




There is currently no doubt that a kidney transplant with good function is the best treatment we can offer a child with severe kidney failure, improving their growth, development and life in general. But there are few works that follow these patients over the years to find out what their life is like as adults, their achievements and if there are any difficulties that may have arisen from their illness. That has been the objective of this work.
Material and methodsWe have collected the evolution of 287 patients who received at least one kidney transplant in pediatric age, analyzing not only the survival of grafts and recipients but, fundamentally, their current quality of life.
ResultsOver a 40-year period (1979−2019), 345 kidney transplants were performed in 287 pediatric recipients, with a rate of retransplantation before reaching the age of majority of 16.7%. Survival, both of patients and grafts, has improved remarkably in the last 20 years. The survival of transplanted patients in the period from 1979 to 1996 at 10, 20 and 25 years after the intervention was 83%, 76% and 65% respectively, and 94% and 82% at 10 and 20 years respectively in those transplanted in the period from 1997 to 2019. Graft survival in the period from 1979 to 1996 at 10 and 20 years was 39% and 18%, increasing in the second period to 68% and 34% respectively. Survival of the first living donor graft (LD) at 5 and 10 years was 94% and 89%. Currently 150 of these patients are adults. Of these, 32% have a stable partner and 6.6% have children. The level of training is lower than that of the general population and many of them have other comorbidities.
ConclusionsThe life expectancy of pediatric patients with kidney failure transplanted during childhood has improved markedly in recent decades, as has graft survival, being better with a living donor. In general, they consider themselves satisfied with their lives, with great acceptance of their illness and limitations, but -analyzing their testimonies- we conclude that they lack social support, both for themselves and their families, to achieve a higher level of education and better quality of life.
Actualmente no hay duda de que un trasplante renal con buena función es el mejor tratamiento que podemos ofrecer a un niño con insuficiencia renal severa, mejorando su crecimiento, desarrollo y actividad en general. Pero hay pocos trabajos que sigan a estos pacientes a lo largo de los años para conocer cómo es su vida de adultos, sus logros y si hay dificultades que han podido derivarse de su enfermedad. Ese ha sido el objetivo de este trabajo.
Material y métodosHemos recogido la evolución de 287 pacientes que recibieron al menos un trasplante renal en edad pediátrica en nuestra unidad, analizando no solo la supervivencia de los injertos y receptores sino, fundamentalmente, su calidad de vida actual.
ResultadosEn un periodo de 40 años (1979−2019) se realizaron 345 trasplantes renales en 287 receptores pediátricos, con una tasa de retrasplantes antes de cumplir la mayoría de edad del 16,7%. La supervivencia, tanto de los pacientes como de los injertos, ha mejorado notablemente en los últimos 20 años. La supervivencia de los pacientes trasplantados en el periodo de 1979 a 1996 a los 10, 20 y 25 años de la intervención fue del 83%, 76% y 65% respectivamente, y del 94% y 82% a los 10 y 20 años respectivamente en los trasplantados en el periodo de 1997 a 2019. La supervivencia del injerto en el periodo de 1979 a 1996 a los 10 y 20 años fue del 39% y 18%, aumentando en el segundo periodo al 68% y 34% respectivamente. La supervivencia del primer injerto con donante vivo (DV) a los 5 y 10 años fue del 94% y 89%.
Actualmente son adultos 150 de estos pacientes. De ellos, 32% tienen pareja estable y 6,6% tienen hijos. El nivel de formación es menor que el de la población general y muchos de ellos tienen otras comorbilidades.
ConclusionesLa esperanza de vida de los pacientes pediátricos con insuficiencia renal trasplantados durante la infancia ha mejorado notablemente en las últimas décadas, así como la supervivencia de los injertos, siendo mejor con donante vivo. En general, ellos se consideran satisfechos con su vida, con gran aceptación de su enfermedad y limitaciones, pero -analizando sus testimonios- concluimos que les falta apoyo social, tanto a ellos como a sus familias, para lograr un nivel educativo más alto y mejor calidad de vida.
There is currently no doubt that kidney transplantation is the best treatment we can offer to a child with chronic kidney failure. A transplant, with a good graft function, allows healthcare workers to correct to a large extent the metabolic alterations secondary to the disease, correct anemia, improve appetite and, with it, nutritional status, improve activity, growth, social relationships… in short, improve the child's quality of life. All this necessarily entails lifelong immunosuppressive treatment, with periodic medical checks.
But the life expectancy of a child is long, longer than the expected survival time of the graft, so the individual will need several grafts over their lifetime, with periods of organ malfunction that will require returning to multiple treatments in addition to the usual treatment with immunosuppressants, more frequent visits and medical checks and, most likely, new periods of treatment by dialysis. That is, with a kidney transplant we do not “cure” a pediatric patient with kidney failure.
What happens to these patients next, when we transfer them to adult units upon reaching the age of adulthood? What is their life expectancy? What problems have they encountered throughout their lives? Do they achieve an “acceptable” quality of life?
There are few studies on these issues, probably because it is difficult to conduct multiple follow-ups across different units, different hospitals, and different cities over many years.
Currently, the great development of computer science and communication has facilitated long-term monitoring of this population, allowing us to better understand the lives of these children and adults, and thus, perhaps, we can consider new challenges to improve their quality of life.
With this idea, 40 years since the beginning of the kidney transplant program in the pediatric unit of the hospital where we work, we have tried to synthesize the lives of our patients, reflecting, more than their clinical-analytical data, their development and their achievements, in order to know what we are offering when we transplant these patients and what we can do to improve their futures.
Materials and methodsRetrospectively, through medical records - initially on paper, later in computer databases- and prospectively, through outpatient medical visits, through emails or postal mail and telephone calls, we have monitored the 345 pediatric kidney transplants conducted by the Pediatric Nephrology unit of the Virgen del Rocío University Hospitals, in Seville. The study covered a period of time of 40 years since the beginning of the transplant program in our unit. Patients were transferred to the adult units closest to their places of residence at the age of 18.
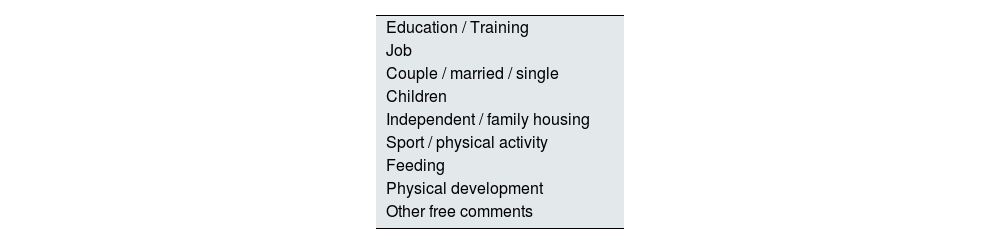
Through the medical records we have collected the deaths and the current clinical situation of the patients to study the survival of both the graft and the patient. Through conversations with them, emails and phone calls, we have asked them, including those of adult age and transferred to adult services, the questions that are included in Table 1 to learn some aspects of their quality of life over time, which was what most interested us, also encouraging them to tell us what they wanted about themselves and if they were satisfied.
We defined comorbidity as the involvement of at least one organ other than the kidney.
The first pediatric kidney transplant in our hospital was performed on June 1, 1979, and we have collected in this work all transplants performed since then until June 1, 2019, 40 years later, with a minimum follow-up time of one year in all patients.
Graft and recipient survival data have been analyzed with the IBM SPSS Statistics 20.0 statistical program, estimating patient and graft survival using the Kaplan-Meier method. We consider patient survival the period elapsed from the first graft until death, regardless of whether they have been transplanted on more than one occasion, since what we want to highlight fundamentally in this work is the future change in quality of life of these patients, from when their kidney function declines to the point of requiring a transplant, currently considered the ideal treatment. The survival of the grafts, measured from the time of transplantation until restarting dialysis or needing a new graft, is calculated from the total of those implanted in each period without taking into account whether it was the first or a retransplant.
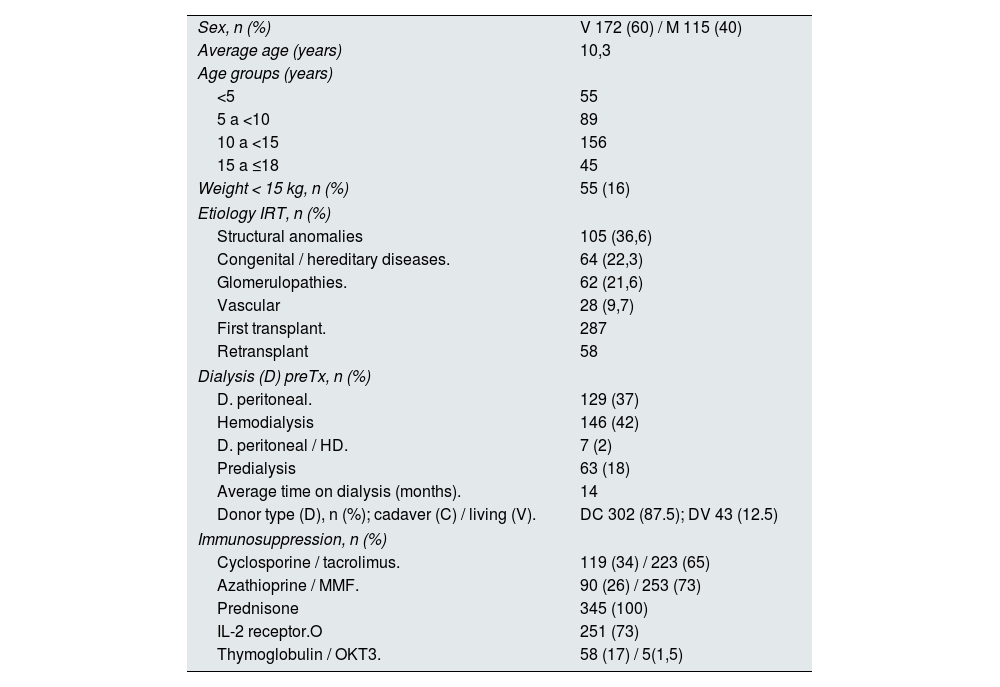
ResultsIn these 40 years of activity in child kidney transplantation, 345 transplants were performed in 287 patients under 18 years of age, with ages ranging from 1.5 years in the case of the youngest patient to 17.8 years for the oldest. The smallest weighed 8.9 kg. The main characteristics of the population studied are shown in Table 2.
Patient characteristics (n = 287).
| Sex, n (%) | V 172 (60) / M 115 (40) |
| Average age (years) | 10,3 |
| Age groups (years) | |
| <5 | 55 |
| 5 a <10 | 89 |
| 10 a <15 | 156 |
| 15 a ≤18 | 45 |
| Weight < 15 kg, n (%) | 55 (16) |
| Etiology IRT, n (%) | |
| Structural anomalies | 105 (36,6) |
| Congenital / hereditary diseases. | 64 (22,3) |
| Glomerulopathies. | 62 (21,6) |
| Vascular | 28 (9,7) |
| First transplant. | 287 |
| Retransplant | 58 |
| Dialysis (D) preTx, n (%) | |
| D. peritoneal. | 129 (37) |
| Hemodialysis | 146 (42) |
| D. peritoneal / HD. | 7 (2) |
| Predialysis | 63 (18) |
| Average time on dialysis (months). | 14 |
| Donor type (D), n (%); cadaver (C) / living (V). | DC 302 (87.5); DV 43 (12.5) |
| Immunosuppression, n (%) | |
| Cyclosporine / tacrolimus. | 119 (34) / 223 (65) |
| Azathioprine / MMF. | 90 (26) / 253 (73) |
| Prednisone | 345 (100) |
| IL-2 receptor.O | 251 (73) |
| Thymoglobulin / OKT3. | 58 (17) / 5(1,5) |
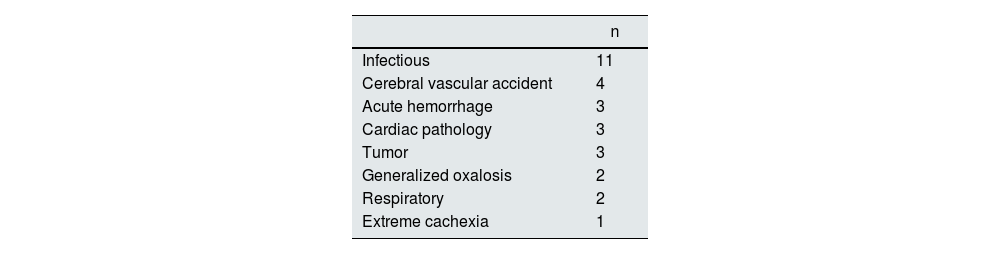
Today we have lost track of 17 of these 287 patients, so we do not know their current situation. But we do know that of the remaining 270, 45 have died, that is, the mortality rate has been 16.66% of patients in these 40 years. The youngest died at the age of 1.5 years, and the oldest is 37.5 years old. The median age at death was 19 years, with a median time since the first transplant of 9 years (range from 48 hours to 25 years). Nine of these 45 patients had already received a second graft, 3 of them after being transferred to adult services. Fifteen died with a functioning graft, and the remaining 30 were back on dialysis due to graft failure.
The causes of death, of which we know 29, are listed in Table 3; we highlight that the leading cause is infection.
We analyzed the survival of grafts and recipients by differentiating two groups: those who received grafts between 1979 and 1996 inclusive, and those who received them from 1997 to 2019. The first group (93 grafts, 77 patients) received as immunosuppressive treatment cyclosporine (with controls of plasma levels with much variability), azathioprine and prednisone; the second group (252 grafts, 210 patients) received treatment with calcineurins inhibitors (29 with cyclosporine with better controlled levels, the remaining 223 with tacrolimus), mycophenolate mofetil, and prednisone. Survival, both of the grafts and of the patients, has improved markedly in the second period, as can be seen in Figs. 1 and 2. Patients transplanted in the period from 1979 to 1996 had a survival of 83%, 76% and 65%, respectively, at 10, 20, and 25 years after the intervention. Survival of transplants in the period 1997–2019 was 94% and 82%, respectively, at 10 and 20 years (P < .01).


Graft survival in the period from 1979 to 1996 at 10 and 20 years of follow-up was 39% and 18%, respectively, improving in the second period to 68% at 10 years and 34% at 20 years. The median estimated in the first period was 7.36 years, compared to 15.156 years in the second period (P < .0001).
Living donor transplants began in our unit in 2005, achieving a total of 43 transplants in 2019. Survival of these grafts, all early transplants, was 89% at 10 years.
Despite this, 48 (16,7%) of the 287 patients had received a second graft before reaching the age of 18 years, 8 of these 48 had been transplanted for the third time and two of these 8 had already received a fourth transplant before reaching adulthood, thus before being transferred to adult nephrology services.
During the follow-up time in adult services 40 more patients received a second kidney transplant, 14 a third and 2 a fourth and, subsequently, one patient received a fifth graft.
Today, the oldest of these patients would now be 54 years old. The average age of the 225 patients that we know and are currently alive is 21.2 years, ranging from 4 years old to 50 years.
As of June 1, 2020, 150 patients were already adults (>18 years) and 114 of them were ≥25 years of age, excluding the deceased and those lost to follow-up. On the other hand, 75 patients had not yet reached the age of 18. One hundred and eighty-two had a working graft (81%), with the remaining 43 (19%) undergoing chronic dialysis treatment.
Eighty two out of the 150 adult patients responded to our survey.
Of these, 31 (38%) are married or with a stable partner, only 10 have children (two have two children, the rest one); 32 of them (39%) are living independently from their families, with or without a partner. Some (16%) highlighted their short stature (well below that expected by family inheritance: << P3), and 4 of them mentioned their obesity.
In terms of education, only 13 (16%) have higher education and 23 (28%) have a secondary or vocational education. The rest (56%) had studied, at most, until the first stage of secondary education. A 35% (n = 29) have a job.
Twenty-six percent said that they were happy/satisfied with their quality of life; in their opinion, their lives are similar to those of their friends without chronic disease. Only three reported notable limitations in their lives, although at least 30% of them have other comorbidities or pathologies associated with their kidneys, particularly liver pathologies (10 patients, of which 4 have subsequently undergone liver transplants), malignancies (13), severe bone disorders (8 patients, 4 of them with hip and/or knee prostheses), diabetes (5), mental disorders (3), deafness (3), cataracts (2), and organic involvement secondary to severe arterial hypertension (2).
Only 9% exercised regularly, and 5 of the 82 respondents (6%) reported drug addictions.
With the exception of two patients, all reported that they were happy to learn that we were interested in their lives, their achievements and their expectations, and wanted to share their stories and their difficulties.
All but one claimed to have good memories of their time in the Pediatric Nephrology unit despite multiple admissions, analytical extractions, treatments, and tests. We include a sample of short selections from their answers at the end of this work.
DiscussionIn our patients, as in other pediatric samples,1 the most frequent etiology that leads a child to require a kidney transplant is congenital structural abnormalities of the urinary system, followed by hereditary diseases.
Life expectancy is the average number of years that a person of a certain age would expect to continue living if the currently observed pattern of mortality by age (mortality rates by age) were maintained. In Spain, between 1999 and 2019 the life expectancy at birth of men has gone from 75.4 to 80.9 years and that of women from 82.3 to 86.2 years, according to the basic demographic indicators published by Spain’s National Institute of Statistics (June 2020).2
Given the age at transplantation of all the patients collected in this work under 18 years, their average post-transplant life expectancy, according to the European registry, would be 63 years, as shown in Fig. 3,3 or according to the life expectancy of the general population by age groups, in Spain, as shown in Table 4 (somewhat lower in the years we transplanted our first patients). It is still too early to know how many of our patients will reach those ages, given that the oldest at the time of this study could not have been older than 54 years at the time.

Life expectancy at different ages by period. Gender gap. Spain.
| 2019 | 2009 | |||||
|---|---|---|---|---|---|---|
| Men | Women | Gender gap (women-men) | Men | Women | Gender gap (women-men) | |
| At birth | 80.9 | 86.2 | 5.4 | 78.6 | 84.7 | 6.0 |
| 10 years | 71.2 | 76.5 | 5.3 | 69.0 | 75.0 | 6.0 |
| 20 years | 61.3 | 66.6 | 5.3 | 59.1 | 65.1 | 5.9 |
Units: years.
Source: Mortality tables, INE.2 Available at: https://www.ine.es/jaxi/Datos.htm?path=/t00/mujeres_hombres/tablas_1/l0/&file=d01005.px.
Considering that the mortality rate for the Spanish population in 1996 was 8.75 per thousand inhabitants, it was similar in 2019: 8.83 per thousand inhabitants. In our autonomous community, Andalusia, the mortality rate for the total population in 1996 was somewhat lower, at 8.18 per thousand, remaining at 2019 at 8.35 per thousand. If we examine mortality in Andalusia in the same years for the age group between 1 and 39 years, in 1996 it was 5.76 per thousand inhabitants, having decreased in 2019 to 2.09 per thousand. It is difficult to compare this mortality rate with that obtained in our patients, given the different ages and annual variations, but the average rate obtained roughly over these years, is 4.16 annual deaths per thousand. Although as seen in the survival graphs, both the grafts and the patients have improved survival in the last 20 years, with a higher mortality rate in the period from 1979 to 1996 for the same post-transplant time period (Fig. 1).
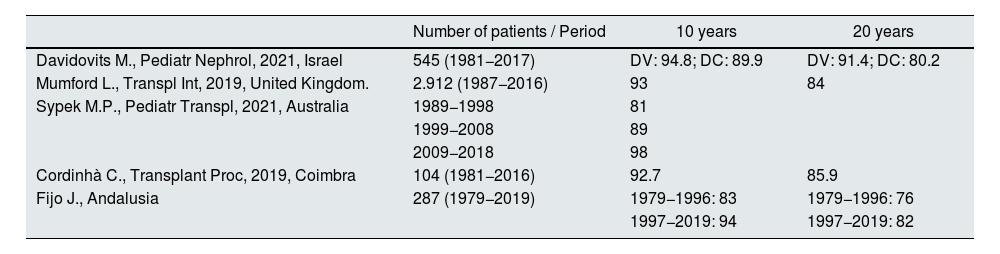
This patient survival is similar to those obtained in other pediatric patient samples in the literature4–6 (Table 5) in the same time period.
Patient survival (%).
| Number of patients / Period | 10 years | 20 years | |
|---|---|---|---|
| Davidovits M., Pediatr Nephrol, 2021, Israel | 545 (1981−2017) | DV: 94.8; DC: 89.9 | DV: 91.4; DC: 80.2 |
| Mumford L., Transpl Int, 2019, United Kingdom. | 2.912 (1987−2016) | 93 | 84 |
| Sypek M.P., Pediatr Transpl, 2021, Australia | 1989−1998 | 81 | |
| 1999−2008 | 89 | ||
| 2009−2018 | 98 | ||
| Cordinhà C., Transplant Proc, 2019, Coimbra | 104 (1981−2016) | 92.7 | 85.9 |
| Fijo J., Andalusia | 287 (1979−2019) | 1979−1996: 83 | 1979−1996: 76 |
| 1997−2019: 94 | 1997−2019: 82 |
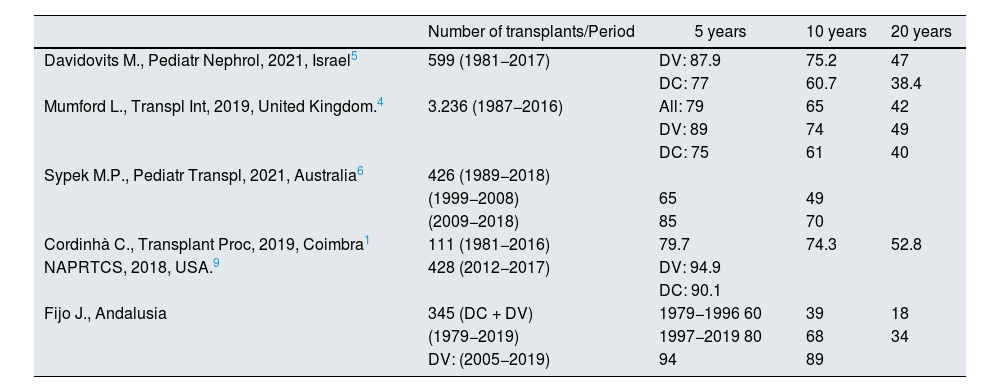
To compare the survival of the grafts with those obtained in other samples4–7 (Table 6) it must be considered that those collected by other authors are calculated only for first grafts, whose overall survival is often higher than in retransplants.8,9 We have not made that distinction, so the average survival of the grafts calculated in this work may be lower due to retransplantation.
Graft survival (%).
| Number of transplants/Period | 5 years | 10 years | 20 years | |
|---|---|---|---|---|
| Davidovits M., Pediatr Nephrol, 2021, Israel5 | 599 (1981−2017) | DV: 87.9 | 75.2 | 47 |
| DC: 77 | 60.7 | 38.4 | ||
| Mumford L., Transpl Int, 2019, United Kingdom.4 | 3.236 (1987−2016) | All: 79 | 65 | 42 |
| DV: 89 | 74 | 49 | ||
| DC: 75 | 61 | 40 | ||
| Sypek M.P., Pediatr Transpl, 2021, Australia6 | 426 (1989−2018) | |||
| (1999−2008) | 65 | 49 | ||
| (2009−2018) | 85 | 70 | ||
| Cordinhà C., Transplant Proc, 2019, Coimbra1 | 111 (1981−2016) | 79.7 | 74.3 | 52.8 |
| NAPRTCS, 2018, USA.9 | 428 (2012−2017) | DV: 94.9 | ||
| DC: 90.1 | ||||
| Fijo J., Andalusia | 345 (DC + DV) | 1979−1996 60 | 39 | 18 |
| (1979−2019) | 1997−2019 80 | 68 | 34 | |
| DV: (2005−2019) | 94 | 89 |
Of course, we also note that although there has been less follow-up time since the start of living donor transplants in our unit in 2005, and fewer transplants performed, living donor transplants appear to have better survival compared to that of cadaveric donor transplantation, as reported in other pediatric samples.
It is worth noting the number of patients with onset of kidney failure at an early age who have already received more than one graft when reaching adulthood, which means that many of these patients are sensitized with a high percentage of antibodies. This - coupled with the loss of preference in the waiting lists when they reach adulthood- makes a new transplant more difficult and forces them to remain in dialysis for a long time during early adulthood, with disruptive impacts on their lives, as we see in some of the patient comments.
The educational level of the adult population10 (aged 25–64) is an indicator related to the development and employment levels of current and future society.
In Spain, in the year 2019, 41.7% of men and 35.7% of women (aged 25–64) had a 0–2 level of education corresponding to preschool, primary and first stage of secondary education, with the percentages of the population being lower at higher educational levels.
By age group, in the population aged 25–34, 40.6% of men and 52.4% of women have a level of training corresponding to higher education and doctorate (levels 5–8). For the same age group, the percentages with a level of training lower than the second stage of secondary education, that is, level 0–2, are 35.5% in men and 24.8% in women.
Only 16% of patients in this series have higher education (level 5–8) and 28% have intermediate or vocational training (level 3–4); the remaining 56% have training equivalent to levels 0–2. Some 42% dropped out of school early. There were no significant differences in the level of education in relation to sex. This differs with some of the few studies that collect this data in the literature, such as Mekahli et al.11 and Rosenkranz et al.,12 which find a high percentage of patients with complete studies and professional studies although with a lower employment rate than the general population, although they are limited to a small group of patients chosen to participate in another study.
In the year 2020, in Spain, school dropouts, despite having been reduced compared to previous years, reached 20.2% for men and 11.6% for women, figures much lower than those of our study. These figures must influence the low number of patients who work and the associated difficulty in achieving independence.
The 75 pediatric patients still being monitored in our Pediatric Nephrology unit, are attending school except for one (illiterate), and although some of them are in lower grades than they would correspond to their ages, they have higher educational levels than recorded in the older patients.
We did not obtain survey answers from 68 adult patients, so our data may have some bias depending on the current situation of patients who have not participated or the memories they had of their passage through child nephrology. However, we do have their early medical characteristics (age at first transplant, etiology of their kidney failure, current clinical data…), and found no significant differences in these elements between non-respondents and respondents.
There is no universal concept of quality of life, nor a single instrument to measure it. It depends, to a large extent, on the scale of values of the person and the emotional and personal resources of each one. We started this work with the intention of knowing what our patients' perception of their lives was, if after transplantation at pediatric ages - in their opinion - they achieved a life similar to that of the general population. We wanted to know the personal situation of each patient, their way of life, their social skills, their psychological development, what they wanted to tell us. That is why we used directed but open-ended questions. We have attempted to conduct fundamentally qualitative research.13 Perhaps if we had used some of the existing questionnaires (WHOQOL-100 or BREF, SEIQoL-DW… or other more specific ones, such as the Kidney Disease Quality of Life [KDQOL], used by other authors14) it would have been easier to communicate and compare our results. Thus, it has been a very difficult task to summarize and draw conclusions with statistical support, but we consider it worthwhile to know what life is like after a first kidney transplant performed in childhood.
What emerges from their answers and testimonies,15 some of which we collect in this article, is that, although many of them have been, not only been able to adapt to transplantation, but to achieve psychological and emotional growth to have a satisfactory life similar to healthy individuals or even with more motivation and energy, they are still chronically ill, several of them with behavioral problems, difficulties with attention and learning and episodes of anxiety and depression. This coincides with the conclusions reported in other publications.16
Both, patients and their families need support, especially the latter, given the impact of caring for these patients, at least until they became adults, in their own timeframe, their family dynamics, their level of stress, and their quality of life.
As has already been fully demonstrated, kidney transplant is the best option for these patients, and a functioning transplant allows them to resume their rhythm and quality of life, increasing their survival and improving their growth and development. But as has already been reflected in other works,16,17 there is a social perception that kidney transplant in these patients represents a total cure for their kidney failure, enabling them to resume a life without limitations; this is not so: it is the best treatment we can offer them, but the quality of life they achieve in the long term and the rehabilitation of many of them is still insufficient.
ConclusionsKidney transplant patients are chronically ill.
Even with the enormous improvement in the survival of pediatric kidney transplant patients during childhood and their grafts, and the good adaptation of some of them to their disease, many others have serious difficulties in achieving good social development and independence. More funds and social support are needed to ensure that they have greater support from therapeutic teams -both themselves and their families- that include pedagogical counselors, psychologists, and social workers.
Testimonials• I have received your letter, it gave me great joy. I'm already 45 years old. I started my illness at the age of 11. My first transplant lasted 11 and a half years. Five years after the intervention I had a rejection, but the kidney lasted 6 and a half more years. I went back on dialysis during 1 year and 4 months, and I was transplanted again 18 years ago, and everything was perfect thanks to my donor. I got married, I did not have children, I completed basic school and courses in sewing and hairdressing. I live with my mother and my husband. The truth is, I don't do much sport because I wear hip prostheses, and previously I had another on my femur. I don't have any food problems. Although my family is short, I am the shortest and I am self-conscious about my body; my illness has influenced me a lot. My life has been difficult.
When this confinement thing ends, I'll go to the hospital. I want to visit my doctors and nurses from my childhood. A million thanks for sending me this letter, it has made me super happy today.
• What a joy to receive these types of letters. Of course I remember all of you. I hope you are all doing very well, and now more so, with everything we are experiencing.
I'm great, in November I'll have been transplanted for 13 years. I have myomas in the uterus, but it is something that does not worry me at the moment, and with the checkups they always have me under control. At the end of 2018 I was very ill, with a Clostridium infection, what a cursed time… there were bad months, my lab values were out of control with the bacteria until the end of 2019, but I’m here, still in the fight, and still have a way to go. I think that my very positive character makes me take things differently.
In December of last year I finished studying dental prosthesis, and I continue training and studying; in 2010 I became a pharmacy technician, but I am still looking for work, things are very tough. I still live with my parents.
I am happy, I live a life totally like a healthy person with two kidneys, and I even think that I am even doing better than some other people, I take a lot of care of myself. I do a lot of sport, because I feel very good about myself, and my partner, apart from his work, is dedicated to fitness, and you can imagine. With food I take good care of myself and I don't usually go overboard. Whenever I go to check-ups, people ask me if I am the transplant recipient, because nothing is noticeable to me, and it is true that other patients do not have the quality of life that I have due to many factors.
My physical development is not something I've ever worried about; I'm short but, hey, nothing that a pair of good heels can’t fix.
And that’s all, I encourage the little ones you have there or the teenagers to try to live a happy and “normal” life within their possibilities, encourage them to study and train. Things are bad, but anything could happen in this life and change you overnight. Above all, as I said before, be very positive.
Please keep in touch. A very big hug for the whole team and thank you always.
•… I am currently well, thank God and my kidney is working perfectly. I walk for an hour every day. I stopped studying, I didn't finish the intermediate grades (ESO), and now I'm studying to try to finish it. I also work on whatever comes up.
My transition to the adult hospital was very good, although it took me a while to adapt to the change.
Personally, I live with my partner in his home and town; he takes very good care of me. At the moment, we have no children.
As soon as things get better, I'll stop by to say hello, as that hospital was my home for many years. Virtual kisses.
•… I am the mother of …, I am writing these lines to tell you that he is fine, very tired of being on dialysis again, but it seems that that is what we have to face. He has many antibodies and they cannot find a kidney for him.
His life is not too good, because he has been on dialysis for 13 years, so he does not work, he lives with us, now he exercises a lot, he is in the gym and he goes for walks. He had a friend, but she was on dialysis like him and one day she passed away. His studies are just as bad, he has not even obtained his driver's license. As far as diet, he eats now more or less what he used to eat.
Now they say that he has it very difficult and we don't know what to do, he comes super tired, with the spirit that characterizes him, and I see him some days and I don't know what to think.
You don't know how grateful I am for your letter…
• … In December, 32 years ago, I had a kidney transplant and I'm still fine. I didn't get to study anything serious, I work as a housewife. I spent a few years working in a hotel. I got married 21 years ago, and I have a 15-year-old son; it was a great pregnancy, and then I had a couple of miscarriages. I live at home with my husband and son, within my limitations I live happily, and my life does not change much from that of others. My physical development has been normal, although it caught me in full growth development. I don't do any sports, although I walk. My diet is normal, I eat everything, yes, with low amounts of salt; I have high blood pressure due to the narrowing of the kidney vein that was transplanted to me, so I have had several dilations; in the last one they put in a coil.
• … I have been transplanted for 26 years. I suffered a lot of bullying because of my appearance both by classmates and teachers, I never wanted to go to school or high school because of that. I could not finish my studies, and in my adult life I still carry those mental problems from my childhood. I only got to third-year of ESO. So my studies are basic. I took a course to be a kindergarten and playroom assistant (because I love children). I took three months of practical training and I spent the whole time from virus to virus, and I had to leave it.
I took a makeup course and I'm currently doing that for a living.
I have had a stable partner for 10 years; I do not have children, but I would love it, it would be a dream for me.
I live with my parents, but I spend several days with my partner.
•… When my son, after the transplant and his recovery at home, returned to his elementary studies, it was not as we would have liked it as parents, and it is not because he suffered some kind of rejection or misunderstanding from his classmates, at all, it was because he felt bad because his classmates had moved on and he looked a lot “older” with the new classmates. So we went through a bad times that ended with dropping out of school.
It was a stage of adaptation for everyone to the new situation, for him and for us, wanting to do the best for him and not knowing what was best.
• I tell you about my experience in the children's unit of the Virgen del Rocío: until I reached adolescence I did not realize my situation, although as a child they always explained everything to me very well and I did not have any “trauma”; on the contrary, whenever I remember something they are good memories, but I think that the boys and girls who are entering adolescence should have a psychologist, and with the new technologies so many trips and visits to the hospital should be avoided.
Regarding my studies, I had some problems in school but I managed to complete my intermediate school (ESO) and a more advanced course in marketing, business, and e-commerce. Currently I am not working because I am back on dialysis, but I want to finish the course internship and get to work.
Fortunately, I met a wonderful girl 4 years ago with whom I am very happy, who supports me and understands me.
I still live with my parents, because I don't have a job, but I would like to become independent soon.
The truth is that I am happy with my life, although it differs a lot from that of my friends, who, at my same age, have their jobs and their lives are very different.
I don't usually do much sport, I've always been a very sedentary boy, but it doesn't stop me from taking care of my diet and I always try to control my weight.
The eating habits on dialysis are much stricter, both because of the food and the drink, and I have to control myself much more so as not to carry too much weight on the days of dialysis, and there are foods that I cannot take.
The kidney issue has influenced my development: I could have been somewhat taller.
• … Regarding my personal life, I am still at my parents' house, without a partner and I obtained my school certificate a year ago at adult school, but starting with COVID my life stagnated again. My physical development has been adequate with respect to my family, in size and weight. But my life, compared to that of people my age, is very different, I do not carry out the activities that a person of my age could do; the whole problem has affected my personal life, but I try to carry on as well as I can…
• Since you transferred me to adult clinic, everything about the kidney is very good so far, and God-willing it will continues this way, I am very responsible with my treatment. I still hear badly.
After 5 years of transplantation, in 2009, I was diagnosed with a bulb cavernoma due to bleeding in the brain; I was very ill and half my body was paralyzed, I did not see well, I had double vision. After a year it happened again, in the area where it was they could not operate, and I spent two years until I recovered.
Thank God the cavernoma was absorbed slowly, and since then I have been followed up every year and have an MRI. The secuela that has stuck with me is that if I look sideways I see double; otherwise everything is fine, despite the fact that I had a very bad time.
About studies, I missed many classes and courses, I did not make enough progress, it was very difficult for me to memorize and study, with the problem of hearing it is very difficult for me to grasp and understand things. I got my ESO certificate with a lot of effort and help from my mother and teachers. When I recovered from the paralysis, I got my driver's license, which also was difficult and it took a lot of effort.
As for work, I dedicated myself to going with my father to fix gardens and swimming pools, and I'm still with him.
I don't currently have a partner or children; I had two partners, but it didn't go well. I live with my parents and I have never been independent.
I am happy, I get along very well with my parents, my sister and my friends, but my friends, unlike me, perform much better in all aspects of life. Sometimes I ride my bike or play football. I have no eating problems and I like all kinds of food. My physical development has not been the one that would correspond to me in size or weight.
I would consider that it would be very good if there were psychologists in hospitals, since it is very hard to live this situation and spend so many years in the hospital or visiting hospitals, since I have not stopped since birth. This whole situation, everything I have experienced, has created dependence on my parents and I am not able to take care of myself independently.
FundingThis work has not received any grants or scholarships from public or commercial agencies or non-profit entities.
Conflict of interestsThe authors have no conflict of interests to declare.
We thank all our patients for the affection they have transmitted to us in all their answers, for having collaborated with us by telling us about their experience and their life, and what they have taught us with their attitude in the face of all their adversities.



