





Hemodialysis (HD) is a treatment with a significant environmental impact. One dialysis cycle is equivalent to the daily consumption of 3.5–4 people, and the average annual electricity consumption of a center is equivalent to that of approximately 2.5–3 households (9 kWh/day per household). The carbon footprint (kg CO2 equivalent) measures direct and indirect greenhouse gas emissions and is influenced by the production of the various materials used, their transport, patients, and healthcare personnel. In this context, it is necessary to understand the real impact of each center on the environment and act sustainably. The aim of this review is to analyze the environmental footprint generated by dialysis, rethink processes, and propose management strategies to provide tools applicable to any unit to reduce the negative impact of this activity. Each center must measure and monitor indicators, set its own standards, design improvement plans, and carry out annual monitoring in a multidisciplinary manner.
La hemodiálisis (HD) es un tratamiento con gran impacto en el medio ambiente. Un ciclo de diálisis equivale al consumo diario 3,5−4 personas y el consumo anual medio de electricidad de un centro se equipara al de aproximadamente 2,5 a 3 hogares (9 kWh/día por hogar). La huella de carbono (kg CO2 equivalente) es la medida de las emisiones directas e indirectas de gases de efecto invernadero y está influida por la producción de los distintos materiales utilizados y el transporte de estos, de los pacientes y el personal sanitario. En este contexto se hace necesario conocer el impacto real de cada centro en el mediomabiente y actuar de una manera sostenible. El objetivo de esta revisión es analizar la huella medioambiental que genera la diálisis, repensar los procesos y plantear estrategias de gestión con el fin de aportar herramientas aplicables a cualquier unidad para reducir el impacto negativo de esta actividad. Cada centro debe medir y hacer seguimiento de indicadores, fijar su estándar, diseñar planes de mejora y realizar seguimiento anual de manera multidiciplinar.
“We never know the worth of water till the well is dry,” Thomas Fuller, historian.
Climate change is the most significant threat to human health and well-being this century. Human activities have played an essential role in the climate and ecological crisis, mainly due to the emission of greenhouse gases. The recent climate emergency declaration1 raises social awareness with regards to evaluating the sustainability of a multitude of economic and daily activities, including those in the field of healthcare, such as nephrology.
Although many healthcare professionals are fully aware of the impact of climate change and feel a responsibility to raise public and policy makers' awareness of the issue,2 environmental sustainability is not prioritised in clinical practice: not in the infrastructure, nor in the management systems.3 This highlights the need to address this challenge in nephrology in a multidisciplinary manner, particularly with regards to haemodialysis (HD), which has a significant environmental impact.
This paper will discuss the environmental footprint of dialysis and reflect on our current and usual practices, rethinking the processes and proposing a number of management strategies, with the aim of reducing this activity's negative impact.
Environmental impact of haemodialysis and how it is measuredIn the setting of HD centres, the most recommended indicator (due to its simplicity, sensitivity and easiness to interpret ) is the relationship between water and electricity usage, and waste generation, with the number of dialysis sessions performed.
Three key performance indicators (KPIs) are identified4:
- a
Water usage (l/session).
- b
Electricity usage (kWh/session).
- c
Waste generation (kg/session).
These key indicators are supplemented by measuring the carbon footprint (kg CO2 equivalent), which is the measurement of the direct and indirect emissions of greenhouse gases produced by an individual, organisation, product or service. The factors that most influence the carbon footprint are the production of the different materials used (drugs, solutions, consumables)5 and transportation (patients, healthcare personnel and material).6 Each centre must set its own carbon footprint standard, design plans to reduce it7 and carry out annual monitoring.
Water usageHD is a major devourer of water resources. For reference purposes, one dialysis cycle consumes as much water as 3.5–4 people per day at the centre.8 Ultrapure water is generated at the water plant, the efficiency of which depends on various factors: on the one hand, the supply water (conductivity, salinity, hardness, suspended elements and seasonal variability); and on the other hand, the design of the treatment and pretreatment plant (some designs are more efficient than others for saving waste water and the shelf life of the reverse osmosis membranes). The technology used can achieve a recovery rate of 50%–75%.9 Finally, the efficiency of the HD session depends on the size and operation of the centre. Larger facilities, even though they use a higher total amount of water, can be more efficient since almost all of the water is used for treatment. In small centres, part of this water usage, especially if the centre dialyses on alternate days, is used for ring washing and regeneration of some elements of the treatment plant, even if dialysis is not carried out that day. By way of example, in a study conducted in 12 of our centres over three years (2019–2021), with an average of 10,541.5 ± 7264 (range 756−22,436) HD sessions per year, large centres (>10,000 sessions per year) consumed a greater amount of water than small ones (<10,000 sessions) (5910 vs 2437 m3 year) (P < .001). However, water usage per HD session was significantly lower in large centres than in small ones (367.3 vs 589 l/HD (P < .001).10
Two of the consequences of the climate crisis are variations in temperatures and weather patterns. Sensitive regions, such as the Mediterranean basin, will be affected by an increase in the number and intensity of heat waves, which will contribute to periods of drought with storms and floods.11 A 15% decrease in rainfall is projected according to the most conservative models, which will significantly affect the planet's water resources12 and, as a direct result, dialysis techniques. Each conventional HD session (duration of four hours) can require up to 500 l of mains water,13 with only a third being used directly as dialysate (500 ml/min × 4 h = 120 l, not counting disinfection water). For on-line haemodiafiltration (OLHDF), the usage of replacement fluid needs to be added to these figures. In addition, maintaining the water plant also entails additional usage, as we have already mentioned, washing and regeneration processes, keeping the water in the ring in constant motion, disinfection, etc.
Energy expenditureThe indicator that measures the energy expenditure of an HD unit is electricity usage (kWh)/session. The average annual electricity usage of the centre can be equated to the estimated daily usage of approximately 2.5–3 households (estimated average usage of 9 kWh/day per household).14 The energy expenditure in an HD centre is multifactorial. In addition to the usage of the monitors themselves (between 1.5–3 kWh/session), other costs are involved in this type of treatment that need to be calculated,15 such as the energy usage of air conditioning, lighting and other equipment (computers, storage refrigerators, water treatment or osmosis systems, thermal disinfection, automation of centralised concentrates and patient televisions, etc.), as well as transportation.
Waste generationThe production and distribution of materials used in haemodialysis is a multifaceted process with significant environmental implications. Transportation from manufacturing plants to distribution centres and, ultimately, to healthcare facilities, requires significant energy expenditure and logistical coordination, contributing to carbon emissions and air pollution. The decision in a unit to use individual acid canisters for all patients or to use centralised acid for the majority and canisters for those requiring more personalised treatment can have a major environmental impact. Materials used in haemodialysis predominantly include plastics, polymers and other synthetic compounds, reflecting the strict requirements for biocompatibility, durability and sterility.
The waste generated in the haemodialysis process is classified according to its nature (Fig. 1):
- 1
Group I (waste similar to urban waste): paper and cardboard (product boxes, packaging, office paper), containers (plastic and metal, medical device wrappers, empty concentrate canisters), organic waste, glass and other unclassifiable waste (the so-called remainder).
- 2
Group II (non-specific medical waste): dressing material, bandages, plasters, blood-stained single-use tissue, secretions, gloves, lines and used and emptied haemodialysers, as well as all waste not classifiable as hazardous.
- 3
Group III (medical waste with biological hazard): which would include blood and blood products in liquid form, live and attenuated vaccines, anatomical waste without sufficient entity, cultures, infectious agents, animal waste for research, as well as sharp and cutting material, such as needles, scalpel blades and slides.
- 4
Group IV and Group V (cytotoxic material with mutagenic, carcinogenic or teratogenic properties, biohazardous medication, chemicals).

Waste generation is linked to both quantity (kg/HD session) and type of material. Of particular interest is waste that is reusable or easily recyclable with a view to extending their life cycle or reducing the carbon footprint resulting from their management, which depends on the waste group and its subsequent processing (recycling, reuse, landfill or incineration). The bulk of the waste generated by HD will usually fall within groups I and II, and to a lesser extent group III. Nonetheless, we should not forget the huge amount of paper consumed in HD units, which can be minimised.
TransportTransporting this material from manufacturing plants to distribution centres, and ultimately to healthcare facilities, requires considerable energy expenditure and logistical coordination, contributing to carbon emissions and air pollution. The same applies to transportation used by staff and patients.
Actions towards environmentally sustainable haemodialysisIn order for any activity to be carried out, it needs an input of energy, materials, consumables and raw materials, etc. Therefore, in dialysis there will always be usage and emissions generated in proportion to the scale of the activity.
It should be noted that any measure or action to not use any electricity or water, or generate any waste (zero emissions) is completely unfeasible. In the short term, the best policy is to minimise energy and water usage, and waste generation (which will never be zero). In the long term, moving towards a zero-emissions policy makes sense through the use of offsetting systems (photovoltaic panels, implementation of CO2 capture systems, planting of trees, extended manufacturer responsibility).
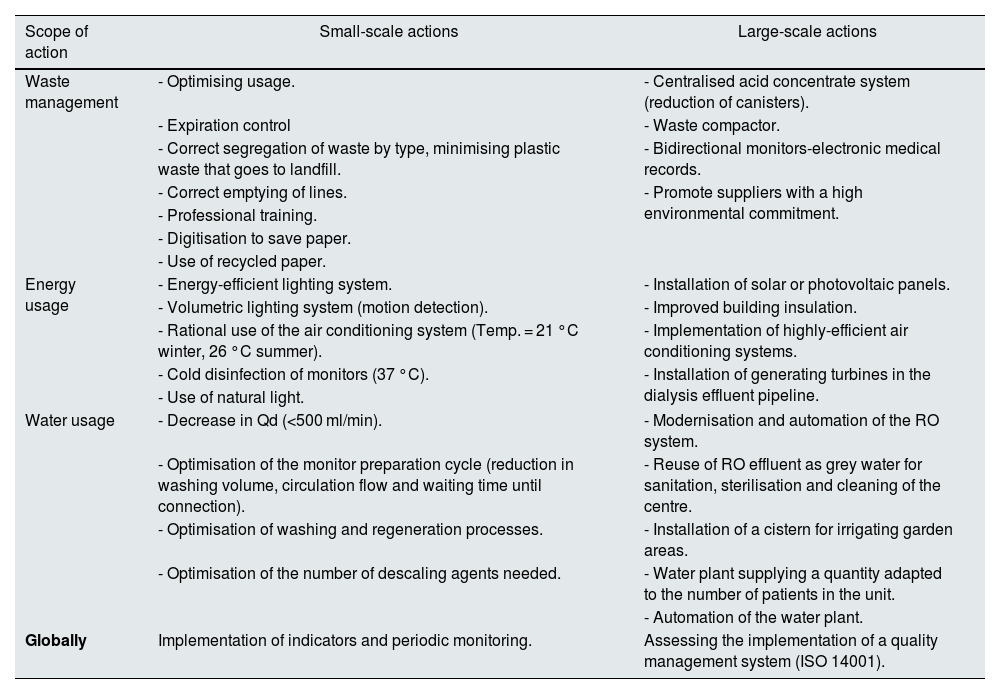
The need to focus actions towards a more environmentally friendly model in the field of dialysis has been clearly stated in the literature.16–18 In order to make a gradual transition towards a more sustainable treatment, indicator measuring systems, environmental impact and efficiency analysis should be introduced as an initial step, according to the needs and limitations of each centre (Table 1).
Possible actions to take according to scale and scope of action.
| Scope of action | Small-scale actions | Large-scale actions |
|---|---|---|
| Waste management | - Optimising usage. | - Centralised acid concentrate system (reduction of canisters). |
| - Expiration control | - Waste compactor. | |
| - Correct segregation of waste by type, minimising plastic waste that goes to landfill. | - Bidirectional monitors-electronic medical records. | |
| - Correct emptying of lines. | - Promote suppliers with a high environmental commitment. | |
| - Professional training. | ||
| - Digitisation to save paper. | ||
| - Use of recycled paper. | ||
| Energy usage | - Energy-efficient lighting system. | - Installation of solar or photovoltaic panels. |
| - Volumetric lighting system (motion detection). | - Improved building insulation. | |
| - Rational use of the air conditioning system (Temp. = 21 °C winter, 26 °C summer). | - Implementation of highly-efficient air conditioning systems. | |
| - Cold disinfection of monitors (37 °C). | - Installation of generating turbines in the dialysis effluent pipeline. | |
| - Use of natural light. | ||
| Water usage | - Decrease in Qd (<500 ml/min). | - Modernisation and automation of the RO system. |
| - Optimisation of the monitor preparation cycle (reduction in washing volume, circulation flow and waiting time until connection). | - Reuse of RO effluent as grey water for sanitation, sterilisation and cleaning of the centre. | |
| - Optimisation of washing and regeneration processes. | - Installation of a cistern for irrigating garden areas. | |
| - Optimisation of the number of descaling agents needed. | - Water plant supplying a quantity adapted to the number of patients in the unit. | |
| - Automation of the water plant. | ||
| Globally | Implementation of indicators and periodic monitoring. | Assessing the implementation of a quality management system (ISO 14001). |
The energy efficiency of HD is related to the electricity usage of the monitor, the water treatment plant and thermal disinfection, as well as the air conditioning and lighting of the facilities. Both air conditioning and lighting must meet optimal standards of well-being for both healthcare personnel and patients, ensuring the maximum possible efficiency in the use of energy resources.
In order to be more energy efficient, the following measures can be considered, always taking into account the optimal conditions of well-being for staff and patients:
- a
Lighting.
One of the simplest measures is the installation of energy-efficient LED lights and motion sensors that activate the centre's lighting devices to reduce electricity usage in general and in unnecessary periods (night, non-active days).
- b
Air conditioning options.
Royal Decree-Law 14/202219 stipulates that heating and air conditioning in public buildings should not exceed 21 °C in winter or be below 26 °C in summer. For patients on dialysis, it should be considered that changes in the temperature of the dialysate can increase or decrease their body temperature. For the well-being of these patients, it is important to either adjust the temperature for their comfort or use blankets (which also entail a cost of manufacturing, periodic washing and replacement). Other measures include proper compartmentalisation and insulation of rooms, the use of materials to minimise dissipation losses and the use of highly-efficient air conditioning systems.
- c
Green energy generation.
The possibility of installing solar panels or photovoltaic solar energy to cover part of the centre's demand should be evaluated.
- d
Cold disinfection.
An easy strategy to implement is the use of monitors that allow cold disinfection (37 °C), as opposed to high temperature disinfection (80 °C), but this will depend on the chemicals involved.
- e
Energy reuse.
A novel alternative is the installation of generating turbines in the different stages of the reverse osmosis (RO) system, which allow part of the energy consumed to be recovered through mechanical energy.20
Water usageCentres consume water in healthcare activities as well as in healthcare-related tasks, such as cleaning, bathrooms, hand washing and dishwashing. There are a number of strategies that could be put in place to optimise dialysis water usage (Fig. 2):
- a
Rationalising dialysis bath flow.

While there is a downward trend, practices whereby the dialysate flow is between 700−800 ml/min21 (including usage for its generation) are still common. Given that climate change will have an impact on drought, emphasis must be placed on optimising water usage. For some years now, there has been an insistence on rationalising the dialysis flow at 500 ml/min, even in OLHDF techniques. Higher values demonstrate only a marginal contribution, both in the dialysis dose (Kt)22,23 and in the clearance of uraemic toxins.24,25
- b
Modification of priming and flushing strategies, as well as washing and regeneration processes of the pretreatment elements and the ring.
- c
Assess the number of water softeners needed based on the hardness of the water (fewer water softeners save water and the salt required for the process).
- d
Water reuse.
Possibility of using the water discarded at various stages of its use (in the reverse osmosis [RO] system or from the haemodialyser effluent fluid):
- •
Water rejected by the RO system: there are systems that achieve reject water recycling rates of 50%–75% by passing it through osmosis again. The waste water meets quality standards26,27 and can be used for other purposes: supply for toilets (WC), steam for sterilisation28 or irrigation of garden areas.29 In other innovative trials, waste is used in a horticulture and aquaponics system.30
- •
Effluent liquid from monitors: there is reluctance to reuse it owing to its high salinity and content of phosphates, nitrates and microorganisms.31,32 However, standard waste water treatment processes allow the recovery of nutrients with high fertiliser value for the agricultural sector.33,34 Nonetheless, these measures are not without cost.
- a
Scalable water plant that generates sufficient quantities of water for the number of patients in the unit.
- b
Water plant automation.
- a
Ensuring that the absence of chemical and microbiological contamination is a priority for all HD units. All components of the system are involved in this process: water supply, arrival at the monitor, design of the treatment plant, etc. The implementation of digitisation and remote control in water plants, compared to conventional advanced sensor technology, can increase energy expenditure, but reduces water usage and the number of trips by technical staff (from 486 h to 92 h), substantially reducing the environmental impact.35
- a
Other actions: plumbing and sanitation maintenance, review and updating of quality standards, as well as introducing new technologies and optimised dialysers, dry cleaning techniques, installation of aerators on taps and reduction of toilet water usage.
Waste reduction and management and its proper segregation must be an objective in dialysis units. This can be achieved by:
- •
Optimising usage.
- •
Expiration control.
- •
Cleaning of lines and dialysers to make them suitable for municipal recycling.
- •
Prioritising sustainable suppliers.
- •
Reducing reliance on paper thanks to digitisation and bidirectional connection between monitors and electronic medical records (if paper is used, it should ideally be recycled).
- •
Using centralised systems (lower usage of plastic canisters).
A first step towards sustainability at the national level is to have management systems in place, whether in the form of voluntary systems, audit systems or international standards. One study that collected data from 210 dialysis units in Spain found that only 53 hospitals with dialysis (25%) and 11 outpatient centres had ISO14001 certification.36 Environmental commitment begins with the “eco-report”. With the aim of minimising the environmental footprint of HD, it is important to record and control referenced indicators of activities and their proper interpretation.
Reading indicators is complex and it must be taken into account that:
- •
Each indicator is independent: the water, light and waste readings cannot be mixed.
- •
Each indicator is specific to each centre. Each indicator must be read and interpreted on an individual basis, since each centre has its own specific characteristics.
- •
The aim of individual reading should be to maintain or decrease the value of the indicator.
- •
Values must be monitored periodically (half-yearly/annually). The monthly/annual value of the indicators is unlikely to always be a single value. If changes are detected, their origin must be investigated and measures implemented to correct them.
- •
The interpretation should not be directed at electricity and water usage or the generation of waste, but at the impact of this usage and expenses for each HD cycle in the centre.
Data corresponding to electricity and water usage indicators, in addition to waste generation, are shown below, which serve as illustrative examples of the methodology for reading and interpreting environmental indicators in an HD centre.
Fig. 3 shows the water usage indicator (litres per session) of an HD unit over six years. Stability is recorded over the years with minimal variations (Fig. 3A) and small monthly fluctuations (Fig. 3B) derived from various factors, such as leaks, additional purging requirements, variations in water quality that require a higher flow and additional usage not directly related to the HD process. However, since 2023 a significant increase has been detected, which requires analysing the causes and implementing improvement actions to minimise usage. This analysis has identified the cause to be an increase in the conductivity of the inlet water due to the drought, which requires a greater number of washes of the osmosis membranes, with the consequent increase in water usage to achieve the conductivity of less than 5 μS recommended by the HD water quality guides. This demonstrates the importance of monitoring indicators and promoting the responsible use of water in centres by applying the aforementioned measures.
 Average annual usage by litres/session/day. B) Monthly usage by litres/session.")
Fig. 4 shows the electricity usage indicator, which, like the water usage indicator, demonstrates stable results over the annual period (Fig. 4A). However, the monthly analysis (Fig. 4B) reveals a pronounced seasonality, with usage peaks in the summer months. This seasonality suggests a significant climatic influence on electricity usage, which can be remedied by improving the thermal insulation of buildings and optimising the efficiency of air conditioning systems. In addition, raising awareness on the prudent use of energy and air-conditioning could have a significant impact. This would include not leaving lights, computers and other appliances on standby unnecessarily, keeping doors closed and using screens to minimise the incidence of direct sunlight during peak usage months.
 Average annual usage by kWh/session/day. B) Monthly usage by kWh/session.")
Fig. 5 shows the annual indicator of medical waste generation where, unlike the previous two, there is a progressive increase from 2020 onwards. This could be explained improved record-keeping, or alternatively reflect the impact of the COVID pandemic with greater use of gloves and masks.
.")
In short, monitoring indicators provides us with an overview of our impact on the environment and their reading allows us to detect trends and deviations, and to act accordingly.
Carbon footprintIn addition to the usual indicators, nowadays there are accessible tools that can be used to estimate the carbon footprint generated by different human activities. On an international level, several countries have carried out a detailed analysis of the CO2 footprint of their centres, including England (more than a decade ago),7 Australia37 (a country dedicated to the implementation of sustainable processes), Japan38 and the USA.39,40
Life cycle assessment (LCA) is used to assess the impact of activities from the extraction of raw materials to manufacturing, transportation, use and recycling or disposal. It is a useful and widely accepted method for quantitatively evaluating the impact of processes and products on the environment, but given its measurement complexity, there are still not many studies in which it is used.41–43 As the prevalence of kidney disease is expected to increase over the coming decades, LCA results may help to find the balance between clinical practice and the economic and environmental costs of treatment.
What are the challenges for the future?Promoting home-based techniquesIn terms of economic and environmental sustainability, kidney transplant is currently the most sustainable renal replacement therapy (RRT) option,44 accounting for 54.45% of RRT patients in Spain according to data from the 2021 Dialysis and Transplant Report.45
A recent Italian study46 suggests that home HD methods (especially unassisted home HD) are a viable option with a lower environmental impact for subjects living in low population density areas where the transport of subjects and professionals has a high impact on CO2 emissions. However, there is considerable room for improvement for increasing the implementation of home-based techniques, and further research is needed to demonstrate that these techniques do indeed reduce the carbon footprint significantly compared to in-centre HD.
Involvement of professionals and organisationsIt is essential to raise awareness among professionals in order to minimise the environmental impact of healthcare activities. All medical societies and scientific organisations urgently need to undertake useful and long-lasting educational initiatives, where digital innovation opens the door to a more sustainable future.
Countries such as the United Kingdom and the Netherlands have already launched national initiatives. The European Renal Association-European Dialysis and Transplant Association (ERA-EDTA) has created a specific committee, the “Sustainable Nephrology Task Force”, whose aim is to raise awareness about sustainability and kidney disease, and has organised its 60τη congress as a hybrid event to reduce the impact of travel. It has also promoted Forestami, a project launched by local authorities to plant three million trees by 2030. The International Society of Nephrology has also launched its global initiative (Global Environmental Evolution in Nephrology and Kidney Care [GREEN-K]) with the aim of promoting sustainable and resilient renal care.47 In Spain, the carbon footprint was measured at the last two Spanish Society of Nephrology (SEN) congresses and the results showed a total scope of 97 tons of CO2 equivalents and 64.5 kg of CO2eq/participant at the Granada Congress (52nd edition, 2022).
Industry involvementIt is important to define activities that reduce environmental impact, such as waste packaging. When choosing new dialysis equipment or materials, their sustainability or the development of programmes to reduce, reuse and recycle materials must be considered.48
Economic cost of the measuresIn general, the measures adopted in HD to reduce environmental impact have an initial cost of investments, data analysis, etc., which is not always recovered. Even so, some of these measures may lead to at least a partial recovery of the initial cost in the medium-long term, such as, for example, the use of centralised systems instead of canisters for more efficient dialysis fluid consumption, improvements in air conditioning to reduce expenditure on energy usage, or appropriately sized water plants to optimises the cost of water usage. However, future studies that include an analysis of the economic impact of these measures are needed.
Dialysis tenders must take into account the reality of treatment and technology, updating requirements that have become obsolete and that may entail unnecessary costs, both economically and environmentally (e.g., requiring water plants with certain characteristics that are oversized with respect to the centre's needs). It would be interesting if dialysis tenders, in both the rates and their valuations, took into account the investment that an environmental improvement entails.
ConclusionsHD treatments consume a significant amount of resources (water and energy) and generate high levels of waste. Each centre needs to be aware of and analyse its indicators to fully understand its impact on the environment. This will enable them to set standards and implement improvement actions to achieve a greener and more sustainable HD.
Key concepts- •
Haemodialysis treatments consume a significant amount of resources (water and energy) and generate high quantities of waste.
- •
The main indicators that report on the impact of haemodialysis on the environment are: water usage (l/session), electricity usage (kWh/session) and waste generation (kg/session). These key indicators are supplemented by measuring the carbon footprint (kg CO2 equivalent).
- •
Each centre needs to be aware of and to analyse its indicators to understand its impact on the environment and propose individualised management strategies.
- •
Dialysis will always consume resources and generate emissions in proportion to the size of the activity, but it is always possible to focus actions towards a more environmentally friendly model.



