



In 2015, were celebrated in Brazil 50 years of kidney transplants, whose activities have been registered since 1995 by the Brazilian Association of Organ Transplantation (ABTO).
PurposeTo evaluate the quantitative evolution of renal transplants that occurred in Brazil during the period from 1995 to 2015 and to classify the country's position in the international scenario.
MethodsEcological and retrospective study, based on data records published by ABTO and the International Registry in Organ Donation and Transplantation (IRODaT).
ResultsDuring the period evaluated, there were 75,479 kidney transplants in Brazil, 43,771 (58%) of deceased donors. The southeastern region had the highest absolute number (n=44,746; 59.3%) and, the north, the lowest (n=1159; 1.6%). The cumulative percentage variation of transplants was 121%, and the annual variation was negative on six occasions (1996, 1997, 2002, 2005, 2006, 2015). The number of effective transplantation teams had a weak relation with the number of procedures performed (r=0.45, p: 0.03). Brazil was the second country with the highest absolute number of transplants in the period of analysis, considering a world ranking with 30 nations.
ConclusionThe number of renal transplants in Brazil increased significantly over the years. However, the efforts of those involved in the different phases of the donation-transplant process should be continuous.
En 2015, se conmemoraron 50 años de realización de trasplantes renales en Brasil, cuyas actividades son registradas desde 1995 por la Asociación Brasileña de Trasplante de Órganos (ABTO).
ObjetivosEvaluar la evolución cuantitativa de los trasplantes renales ocurridos en Brasil durante el período 1995 a 2015 y clasificar la posición del país en el escenario internacional.
MétodosEstudio ecológico y retrospectivo, basado en registros de datos divulgados por la ABTO y por el International Registry in Organ Donation and Transplantation (IRODaT).
ResultadosEn el período evaluado, ocurrieron 75.479 trasplantes renales en Brasil, siendo 43.771 (58%) de donantes fallecidos. La región sudeste presentó el mayor número absoluto (n=44.746, 59,3%) y, al norte, el menor (n=1.159, 1,6%). La variación porcentual acumulada de trasplantes fue del 121% y la variación anual fue negativa en seis ocasiones (1996, 1997, 2002, 2005, 2006, 2015). El cuantitativo de equipos trasplantadores efectivos tuvo una débil relación con el número de procedimientos realizados (r=0,45, p-valor: 0,03). Brasil fue el segundo país con mayor número absoluto del trasplante en el período de análisis, considerando un ranking mundial con 30 naciones.
ConclusiónEl cuantitativo de trasplantes renales en el país presentó un importante incremento a lo largo de los años. Sin embargo, los esfuerzos de los involucrados en las diferentes fases del proceso de donación-trasplante deben ser continuos.
It is estimated that the worldwide prevalence of chronic kidney disease (CKD) is between 11% and 13%1 and that approximately five million people require renal replacement therapy (RRT).1,2 In Brazil, the epidemiological indicators related to this disease have increased rates over the years. Only in 2014, more than 100 thousand Brazilian patients performed dialytic treatment.3 For those who require RRT, the expected improvement in survival is in the performance of a kidney transplant (KT).4
In this direction, since 1954, the year in which the first successful KT in the world (specifically in the city of Boston – United States of America – USA), several advances in the field of medicine and health sciences as a whole have contributed to that more and more individuals with end-stage CKD can benefit from this treatment modality. Currently, KT is a routine procedure in thousands of transplant centers around the world.4–6
In Brazil, registration of the first KT occurred just over 50 years ago, that is, about a decade after the conclusion of the first procedure with positive results worldwide. It was in the early 1960s, in the midst of a turbulent historical-political context experienced by the country at the time (military dictatorship), that work began on the realization of the first KT on Brazilian soil.5,6
In the context of the panorama presented here, it is understood that the epidemiological studies are important within the analytical context of the triad “structure, processes and results” involving KT in Brazil, since the data encourage the planning of new public policies aimed at improving the system and, consequently, the process of donation-transplantation as a whole.3–6
In this sense, this research aimed to evaluate the quantitative evolution of KT in Brazil during the period from 1995 to 2015 and to classify the country's position in the international scenario.
MethodsThis ecological and retrospective study is the analysis of the KT records that occurred in Brazil and the world between 1995 and 2015. Data from the national bank maintained by the Brazilian Association of Organ Transplantation (ABTO), called the “Brazilian Registry of Transplantation – RBT”,7 which is published through periodic electronic editions and free access to both the academic and scientific community as well as to the general population.
With the use of a structured and specifically designed form for this study, the following data were extracted from the RBT: absolute (gross) and adjusted (per million population) KT occurring in each year of evaluation, according to the type of donor (living or deceased) and the regional geographical location of occurrence (northeast, north, central-west, southeast and south); number of effective transplantation teams (who performed at least one kidney transplant over a year). In addition, the absolute and adjusted numbers of KT occurred worldwide in the same period of the national evaluation (1995 to 2015) were extracted from the International Registry in Organ Donation and Transplantation (IRODaT).8
In order to carry out an evaluation of updated information, the data were “reverse-collected”, i.e., for all variables, data were extracted from the most recently published edition. In this way, the figures up to the year 2005 were taken from the annual RBT of 2015 and, therefore, the data referring to the successor years to 2005 were extracted from the annual RBT of 2016.
Nevertheless, considering that the data of interest in this study are continuously updated, it should be pointed out that the results presented refer to the analyzes performed on the data available on the ABTO and IRODaT electronic website in February 2017, the month in which if the data were collected.
Statistical analysisAfter being collected, the data were tabulated in spreadsheets of the software Microsoft Excel®, version 2010, and then exported to the statistical program R,9 for which the analyzes were performed. Descriptive analyzes of all variables of interest were performed and Pearson's correlation test was applied (after verification of normality by the Shapiro–Wilk test and the sample's homoscedasticity by F-test) to verify the association between the absolute number of transplants and transplantation teams during the period evaluated. The level of significance was p<0.05.
Ethical aspectsBecause it was a research whose objectives returned to the evaluation of secondary data of public access, it was considered that it is not necessary to obtain an opinion from the Ethics Committee in Research of the institution to which the researchers are linked, as well as authorization from the entities that disclose the data. In spite of this, all sources of data were duly cited and the ethical principles established by the Resolution of the Brazilian National Health Council n°. 466, of December 12, 2012, were respected.
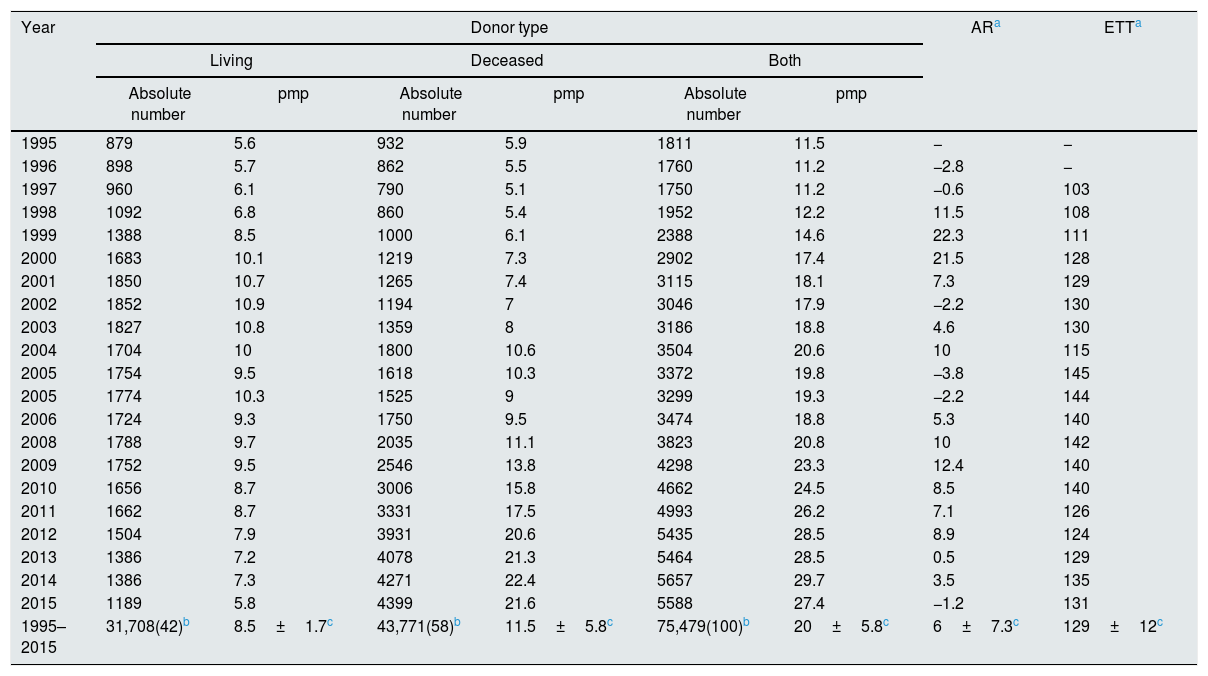
ResultsBetween 1995 and 2015, there were 75,479 KT in Brazil, 43,771 (58%) of deceased donors. By adjusting the data to the population quota, an average of 20±5.8 transplants/year per million population was identified. The number of effective transplantation teams had a weak relationship with the number of transplants (r=0.45; p=0.03) and ranged from 103 (1997) to 145 (2005), and in the last year of analysis there were 131 teams. The cumulative percentage growth of transplants during the whole period was 308.6%, but the annual percentage change was negative on six occasions (Table 1).
Kidney transplants occurred in Brazil (1995–2015).
| Year | Donor type | ARa | ETTa | |||||
|---|---|---|---|---|---|---|---|---|
| Living | Deceased | Both | ||||||
| Absolute number | pmp | Absolute number | pmp | Absolute number | pmp | |||
| 1995 | 879 | 5.6 | 932 | 5.9 | 1811 | 11.5 | − | − |
| 1996 | 898 | 5.7 | 862 | 5.5 | 1760 | 11.2 | −2.8 | − |
| 1997 | 960 | 6.1 | 790 | 5.1 | 1750 | 11.2 | −0.6 | 103 |
| 1998 | 1092 | 6.8 | 860 | 5.4 | 1952 | 12.2 | 11.5 | 108 |
| 1999 | 1388 | 8.5 | 1000 | 6.1 | 2388 | 14.6 | 22.3 | 111 |
| 2000 | 1683 | 10.1 | 1219 | 7.3 | 2902 | 17.4 | 21.5 | 128 |
| 2001 | 1850 | 10.7 | 1265 | 7.4 | 3115 | 18.1 | 7.3 | 129 |
| 2002 | 1852 | 10.9 | 1194 | 7 | 3046 | 17.9 | −2.2 | 130 |
| 2003 | 1827 | 10.8 | 1359 | 8 | 3186 | 18.8 | 4.6 | 130 |
| 2004 | 1704 | 10 | 1800 | 10.6 | 3504 | 20.6 | 10 | 115 |
| 2005 | 1754 | 9.5 | 1618 | 10.3 | 3372 | 19.8 | −3.8 | 145 |
| 2005 | 1774 | 10.3 | 1525 | 9 | 3299 | 19.3 | −2.2 | 144 |
| 2006 | 1724 | 9.3 | 1750 | 9.5 | 3474 | 18.8 | 5.3 | 140 |
| 2008 | 1788 | 9.7 | 2035 | 11.1 | 3823 | 20.8 | 10 | 142 |
| 2009 | 1752 | 9.5 | 2546 | 13.8 | 4298 | 23.3 | 12.4 | 140 |
| 2010 | 1656 | 8.7 | 3006 | 15.8 | 4662 | 24.5 | 8.5 | 140 |
| 2011 | 1662 | 8.7 | 3331 | 17.5 | 4993 | 26.2 | 7.1 | 126 |
| 2012 | 1504 | 7.9 | 3931 | 20.6 | 5435 | 28.5 | 8.9 | 124 |
| 2013 | 1386 | 7.2 | 4078 | 21.3 | 5464 | 28.5 | 0.5 | 129 |
| 2014 | 1386 | 7.3 | 4271 | 22.4 | 5657 | 29.7 | 3.5 | 135 |
| 2015 | 1189 | 5.8 | 4399 | 21.6 | 5588 | 27.4 | −1.2 | 131 |
| 1995–2015 | 31,708(42)b | 8.5±1.7c | 43,771(58)b | 11.5±5.8c | 75,479(100)b | 20±5.8c | 6±7.3c | 129±12c |
Legend: pmp=per million population.
When analyzing the quantitative of KT according to the geographic location, it was verified that the southeastern region presented the highest absolute number (n=44,746; 59.3%) of the procedures performed, while the northern region, the lowest (n=1159; 1.6%) (Fig. 1).
. Legend: n (%); †mean ± standard derivation.")
Regarding the position in the world ranking, it was verified that Brazil was the second country with the highest absolute number of kidney transplants between 1995 and 2015, in a list of 30 nations (Fig. 2). However, in 2015 the country ranked 25th in the world in terms of number of kidney transplants adjusted according to the population quota in that year, presenting a rate of 27.4 transplants per million population (Fig. 3).
DiscussionInternal analysis.")
 and per million population rate (B).")
From the year in which KT activities began in Brazil to the present day, the number of procedures performed presented an evolutionary rate above 300%, from 1811 transplants in 1995 to 5588 in 2015. It was also verified that until the year 2005 the transplants occurred mainly in the face of inter-living donation. As of 2006, there was an inversion, and since then, there has been a higher proportion of transplants performed by the allocation of organs from deceased donors (Table 1).
It was no coincidence that in 2006, the creation of the Intra-Hospital Commissions for Donation of Organs and Tissues for Transplants (CIHDOTT) was instituted, through Ministerial Order n°. 1262. Acting locally, that is, directly within health institutions, CIHDOTTs have among their responsibilities the responsibility of promoting the organization of care protocols for organ donation.10 From the actions of CIHDOTTs, the amount of post-mortem donations was substantially high. In the year of creation of these commissions, the number of KT from deceased donors was just over half of the total. By 2015, transplants from deceased donors were equivalent to approximately 79% of the procedures performed (Table 1).
Although the activities developed by the CIHDOTTs contributed unequivocally to the evolution of the donation-transplant process in Brazil, it should be noted that other factors were equally important. Among these factors, technological advancement, human resource development and training, and the large number of task forces for population sensitization, carried out by health professionals, labor classes, governmental and non-governmental entities and bodies, are cited.5,6
However, there was a significant regional disparity in the total and average number of transplants performed. While the Southeast region had a mean KT (3729±3717) higher than the national average (3594±1276) and was responsible for 59.3% of surgeries for this purpose between 1995 and 2015, the quantitative effect in northern and in the same period, it was small and represented 1.6% and 5.4% of the total, respectively (Fig. 1). In fact, this fact can be influenced by the great territorial extension of the country. The northern region, for example, is the most extensive of the five Brazilian regions. The State of Amazonas, with its more than 1.5 million square kilometers, has an area greater than the extension of the territories of the south and southeast regions together,11 as well as superior to the territories of several nations. Another issue, which may also have an impact on geographical differences, is the population contingent.
The great territorial extension of the country combined with the significant number of inhabitants (more than 200 million in 2015), favors the existence of regional niches more or less economically developed, depending on the existing local population conglomerate. This is because, in the first instance, it is precisely the population of a given region that determines the aspects related to its territorial development.12 However, it is certainly understood that the influence of the population on the quantity of transplants is due to the awareness of the act of organ donation rather than intervention over other aspects of the process. Thus, it is suggested that existing inequality is one of the innumerable reflexes of the economic-social inequality that, historically, plagues Brazil.
In 2012, the sum of the Gross Domestic Product (GDP) of the Southeast and South regions corresponded to 70% of the national GDP, and the state of São Paulo (Southeast) presented and has been showing the country's largest GDP, concentrating good part of the Brazilian income, especially in the city of São Paulo.13 Thus, when mentioning regional economic development, as a factor that exerts influence on the disparity in the numbers of KT, it is also necessary to consider both efficiency- and effectiveness of the process regarding the cost-effectiveness of the procedures.5,6
In five years (from 2006 to 2011), the total average spending of the states and the Federal District with kidney transplants, including hospital and professional expenses, increased by 103.83%. However, capturing and transplanting activities remained at the end of the period more efficient in terms of productivity in the states located in the Southeast and South regions,14 which corroborates with the results of the present research, in which it was identified that in the referred more than 80% of the total kidney transplantation in the period evaluated (Fig. 1).
In a study conducted by members of the Institute of Applied Economic Research, it was possible to verify that, in 2006, the percentage of KT needs met by the states showed great variation, ranging from 0.12% in Mato Grosso (central-west) to 32.72% in Santa Catarina (southern region). In addition, the study also highlights that, in that year, the rate transplantation teams per million population showed higher in the Southeast and South regions.15
This context portrays a multifaceted problem, which is evidenced both in the disparity of recruitment and transplant numbers, and by the existence of overloaded and poorly distributed teams of CIHDOTTs and inactive Organ Procurement Organizations, as well as weakly engaged state power stations, among other aspects, arising from the binomial “causes-consequences” of the managerial inefficiency and inefficiency of the decentralized system.14,15
Regarding cost-effectiveness, there is evidence in the literature that KT presents more benefits, both from the clinical point of view (by improving patients ‘quality of life’)16–18 and financial (given the lower monetary cost with patients’ treatment),18,19 in comparison to RRT modalities. Given the complexity of the process and the Brazilian system itself, the difficulties experienced by the country in relation to the existing regional discrepancies present multidimensional determinants and, therefore, the mentioned aspects are only some of the possible causes, which go far beyond, whose discussion on the subject demands further study. In spite of this, it is emphasized that the creation of a system, based on the principles of universal access and integrality of assistance and, above all, gratuitous, represented a revolutionary framework in the historical-epidemiological context of KT occurred in Brazil.
Brazil's position in the international scenarioEstablished by Decree n°. 2.268, on June 30, 1997,20 the Brazilian National Transplant System (Brazilian-NTS) is considered to be the largest public transplant system in the contemporary world.5,6,21,22
The Brazilian-NTS's good reputation is due, in particular, to its position in the world transplant ranking. As can be seen in Fig. 2, throughout the evaluated period, only the USA performed a number of surgeries of KT superior to Brazil. It is worth noting that, in addition to possessing about 100 million inhabitants more than Brazil (which invariably raises the amount of donors), the USA is also a universal reference in terms of organ harvesting, due in large part to part, for the juridical conformation that it possesses, with respect to the donation-transplant process.23
Unlike in our country, where inter-living donation occurs only between people who are in the bloodstream up to the fourth degree, and post-mortem donation occurs through the consent of the spouse or blood relative to the second degree,24 the USA law allows what is called the kidney paired donation (KPD).25 Through KPD, a person who wishes to donate a kidney to a family member who needs it, but unfortunately is not compatible with the family, can donate to another patient with whom he/she has no blood relationship, presents the necessary compatibility for the accomplishment of the procedure.25 In addition, to obtain organs from deceased donors, there is no need for family consent, since the USA adopts the presumed consent law.23 The KPD method and the presumed donation generate controversy and great discussions, from the clinical, ethical, political and financial point of view.
Even with all the difficulties, Brazil was ahead of the great powers of the world, such as England, Spain, Holland and Croatia, in the absolute number of KT performed (Figs. 2 and 3A). These countries also have international respect in the field of transplants (renal and other organs/tissues), since they present the best per capita rates of procedures. Fig. 3B shows that the Netherlands and Spain had the highest transplant rates per million population in the year 2015.
Globally recognized, the Spanish model presents the best rates of organ donation in the world. In 20 years, Spain jumped from 14.3 to 34.4 donors per million population. This is a result of a number of changes in the country's system, including the implementation of a network for coordination of transplants, improvement of coordinators’ profiles, training and permanent education of health professionals (especially doctors and nurses working in units intensive care and emergency and emergency services), investments and efforts aimed at post-mortem donations, support to professionals working at the local level given by representatives of the national body, intense work with the mass media for population awareness and financial reimbursement to hospitals for the activities developed, among others.26
In recent years, Brazil has also experienced an increase in the effective donor rate, from nine in 2009 to 14.6 donors per million population in 2016. Among the factors that block an even more significant increase is the family refusal to attract of organs of deceased donors, which represents more than 40% of the reasons for not donating donations in the country.27 This situation aggravates, even more, the problem of the disproportion between supply and demand in Brazil. Thus, in an attempt to minimize the disposal of organs in which the donation is consented, some Brazilian teams perform transplants with donors of expanded criteria (DEC).
They are classified with DEC patients older than 60 years or between 50 and 59 years old and with at least two of the following conditions are classified as having a history of hypertension; serum creatinine concentration greater than 1.5mg/dl; cerebrovascular accident as cause of death.28 According to the literature, considering DEC may have a significantly positive impact on the number of organs allocated for KT.29 Moreover, patients transplanted with DEC kidneys, although they have a delayed rate of graft function, appear to present a similar survival to that seen in patients transplanted from organs of donors with standard criteria.28–31
Needs for continuous improvementThe use of DEC kidneys is just one of the innumerable strategies adopted in an attempt to expand the allocation of organs that, therefore, make it possible to reduce the extensive quantitative number of patients in waiting queues for transplants. Other strategies should include continuous improvement of public policies, especially in relation to better distribution of resources (material, human, financial, logistic, etc.), and updating of legal provisions; continuing and continuing education; promote evidence-based (professional) practice; awareness of the importance of donating organs; make available statistics on transplants that are carried out in the country; encourage everyone to talk about giving and warn their families about the desire to be a donor. From this, it may be possible to subsidize the narrowing of regional disparities and the gap between supply and demand, as well as to keep Brazil prominent on the international scene, allowing Brazilian-NTS to continue to be a model for several nations.
Limitations of the studyWe have included some additional information in the electronic supplementary material. However, we recognize that the study has limitations. Due to the retrospective collection, it was not possible to recover important data for more comprehensive analysis. Information on the total number of transplantation centers (and not only the effective centers); demographic data for each region of country (with the respective transplant rates per million of population, for each year analyzed), as well as refusal data for donation presented for each region/year, among others, would contribute to a better analysis on the kidney transplants in the Brazil.
ConclusionMore than five decades after the first procedure in Brazil, the number of kidney transplants in Brazil has shown significant growth over the years. Thus, it is possible to say that there are reasons to celebrate. However, internal disparities are still significant. Thus, it is imperative that all actors involved in the process carry out their actions in an integrated and articulated way, in order to minimize regional discrepancies and to sustain the country as an international model, not only with regard to renal transplants, but with respect to the transplants as a whole.
Authors’ contributionsAll authors have contributed substantially to the submitted work and have read and approved the final manuscript. In particular, Santos RP participated in the drafting of the manuscript and critically revised the manuscript. Carvalho ARS and Peres LAB critically revised the manuscript.
FundingNil.
Conflict interestsThe authors declare no conflict interest.



