series is the 3C study.40 A total of 852 patients were randomized to alemtuzumab (30mg peri-operatively and on the subsequent day) with low-exposure tacrolimus (5–7ng/mL) and reduced-dose MPA (enteric-coated mycophenolic acid 360mg b.i.d.), or to a conventional regimen of basiliximab induction, tacrolimus (5–12ng/mL), standard MPA dosing (540–720mg b.i.d.) with ongoing oral steroids. During the first six months post-transplant, the risk of BPAR was significantly lower in the alemtuzumab group versus controls (Fig. 2). The difference arose during the early weeks after transplantation and was accounted for by a reduced rate of T-cell mediated rejection (hazard ratio [HR] 0.37; 95% confidence interval [CI] 0.23–0.58; p<0.0001); antibody-mediated rejection was similar in both treatment arms (HR 1.59; 95% CI 0.52–4.86; p=0.41).40 Graft and patient survival rates at month 6 were similar between groups. Leukopenia was significantly more frequent under alemtuzumab, as would be expected, but there was no between-group difference in opportunistic infections or serious infections. Longer-term follow-up from this trial will be of interest, since at month 6 patients were randomized to remain on tacrolimus or switch to sirolimus. Reconstitution of the lymphocyte population after recovery from alemtuzumab-induced depletion may on one hand have profound effects on the risk of graft rejection, or on the other hand may give rise to more tolerogenic lymphocyte subsets. One recent retrospective study of 200 consecutive non-sensitized kidney transplant patients treated with rapid steroid taper reported that as well as higher rates of acute rejection, three-year graft survival was lower under alemtuzumab induction versus rATG.43
 in 852 unselected kidney transplant patents randomized to alemtuzumab induction with low-exposure tacrolimus, low-dose mycophenolic acid and no steroids, or to basiliximab induction with standard tacrolimus, standard mycophenolic acid and standard steroids. HR, hazard ratio; CI, confidence interval.")
Incidence of biopsy-proven acute rejection (BPAR) in 852 unselected kidney transplant patents randomized to alemtuzumab induction with low-exposure tacrolimus, low-dose mycophenolic acid and no steroids, or to basiliximab induction with standard tacrolimus, standard mycophenolic acid and standard steroids. HR, hazard ratio; CI, confidence interval.
No randomized trial of alemtuzumab with steroid avoidance after kidney transplantation has shown reduced patient survival when followed for up to two years,36–40 an important point in view of the severe lymphocyte depletion associated with alemtuzumab and the potential risk for infectious deaths or malignancy.
Comparative studies between induction agents within steroid-free regimensTwo registry analyses have specifically assessed outcomes according to type of induction in kidney transplant patients discharged on a steroid-free regimen.25,44 Sureshkumar et al. analyzed Organ Transplantation and Procurement Network (OPTN) data from 9172 patients who received a deceased-donor kidney transplant during 2000–2008, with a median follow-up of 26.8 months.25 The risk of graft failure after adjustment for a range of potentially confounding variables was found to be significantly higher with alemtuzumab or IL-2R antagonist induction compared to rATG (Fig. 3). Further analyses showed that higher graft survival for rATG versus alemtuzumab was maintained in at-risk populations (sensitized patients [panel reactive antibodies (PRA)>20%], expanded criteria donor recipients and cold ischemia time >24h)23 but significance was lost in these subpopulations for the comparison between rATG and IL-2R antagonists. Data on rejection were not reported, so it is unclear whether differences in graft failure were related to a lower propensity to rejection under rATG or other causes of graft loss. In a more recent cohort (2000–2012) of patients registered with OPTN, Tanriover et al. analyzed lower-risk living-donor recipients of a first transplant who were discharged on tacrolimus and MMF, with or without steroid therapy.44 Propensity scoring was used to address the risk of selection bias. Within the subpopulation that was discharged steroid-free (n=10,157), acute rejection at one year post-transplant was significantly lower with either rATG (odds ratio 0.73; 95% CI 0.59–0.90) or alemtuzumab (0.53; 0.42–0.67) versus IL-2R antagonist induction. The one-year risk of graft failure was higher with alemtuzumab versus IL-2R antagonist induction (odds ratio 1.27; 95% CI 1.03–1.56) but similar for rATG versus IL-2RA antagonists (1.19; 0.97–1.45).
 who were discharged on steroid-free immunosuppression. HR, hazard ratio; CI, confidence interval; rATG, rabbit antithymocyte globulin; IL-2R, interleukin-2 receptor.")
Probability of graft survival after adjustment for prespecified donor, recipient and transplant-related variables in deceased-donor kidney transplants performed during 2000–2008 registered with the Organ Procurement and Transplantation Network (OPTN) who were discharged on steroid-free immunosuppression. HR, hazard ratio; CI, confidence interval; rATG, rabbit antithymocyte globulin; IL-2R, interleukin-2 receptor.
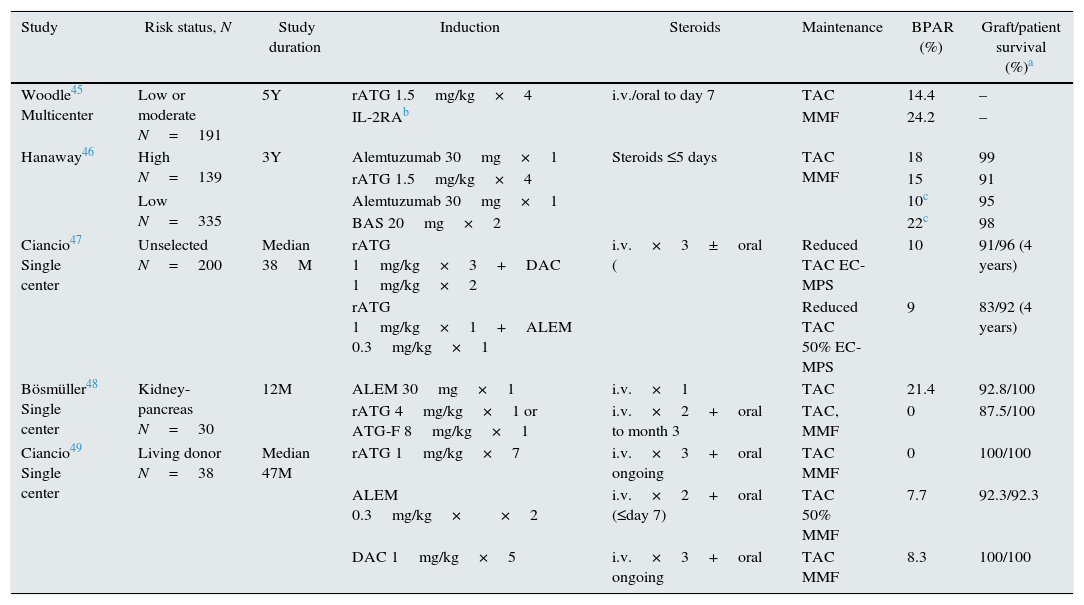
Randomized trials comparing steroid avoidance with different induction regimens are relatively rare (Table 2). In a double-blind, placebo-controlled trial of steroid cessation at seven days versus ongoing steroids, both with tacrolimus and MMF, the 191 patients in the steroid-withdrawal group received either rATG (n=125) or an IL-2R antagonist induction (n=66).46 In this subpopulation, the five-year incidence of BPAR was 14.4% versus 24.2%, respectively (p=0.09). Results of the ongoing SAILOR study, comparing rATG with steroid avoidance versus IL-2R antagonist induction with standard oral steroids in patients receiving low-dose tacrolimus and concentration-controlled MMF,50 will help to clarify the relative effectiveness of each class of agent in preventing rejection in the absence of steroids.
Randomized comparative trials of induction therapy with steroid avoidance in kidney transplantation.
| Study | Risk status, N | Study duration | Induction | Steroids | Maintenance | BPAR (%) | Graft/patient survival (%)a |
|---|---|---|---|---|---|---|---|
| Woodle45 Multicenter | Low or moderate N=191 | 5Y | rATG 1.5mg/kg×4 | i.v./oral to day 7 | TAC | 14.4 | – |
| IL-2RAb | MMF | 24.2 | – | ||||
| Hanaway46 | High N=139 | 3Y | Alemtuzumab 30mg×1 | Steroids ≤5 days | TAC MMF | 18 | 99 |
| rATG 1.5mg/kg×4 | 15 | 91 | |||||
| Low N=335 | Alemtuzumab 30mg×1 | 10c | 95 | ||||
| BAS 20mg×2 | 22c | 98 | |||||
| Ciancio47 Single center | Unselected N=200 | Median 38M | rATG 1mg/kg×3+DAC 1mg/kg×2 | i.v.×3±oral ( | Reduced TAC EC-MPS | 10 | 91/96 (4 years) |
| rATG 1mg/kg×1+ALEM 0.3mg/kg×1 | Reduced TAC 50% EC-MPS | 9 | 83/92 (4 years) | ||||
| Bösmüller48 Single center | Kidney-pancreas N=30 | 12M | ALEM 30mg×1 | i.v.×1 | TAC | 21.4 | 92.8/100 |
| rATG 4mg/kg×1 or ATG-F 8mg/kg×1 | i.v.×2+oral to month 3 | TAC, MMF | 0 | 87.5/100 | |||
| Ciancio49 Single center | Living donor N=38 | Median 47M | rATG 1mg/kg×7 | i.v.×3+oral ongoing | TAC MMF | 0 | 100/100 |
| ALEM 0.3mg/kg××2 | i.v.×2+oral (≤day 7) | TAC 50% MMF | 7.7 | 92.3/92.3 | |||
| DAC 1mg/kg×5 | i.v.×3+oral ongoing | TAC MMF | 8.3 | 100/100 |
ALEM, alemtuzumab; BAS, basiliximab; BPAR, biopsy-proven acute rejection; DAC, daclizumab; EC-MPS, enteric-coated mycophenolate sodium; IL-2RA, interleukin 2 receptor antagonist; i.v., intravenous; MMF, mycophenolate mofetil; rATG, rabbit antithymocyte globulin; TAC, tacrolimus.
In a large trial of kidney transplant patients stratified as either high or low immunological risk, Hanaway et al. randomized a 139 high-risk cohort to alemtuzumab or rATG, and 335 low-risk patients to alemtuzumab or basiliximab, all with tacrolimus and MMF; steroids were discontinued by day 5.46 In the high-risk group, there was no difference in the rate of BPAR between alemtuzumab and rATG at year 3 (Table 2). For low-risk patients, however, alemtuzumab induction was associated with a reduced rate of BPAR versus basiliximab (10% versus 22%, p<0.001). A further comparison of alemtuzumab versus rATG will be provided by the BEST study, an ongoing randomized, open-label trial in which patients receive belatacept-based immunosuppression with MPA and early steroid withdrawal, using induction with alemtuzumab in one group and rATG in a second group, or tacrolimus, MPA, early steroid withdrawal and rATG induction (NCT01729494).
Ciancio et al. undertook a randomized, single-center study of combined induction protocols in 200 first kidney transplant patients, whereby rATG was combined with either daclizumab or with a single dose of alemtuzumab47 (Table 2). All patients were given oral steroids to day 7, with maintenance therapy comprising tacrolimus and MPA. As might be expected with this relatively intensive regimen, rates of BPAR were low in both groups (10% and 9%), although graft survival was numerically higher in the rATG/daclizumab arm (91% versus 83%, n.s.). Early leukopenia was more frequent than with rATG/alemtuzumab induction, despite reduced MPA dosing, than with rATG/daclizumab (12% versus 31%, p=0.002).47 Other comparative studies of rATG versus alemtuzumab or an IL-2R antagonist using steroid-avoidance regimens have usually been relatively small (<40 patients), with different maintenance protocols and steroid use between treatment arms, limiting interpretation48,49 (Table 2). One notable point was a high rate of BPAR (21.4% at month 12) in a small series of kidney-pancreas patients randomized to alemtuzumab with tacrolimus monotherapy and no oral steroids,48 but confirmatory data are lacking.
Three randomized trials of alemtuzumab with steroid avoidance have used an IL-2R antagonist in the control arm, as discussed above, but since the maintenance regimen differed between groups the effect of the induction regimen cannot be assessed.38–40
Lymphocyte-depleting induction and steroid withdrawalSo far, head-to-head comparisons of steroid withdrawal with or without lymphocyte-depleting induction therapy have not been undertaken. Typically, studies of steroid withdrawal either before or after the first year post-transplant have not included induction therapy.4,9,10
One large study of late (month 3) steroid withdrawal allowed lymphocyte-depleting induction according to local practice. A third of patients (34% and 33% in the steroid-withdrawal and control groups, respectively) received induction, but this included both rATG and monomurab (OKT3).51 In this subgroup of 169 patients, the 12-month incidence of BPAR was 14% without steroids compared to 17% in the steroids group, i.e. steroid withdrawal was successfully achieved. In contrast, for the 331 patients without any induction therapy, BPAR was higher in the steroid-withdrawal patients (29% versus 15% in controls). Although only a subanalysis, these data suggest an advantage for lymphocyte depleting induction when undertaking steroid withdrawal after kidney transplantation.
In the SPIESSER study, 150 moderate-risk or low-risk kidney transplant patients underwent steroid withdrawal at the end of month 5 post-transplant.49 All patients received rATG induction.52 The intervention group was randomized to sirolimus and MMF in a CNI-free regimen, while the control group received CsA and MMF. In both arms, the 12-month incidence of BPAR was low (14% with sirolimus/MMF, 9% with CsA/MMF) and more than 80% of patients remained steroid-free at month 12. Steroid withdrawal around month 6 thus appears feasible under rATG induction with or without CNI therapy, when high-risk patients are excluded.
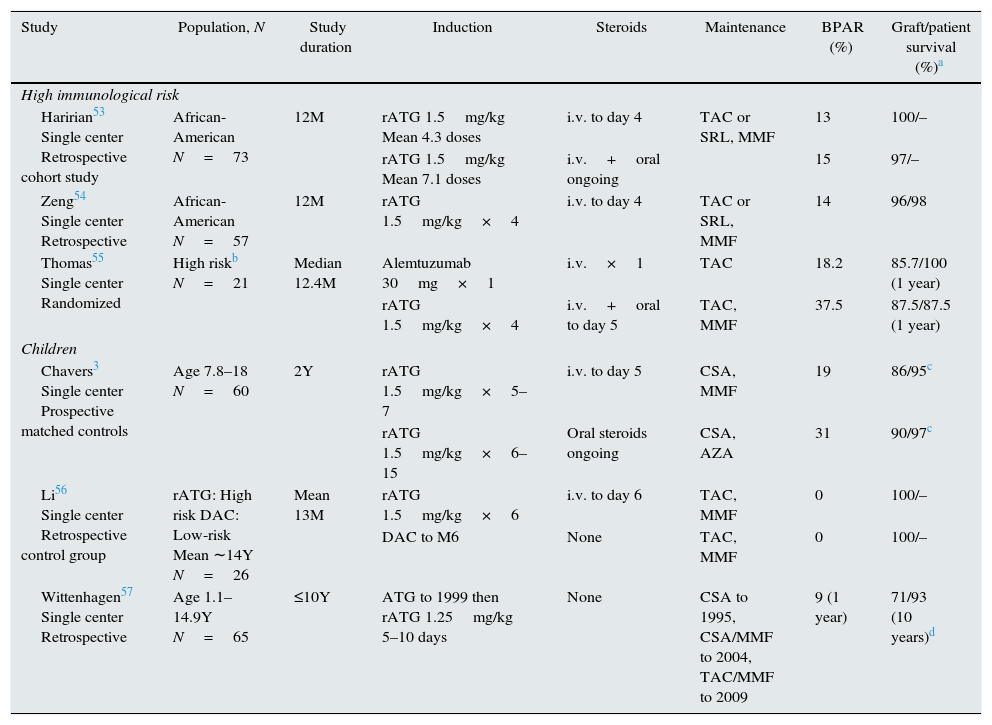
High-immunological risk patientsSteroid-free immunosuppression is less frequently attempted in high-risk patients, and data are limited (Table 3). Two retrospective single-center studies in African-American populations have assessed outcomes following rATG induction with i.v. steroids to day 4, both with a maintenance regimen of tacrolimus combined with either sirolimus or MMF.43,53 The one-year rates of BPAR in both series were acceptable for this high-risk group (13–14%), and graft and patient survival was excellent, but firm conclusions cannot be drawn in the absence of prospective trials. One small randomized trial (n=21) selectively recruited high-immunological risk patients (PRA >20% or repeat transplantation).55 The treatment regimens comprised alemtuzumab (a single dose of 30mg) with tacrolimus and no steroids, or rATG (total dose 6mg/kg) with tacrolimus, MMF, and steroids to day 5. In this small series, the rate of BPAR at a median of 12.4 months was 18.2% with alemtuzumab and 37.5% with rATG, while graft survival rates were 85.7% and 87.5%, respectively.55 These relatively high rates of rejection suggest that steroid avoidance may not be a favorable option in high-risk individuals unless there is a specific clinical imperative. None of these studies employed Luminex® technology to define the immunological risk pre-transplant, however, which makes any conclusion uncertain.
rATG or alemtuzumab induction with steroid avoidance in high-risk or pediatric kidney transplant populations.
| Study | Population, N | Study duration | Induction | Steroids | Maintenance | BPAR (%) | Graft/patient survival (%)a |
|---|---|---|---|---|---|---|---|
| High immunological risk | |||||||
| Haririan53 Single center Retrospective cohort study | African-American N=73 | 12M | rATG 1.5mg/kg Mean 4.3 doses | i.v. to day 4 | TAC or SRL, MMF | 13 | 100/– |
| rATG 1.5mg/kg Mean 7.1 doses | i.v.+oral ongoing | 15 | 97/– | ||||
| Zeng54 Single center Retrospective | African-American N=57 | 12M | rATG 1.5mg/kg×4 | i.v. to day 4 | TAC or SRL, MMF | 14 | 96/98 |
| Thomas55 Single center Randomized | High riskb N=21 | Median 12.4M | Alemtuzumab 30mg×1 | i.v.×1 | TAC | 18.2 | 85.7/100 (1 year) |
| rATG 1.5mg/kg×4 | i.v.+oral to day 5 | TAC, MMF | 37.5 | 87.5/87.5 (1 year) | |||
| Children | |||||||
| Chavers3 Single center Prospective matched controls | Age 7.8–18 N=60 | 2Y | rATG 1.5mg/kg×5–7 | i.v. to day 5 | CSA, MMF | 19 | 86/95c |
| rATG 1.5mg/kg×6–15 | Oral steroids ongoing | CSA, AZA | 31 | 90/97c | |||
| Li56 Single center Retrospective control group | rATG: High risk DAC: Low-risk Mean ∼14Y N=26 | Mean 13M | rATG 1.5mg/kg×6 | i.v. to day 6 | TAC, MMF | 0 | 100/– |
| DAC to M6 | None | TAC, MMF | 0 | 100/– | |||
| Wittenhagen57 Single center Retrospective | Age 1.1–14.9Y N=65 | ≤10Y | ATG to 1999 then rATG 1.25mg/kg 5–10 days | None | CSA to 1995, CSA/MMF to 2004, TAC/MMF to 2009 | 9 (1 year) | 71/93 (10 years)d |
AZA, azathioprine; BPAR, biopsy-proven acute rejection; CSA, cyclosporine; DAC, daclizumab; i.v., intravenous; MMF, mycophenolate mofetil; rATG, rabbit antithymocyte globulin; SRL, sirolimus; TAC, tacrolimus.
The advantages of steroid avoidance also have to be balanced against the risk of recurrence of certain glomerulopathies. In particular, several retrospective studies have shown that recurrence of IgA nephropathy is reduced in the presence of long-term steroid therapy. Among them, Clayton et al.58 analyzed data from the Australia and New Zealand Dialysis and Transplant Registry (ANZDATA) from 1521 adult recipients of a first kidney transplant in whom kidney failure was due to biopsy-proven IgA nephropathy. After adjustment for various confounding variables, steroid use was strongly associated with a reduced risk of IgA nephropathy recurrence (HR 0.50, 95% CI 0.30–0.84). Only 9% of patients in the study population received depleting induction therapy. Kukla et al. observed that steroid avoidance may be associated with a higher rate of recurrent glomerulopathy but found no apparent increase in the risk of graft loss in patients treated with rATG induction coupled with maintenance therapy comprising tacrolimus and an antimetabolite.59 Von Visger et al.60 recently showed similar results in a cohort of 124 patients, in which 91% of patients in the steroid-free group received lymphocyte-depleting induction. Although the mechanisms involved have not been elucidated, steroid avoidance would not appear advisable in kidney transplant patients in whom kidney failure was caused by IgA nephropathy.
In other types of glomerular diseases with risk of recurrence, such as focal segmental glomerulosclerosis, membranoproliferative glomerulonephritis or lupus nephritis, for which steroids are used as part of the treatment strategy in native kidneys, some centers tend to maintain steroids in the immunosuppressive protocol after transplantation even in the absence of relevant studies.
Steroid minimization in pediatric patientsSteroid-sparing strategies are of particular interest in children. Randomized trials of steroid avoidance in pediatric populations under lymphocyte-depleting induction have not, however, been carried out to date. In a single-center prospective study, Chavers et al. used rATG induction at a relatively high dose (1.5mg/kg for between five and seven doses) with i.v. steroids to day 5, with CsA and MMF as maintenance therapy3 (Table 3). The rate of BPAR (19% at two years) was acceptable and, importantly, children given the rATG/steroid-free regimen showed significantly improved growth compared to matched controls given oral steroid therapy (mean standard height deviation score −0.9 versus −1.9 in controls; p=0.003). Other steroid-related effects (body mass index, lipid profile, blood pressure) were unaffected although leukopenia was reduced (p=0.02) and there were fewer Epstein-Barr infections in the steroid-free arm (p=0.04).3 Li et al., in a single-center retrospective study, achieved a 0% rate of BPAR at a mean of 13 months post-transplant when a relatively high dose of rATG was employed (total dose 9mg/kg) with no oral steroids, tacrolimus and MMF, but growth data were not reported and there was no comparison versus a steroid-treated cohort. Lastly, a retrospective single-center study by Wittenhagen et al. has described a low rate of BPAR (9% at one year) in children given lymphocyte-depleting induction (primarily rATG) with different maintenance regimens.57 Use of depleting induction in a steroid-avoidance regimen using standard maintenance therapy seems adequate to prevent rejection in children following kidney transplantation, and merits a more rigorous examination.
Steroid- and CNI-avoidance regimensA small number of trials have investigated novel immunosuppressive regimens that avoid both steroids and CNI therapy.61–63 Ferguson and colleagues randomized 89 kidney transplant recipients at low or moderate immunological risk to one of three groups: the costimulation blocker belatacept with MMF, belatacept with sirolimus, or tacrolimus with MMF.62 All patients received rATG induction (total dose 6mg/kg) with i.v. steroids to day 4 post-transplant and no oral steroids. At one year, rates of BPAR were acceptable with belatacept and MMF (14%), but lower and similar in the belatacept/sirolimus group (4%) and the control arm (3%). More patients in the conventional tacrolimus/MMF group remained steroid-free at month 12, however (93% versus 73% or 77% in the belatacept group). So while promising, a CNI-free strategy may not be optimal for achieving steroid-free immunosuppression even with lymphocyte-depleting induction. Other small trials have also pointed to low or acceptable rates of BPAR when alemtuzumab induction is used to support CNI-free and steroid-free therapy,61,63 one of which achieved highly minimized immunosuppression by giving bone marrow infusions,63 but such regimens are not currently used in routine practice.
DiscussionThe literature contains few direct comparisons of steroid minimization regimens versus conventional steroid treatment in kidney transplant patients receiving lymphocyte-depleting induction. Studies are typically relatively small, with limited follow-up periods, and to date, the occurrence of de novo antibodies and antibody-mediated rejection is undocumented. Nevertheless, the available data show that the risk of acute rejection is low when rATG induction is given to support steroid-free regimens after kidney transplantation, at least for the first one to two years post-transplant. In the US, it is common practice to use rATG and stop steroids by day 7, and this appears to be a reasonable approach that does not increase the risk of rejection. In contrast, rejection may be more likely under IL-2R antagonist induction using a steroid-avoidance regimen. Induction with alemtuzumab appears effective in supporting steroid-free immunosuppression, although it is not licensed for use in solid organ transplant recipients. For patients at high immunological risk, the limited data available suggest that steroid minimization may not be advisable even with depleting induction therapy. The availability of single-antigen bead technology, permitting more precise measurement of anti-HLA antibodies, may enable more accurate identification of high-risk individuals and feasibly, expand the pool of patients considered candidates for steroid minimization.
In children, non-randomized studies indicate that depleting induction with standard maintenance therapy effectively prevents acute rejection with steroid avoidance, an encouraging finding given the growth inhibition associated with chronic steroid administration. More ambitious regimens have been attempted which include both steroid avoidance and CNI avoidance, of which depleting induction with maintenance therapy comprising belatacept and sirolimus appears the most promising, but currently can be regarded as an experimental approach.
There is some suggestion that steroid-associated side effects such as dyslipidemia and weight gain are lower with steroid-free immunosuppression, but this has not been shown to translate to an improvement in hard clinical endpoints. Given the lack of strong evidence in this field, no strong conclusions can be made.
Early steroid therapy with subsequent withdrawal (i.e. later than the first one or two weeks post-transplant) may be possible without additional risk of BPAR in patients who have received rATG induction, but while encouraging the data are too sparse for firm conclusions. Where late steroid withdrawal is attempted (months 3 to 6 post-transplant), it seems preferable to employ tacrolimus-based immunosuppression over CsA. Overall, the effectiveness of steroid avoidance regimens in this setting is better documented than subsequent withdrawal strategies.
In summary, there is a suggestion that steroid avoidance is beneficial for patients after renal transplantation, with the potential to avoid or reduce steroid-related comorbidities. Whilst the limited literature seems to indicate that depleting induction therapy could be the treatment of choice for steroid minimization and avoidance in kidney transplantation, the results of prospective randomized, controlled studies are eagerly awaited.50
Authors’ contributionAll authors actively contributed to the content of the manuscript during discussions, critically reviewed draft material, and approved the final manuscript for submission.
FundingThe authors attended a meeting at which the data for inclusion in the paper were discussed and presentations made by the authors. The meeting was coordinated by Sanofi but the authors received no remuneration or funding for travel expenses. Julio Pascual and Marta Crespo are supported by grants FISPI13/00598 and RedinrenRD12/0021/0024.
Conflicts of interestMaarten Naesens has received travel support, research grant or consultancy fees from Sanofi, Novartis, Astellas and Roche. Stefan Berger has received travel support from Astellas and consultancy fees form Sanofi, Novartis and Astellas. Luigi Biancone has received travel support, research grant or consultancy fees from Sanofi, Novartis, and Astellas. Marta Crespo has received public funding for research from the Spanish Ministry of Health and travel support, research grant, consultancy fees or speaker's honoraria from Novartis, Astellas, Sanofi and Abbvie. Arjang Djamali is a consultant to Sanofi and has received grants from BMS and Takeda. Alexandre Hertig has received consultancy fees from Sanofi, Bristol-Myers-Squibb, travel grants from Novartis and CSL Behring, and research grant from Astellas and CSL Behring. Robert Öllinger has no conflicts of interest to declare. José Portolés has received travel support, research grant or consultancy fees from Sanofi, Novartis, and Astellas. Andreas Zuckermann has received research grants from Astellas, Roche, Novartis and Sanofi, is a member of the speakers’ bureau for Novartis and Sanofi, and is a member of advisory boards for Sanofi and Sandoz. Julio Pascual has received travel support, research grant or consultancy fees from Sanofi, Novartis and Astellas.



