



Carers of peritoneal dialysis patients may suffer from burden, the characteristics of which differ from burden due to dementia, cancer or other dependent conditions.
AimsTo ascertain the reliability and validity of the Peritoneal Dialysis Carer Burden Questionnaire (PDCBQ), previously created, and to design the burden scale.
MethodsObservational, multicentre study of carers and patients on peritoneal dialysis for more than 3 months. Sociodemographic characteristics of patients and carers, patient dependency, perceived health (SF-36) and carer burden (Zarit scale) were recorded, as well as PDCBQ via 3 scales: dependence, subjective burden and objective burden.
ResultsOne hundred seven patients and their carers from 8 hospitals were evaluable. Carers were mainly women (83.2%), aged 57.50±14.69 years, and 36.4% worked out of the home. The internal consistency of the Zarit scale and the PDCBQ were high (Cronbach's α between 0.808 and 0.901). Significant correlation was found between the Zarit scale and PDCBQ (r=0.683). The concordance analysis between three degrees of Zarit scale and PDCBQ tertiles was good or acceptable (Kendall τ-b: 0.570, p<0.001). The exploratory factor analysis of the main factors revealed 3 factors, which were successfully correlated with the design of the PDCBQ. A new carer burden scale was designed.
ConclusionsThe study shows good reliability with high internal consistency of the PDCBQ. Factorial analysis shows good construct and good correlation, and acceptable concordance with the Zarit burden scale confirmed criterion validity. The questionnaire is suitable to be applied in clinical practice.
Los cuidadores de pacientes en diálisis peritoneal pueden sufrir sobrecarga con características diferentes de la derivada de demencia, cáncer u otras enfermedades dependientes.
ObjetivosAnalizar la fiabilidad y la validez del Cuestionario de Sobrecarga del Cuidador de Diálisis Peritoneal (CSCDP) elaborado anteriormente y establecer los baremos del mismo.
MétodosEstudio observacional, multicéntrico de cuidadores y pacientes con más de 3 meses en diálisis peritoneal. Se registraron: características sociodemográficas de pacientes y cuidadores, dependencia de pacientes, salud percibida (SF-36) y sobrecarga del cuidador (escala de Zarit), además del CSCDP con 3 escalas: dependencia, sobrecarga subjetiva y sobrecarga objetiva.
ResultadosFueron evaluables 107 cuidadores y pacientes de 8 hospitales. Los cuidadores fueron mayoritariamente mujeres (83,2%), con una edad media de 57,50±14,69 años; un 36,4% trabajaban fuera de casa. La consistencia interna de la escala de Zarit y del CSCDP fue elevada (α de Cronbach entre 0,808 y 0,901). La correlación entre la sobrecarga del Zarit y la del CSCDP fue significativa (r=0,683). La correspondencia entre 3 grados de sobrecarga del Zarit y los tertiles del CSCDP fue buena o aceptable (τ-b Kendall: 0,570, p<0,001). El análisis factorial exploratorio de componentes principales mostró 3 componentes coincidentes con el diseño del CSCDP. Se han elaborado los baremos de sobrecarga del cuidador.
ConclusionesEl estudio demuestra buena fiabilidad con elevada consistencia interna del cuestionario CSCDP. El análisis factorial denota validez de constructo y la buena correlación y aceptable correspondencia con la escala de Zarit indican validez de criterio. El cuestionario resulta apto para aplicación clínica.
Carers of patients receiving peritoneal dialysis (PD) or other chronic diseases can be at risk of work overload due to the burden of caring for and treating these dependent individuals.1–3
Overload is a key dimension in the evaluation of carers. Analysis of the variables affecting carers has led to the development of conceptual models that show overload to be caused by different factors and components.4–7 This is why it is so important to measure the degree of overload in this population.
Several studies conducted over the past 30 years have revealed significant degrees of carer overload in connection with different diseases, and have highlighted the need to design respite protocols for carers.8–12
The burden of carers of patients on renal replacement therapy with haemodialysis (HD), PD and kidney transplant has already been evaluated using questionnaires that address various different dimensions: health-related quality of life,1,2,13–15 emotional state,2,16,17 depression,14–18 vital satisfaction, family stress, marital relationship,19 psychosocial repercussion,13 exhaustion or burnout syndrome and, more specifically, subjective or objective caring-related personal overload.2,13,14,16,18,20
However, most studies have so far used general questionnaires to determine carer overload,1,2,14,16 even though generic measures may not be sensitive enough to identify differences, particularly in a research setting.21 Few studies have used questionnaires designed specifically for PD22,23 or HD plus PD.4
The characteristics of PD patients differ considerably from patients with dementia, cancer, or severe functional limitations, and, therefore, the stress factors affecting their carers also differ to a certain extent. Thus, some years ago our group developed the Overload Questionnaire for Carers of Patients on Peritoneal Dialysis (CSCDP, in its Spanish acronym). This instrument includes 3 dimensions: patient's degree of dependence, carer's subjective overload, and carer's objective overload, and has shown optimal reliability and validity for clinical use.24
Nevertheless, validation of health-related questionnaires or scales is an ongoing process, as the results and corresponding interpretation may vary depending on the specific characteristics of the population in which they are used.25
Questionnaires are validated on the basis of their reliability and validity. Reliability indicates the extent to which a measuring instrument produces accurate results on repeated tests. It is evaluated on the basis of internal consistency, stability over time, equivalence, and inter-observer agreement. Validity, meanwhile, shows the degree to which the instrument measures what it really intends to measure in terms of content, construct, and criteria.25–27
In this study, we have validated the CSCDP in a wider sample of carers using the 36-item short form (SF-36) health-related quality of life questionnaire28 and the Zarit Burden Interview (ZBI)29–32 to test the criterion validity. The ZBI has been translated into many languages, and is widely used and recommended.33–36 It has also been used for carers of patients with chronic kidney failure on replacement therapy with HD,13,17,37,38 PD1,2,17,22,23,38,39 and kidney transplant.16
The objectives of this study have been to validate the CSCDP by analysing the reliability (internal consistency) and validity (construct validity and criterion validity compared to the ZBI), and to construct a number of rating scales from the questionnaire to determine the degree of overload of the carers in our study sample.
Material and methodsAll patients included in a PD programme from 8 hospitals were invited to take part in the study. To be included in the study, the patient must have been receiving PD for at least 3 months, and must be cared for by a primary carer. The primary carer was defined as the person close to the patient who, when asked, confirmed that he/she is responsible for the care of the patient on PD. Both participants, patient and carer, were asked to sign an informed consent form before inclusion in the study. The study was approved by the ethics committee of the reference hospital (H. Universitari Germans Trias i Pujol, Badalona) and complies with the principles of good clinical practice.
Data collected from the patients included age, gender, education, work status, concurrent diseases, Charlson index, choice of treatment modality, and degree of independence when performing PD. The tests administered were: the Mini-Mental State Examination,40 the Karnofsky Performance Status scale,41 which assesses the patient's physical capacity and degree of independence, and the Lawton–Brody Instrumental Activities of Daily Living Scale.42 In the latter, we used the original 0–8-point score that measures the patient's degree of independence, and an alternative score developed by us that shows the degree of limitation resulting from not being able to perform the different activities, in order to correlate this with the degree of dependence. Health-related quality of life was assessed using the SF-36 questionnaire validated for the Spanish population.28,43
In the case of the carers, we recorded their personal characteristics and work status and the degree of kinship or relationship with the patient, and their score on the Mini-Mental State Examination, the SF-3628 and the 22-item ZBI29,30 adapted and revalidated for the Spanish population.31,32 In this questionnaire, answers were scored from 0 to 4 (never: 0; rarely: 1; sometimes 2; quite frequently; 3; nearly always: 4). Following the system used by many other authors,17,34,37 overload was classified into 4 different levels, according to the following scores: (1) from 0 to 20, slight overload or no overload; (2) from 21 to 40, mild to moderate overload; (3) from 41 to 60, moderate to severe overload, and (4) 61 or more, severe overload.
The CSCDP comprises 30 questions relating to 3 dimensions: patient dependence (8 items), subjective overload (12 items) and objective overload (10 items) of the PD carer.24 Unlike the previous study published by our group, each item is scored using a scale from 0 to 4, with 4 being the worst situation. These 2 tests were administered with an interval of between 15 and 30 days. The order was changed to avoid bias.
Statistical analysisFor the statistical analysis, one-way ANOVA and the Bonferroni post hoc test were used to compare means between groups, the Student's t-test for 2 groups, Cronbach's α for internal consistency, Pearson's correlation coefficient to compare scales, Kendall's τ-b coefficient for the correspondence analysis, multiple linear regression for the analysis of explanatory variables, and exploratory factor analysis of principal components.
ResultsOne hundred and sixteen patients and carers were included initially; of whom 9 were excluded because they did not complete the protocol, leaving 107 carers and patients from 8 hospitals for the final analysis.
The average age of patients was 63.49±13.29 years, and carers was 57.50±14.69 years; this difference was significant (p=0.002). The patients had been receiving PD for 24.07±19.15 months, with a Charlson comorbidity index of 7.05±2.71; 34.6% were diabetic and 49.5% were treated with a cycler. There were no significant differences between centres (ANOVA).
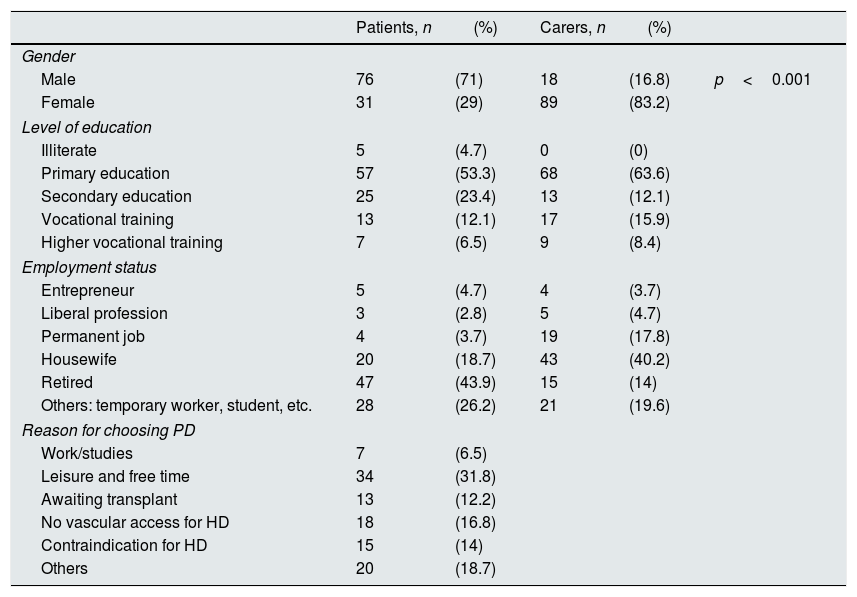
The majority of carers were women, while the patients were mostly men (p<0.001). Both carers and patients had a similar level of education. The work status of most patients was retired, and most carers were housewives.
PD had been prescribed by the patient's doctor in 35.5% of cases, and had been chosen by the patient or his/her family in 64.5% of cases; in 31.8% of these, it was chosen because it enabled them to pursue their leisure and free time activities (Table 1). Forty-three (40.2%) patients always needed help to perform PD, 14 (13.1%) needed help sometimes, and 50 (46.7%) never or hardly ever needed help.
Social and employment status of patients and carers.
| Patients, n | (%) | Carers, n | (%) | ||
|---|---|---|---|---|---|
| Gender | |||||
| Male | 76 | (71) | 18 | (16.8) | p<0.001 |
| Female | 31 | (29) | 89 | (83.2) | |
| Level of education | |||||
| Illiterate | 5 | (4.7) | 0 | (0) | |
| Primary education | 57 | (53.3) | 68 | (63.6) | |
| Secondary education | 25 | (23.4) | 13 | (12.1) | |
| Vocational training | 13 | (12.1) | 17 | (15.9) | |
| Higher vocational training | 7 | (6.5) | 9 | (8.4) | |
| Employment status | |||||
| Entrepreneur | 5 | (4.7) | 4 | (3.7) | |
| Liberal profession | 3 | (2.8) | 5 | (4.7) | |
| Permanent job | 4 | (3.7) | 19 | (17.8) | |
| Housewife | 20 | (18.7) | 43 | (40.2) | |
| Retired | 47 | (43.9) | 15 | (14) | |
| Others: temporary worker, student, etc. | 28 | (26.2) | 21 | (19.6) | |
| Reason for choosing PD | |||||
| Work/studies | 7 | (6.5) | |||
| Leisure and free time | 34 | (31.8) | |||
| Awaiting transplant | 13 | (12.2) | |||
| No vascular access for HD | 18 | (16.8) | |||
| Contraindication for HD | 15 | (14) | |||
| Others | 20 | (18.7) | |||
HD: haemodialysis; PD: peritoneal dialysis.
The relationship between carers and patients was: spouses 83 (77.6%), children 17 (15.9%), father or mother 5 (4.7%) and other 2 (1.8%). The carer had been caring for the patient for: less than 6 months – 11 (10.3%); between 6 months and 1 year – 27 (25.2%); between 1 and 2 years – 27 (25.2%); between 2 and 3 years – 18 (16.8%) and more than 3 years – 24 (22.4%). Twenty-five carers had a full-time job (23.4%), 14 (13.1%) worked part-time, and 68 (63.6%) did not work outside the home. Nearly all (92.5%) carers lived in the same house as the patient.
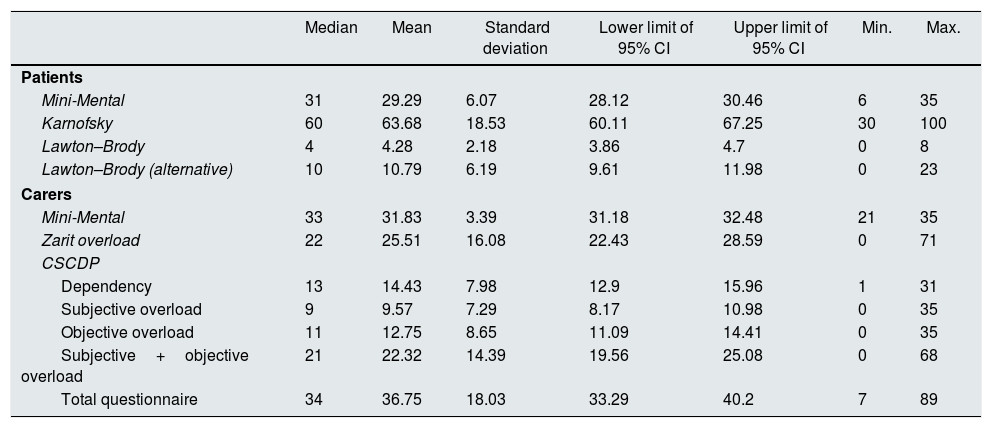
Results of the questionnaires administeredThe results of the descriptive statistics are shown in Table 2. In the Mini-Mental State Examination, patient scores were significantly lower than those of the carers (p<0.001). Eleven patients and 2 carers scored less than 23 points (cognitive impairment). The analysis by centres (ANOVA) found that the carers from centre 3 scored significantly lower on the Mini-Mental State Examination than those from centres 5 and 8 (Bonferroni: p=0.011).
Results of the questionnaires administered to patients and carers.
| Median | Mean | Standard deviation | Lower limit of 95% CI | Upper limit of 95% CI | Min. | Max. | |
|---|---|---|---|---|---|---|---|
| Patients | |||||||
| Mini-Mental | 31 | 29.29 | 6.07 | 28.12 | 30.46 | 6 | 35 |
| Karnofsky | 60 | 63.68 | 18.53 | 60.11 | 67.25 | 30 | 100 |
| Lawton–Brody | 4 | 4.28 | 2.18 | 3.86 | 4.7 | 0 | 8 |
| Lawton–Brody (alternative) | 10 | 10.79 | 6.19 | 9.61 | 11.98 | 0 | 23 |
| Carers | |||||||
| Mini-Mental | 33 | 31.83 | 3.39 | 31.18 | 32.48 | 21 | 35 |
| Zarit overload | 22 | 25.51 | 16.08 | 22.43 | 28.59 | 0 | 71 |
| CSCDP | |||||||
| Dependency | 13 | 14.43 | 7.98 | 12.9 | 15.96 | 1 | 31 |
| Subjective overload | 9 | 9.57 | 7.29 | 8.17 | 10.98 | 0 | 35 |
| Objective overload | 11 | 12.75 | 8.65 | 11.09 | 14.41 | 0 | 35 |
| Subjective+objective overload | 21 | 22.32 | 14.39 | 19.56 | 25.08 | 0 | 68 |
| Total questionnaire | 34 | 36.75 | 18.03 | 33.29 | 40.2 | 7 | 89 |
95% CI: 95% confidence interval; CSCDP: Overload Questionnaire for Carers of Patients on Peritoneal Dialysis.
On the Karnofsky scale, the median score was 60 and the average score was 63.67%, corresponding to the need for occasional help. The ANOVA by centres showed significant differences between centre 3 and centre 8 (post hoc, Bonferroni: p=0.002).
On the Lawton–Brody scale, the average score using the instrument's own system showed moderate dependence, and light-to-moderate dependence using our alternative system. The reliability of this scale was good (Cronbach's α 0.760) with the instrument's own system, and somewhat better (Cronbach's α 0.835) with our alternative system.
The health status of carers (SF-36) was better than that of patients in terms of physical function (p<0.001), physical role (p<0.001), general health (p<0.001) and vitality (p=0.02); there were no differences in bodily pain, social functioning, emotional role and mental health (Fig. 1).

SF-36 Health Questionnaire. The statistical evaluation is given in the text. BP: bodily pain; ER: emotional role; GH: general health; M. 55–64: general population of men aged between 55 and 64 years; MH: mental health; PF: physical functioning; PR: physical role; SF: social functioning; VT: vitality; W. 55–64: general population of women aged between 55 and 64 years.
The health of the patients (mostly men) was significantly worse than that of men in the general population aged between 55 and 6443 in all dimensions (p<0.001). The carers (mostly women) showed worse health status in terms of their physical role (p=0.023), bodily pain (p=0.036), social functioning (p<0.001) and emotional role (p=0.011) than women in the general population aged between 55 and 6443 (Fig. 1).
Overload Questionnaire for Carers of Patients on Peritoneal DialysisThe results of the CSCDP, and the wide range between minimum and maximum scores, are shown in Table 2. The reliability of the questionnaire was excellent, with high internal consistency (Cronbach's α) in each dimension: dependence (α 0.808), subjective overload (α 0.812), objective overload (α 0.868) and total score (α 0.887).
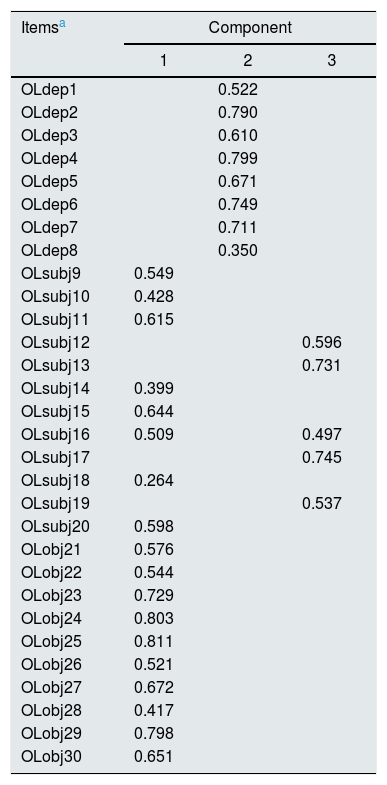
Factor analysis initially showed 8 factors with an eigenvalue greater than 1, which explained the 67.6% of total variance. On the basis of the Scree plot (Fig. 2) we chose the first 3 factors which explained the 45.7% of variance (Table 3). Component 1 showed high factorial loading on objective overload items (items 21–30; r=0.417–0.811) and on 8 of the 12 items of the subjective overload dimension of the CSCDP (r=0.264–0.644). Component 2 only showed high factorial loading on items of the dependency dimension (items 1–8) of the CSCDP (r=0.350–0.799). Component 3 showed high factorial loading on 5 items of the subjective overload dimension (r=0.497–0.745).

Rotated component matrix of the Overload Questionnaire for Carers of Patients on Peritoneal Dialysis.
| Itemsa | Component | ||
|---|---|---|---|
| 1 | 2 | 3 | |
| OLdep1 | 0.522 | ||
| OLdep2 | 0.790 | ||
| OLdep3 | 0.610 | ||
| OLdep4 | 0.799 | ||
| OLdep5 | 0.671 | ||
| OLdep6 | 0.749 | ||
| OLdep7 | 0.711 | ||
| OLdep8 | 0.350 | ||
| OLsubj9 | 0.549 | ||
| OLsubj10 | 0.428 | ||
| OLsubj11 | 0.615 | ||
| OLsubj12 | 0.596 | ||
| OLsubj13 | 0.731 | ||
| OLsubj14 | 0.399 | ||
| OLsubj15 | 0.644 | ||
| OLsubj16 | 0.509 | 0.497 | |
| OLsubj17 | 0.745 | ||
| OLsubj18 | 0.264 | ||
| OLsubj19 | 0.537 | ||
| OLsubj20 | 0.598 | ||
| OLobj21 | 0.576 | ||
| OLobj22 | 0.544 | ||
| OLobj23 | 0.729 | ||
| OLobj24 | 0.803 | ||
| OLobj25 | 0.811 | ||
| OLobj26 | 0.521 | ||
| OLobj27 | 0.672 | ||
| OLobj28 | 0.417 | ||
| OLobj29 | 0.798 | ||
| OLobj30 | 0.651 | ||
The ZBI showed a median of 22 and an average of 25.51±16.08 points, which indicates a slight-to-moderate overload on average among carers, with a wide range between minimum and maximum scores (0–71) (Table 2). Carers with overload: (1) slight or no overload (0–20): 48 (44.9%) carers; (2) mild to moderate (21–40): 39 (36.4%) carers; (3) moderate to severe (41–60): 17 (15.9%) carers, and (4) severe (61 or more): 3 (2.8%) carers. The reliability of the scale was excellent (Cronbach's α 0.901).
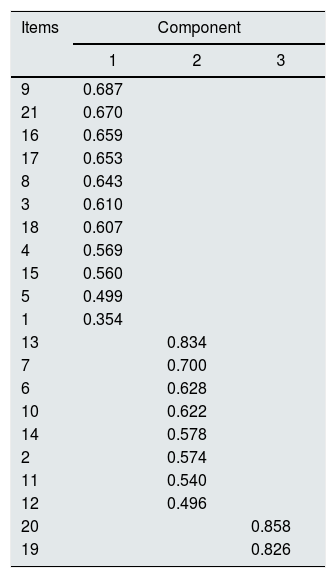
Exploratory factor analysis of the principal components using the Kaiser KMO test (0.873) and the Bartlett sphericity test (χ2=1035.22; p<0.001) showed that the data were adequate for the purpose. The first 3 components explained 53.32% of the total variance, and the Scree plot showed that these were the most relevant (Table 4) and were therefore compared with the components of the CSCDP.
Correlation between the Overload Questionnaire for Carers of Patients on Peritoneal Dialysis and the Zarit Burden InterviewThe Pearson correlation test showed that ZBI scores correlated well with the total score of the questionnaire (r=0.683), the subjective overload (r=602) and objective overload (r=631), and poorly with patient dependence (r=0.308), with a high level of statistical significance in all correlations (p<0.001).
In the exploratory factor analysis of principal components, component 1 of the ZBI showed poor correlation with the CSCDP dependence dimension (r=0.276; p=0.004) and good correlation with the subjective overload (r=0.619; p<0.001) and objective overload (r=0.599; p<0.001) dimensions. Similarly, component 2 of the ZBI showed poor correlation with the CSCDP dependence dimension (r=0.320; p=0.001) and good correlation with the subjective overload (r=0.505; p<0.001) and objective overload (r=603; p<0.001) dimensions. In contrast, component 3 of the ZBI showed no correlation with the CSCDP dimensions.
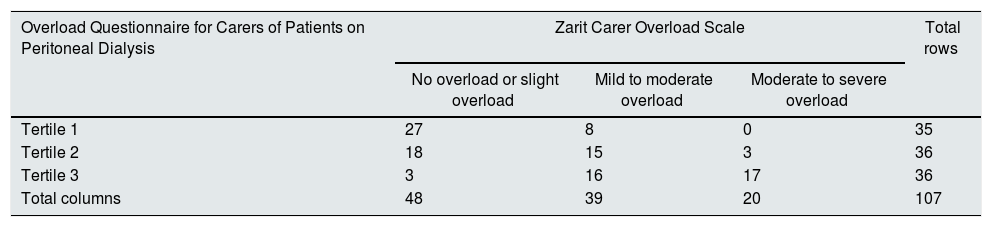
ZBI results were reduced to 3 levels for the purpose of correspondence analysis, grouping 3 and 4 into 3, as moderate and severe overload. The CSCDP dimensions were divided into tertiles. Correspondence between the 3 grouped levels of the ZBI and the tertiles of the CSCDP score was acceptable with the total score (Kendall's τ-b 0.570), the objective overload (Kendall's τ-b 0.650) and subjective overload (Kendall's τ-b 0.450) dimensions, and poor with the dependence dimension (Kendall's τ-b 0.247) (all with p<0.004) (Table 5).
Correspondence between the Overload Questionnaire for Carers of Patients on Peritoneal Dialysis and the Zarit Burden Interview.
| Overload Questionnaire for Carers of Patients on Peritoneal Dialysis | Zarit Carer Overload Scale | Total rows | ||
|---|---|---|---|---|
| No overload or slight overload | Mild to moderate overload | Moderate to severe overload | ||
| Tertile 1 | 27 | 8 | 0 | 35 |
| Tertile 2 | 18 | 15 | 3 | 36 |
| Tertile 3 | 3 | 16 | 17 | 36 |
| Total columns | 48 | 39 | 20 | 107 |
Data presented as number of cases per cell.
Statistical test: Kendall's τ-b: 0.570; p<0.001.
In all the dimensions of the SF-36, the health status of patients showed significant inverse correlations (r=−0.213 to −0.636; p<0.030) with the dependence dimension of the CSCDP, but no correlation with the carer subjective or objective overload dimensions. The health status of carers showed no correlation with the CSCDP dependency dimension, but significant inverse correlations were observed (r=−0.208 to −0.416; p<0.036) between almost all dimensions of the SF-36 and the CSCDP subjective and objective overload dimensions.
ComparisonsIn the ZBI and the CSCDP, no significant difference was observed between carers of patients treated with continuous ambulatory PD or with automated PD (cyclers), or between carers who do or do not work outside the home. The carers of patients who needed help to perform PD had significantly higher scores in dependence (19.02±7.20 vs. 9.20±5.11; p<0.001) and total scores (43.11±18.87 vs. 29.50±13.98; p<0.001), but not in carer subjective or objective overload.
On the ZBI test, carers who had been caring for the patient for more than 2 years scored significantly higher than those who had been caring for less than 2 years (30.95±16.65 vs. 22.27±14.92; p<0.008), whereas in the CSCDP this difference was not statistically significant (p=0.069).
Explanatory variablesThe multiple linear regression analysis showed that the Lawton–Brody scale was a significant explanatory variable for dependence, subjective, objective and total overload, and also for the ZBI. The Karnofsky scale was significant for dependence.
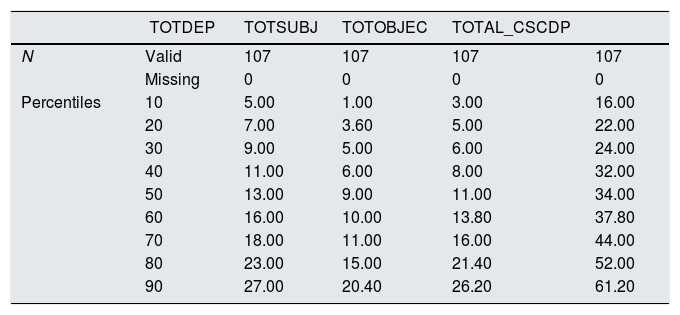
Sample data were used to construct the percentiles of each CSCDP dimension (Table 6) and cut-off points were established for the 3 degrees of CSCDP overload determined by tertiles (Table 7).
Percentiles of the Overload Questionnaire for Carers of Patients on Peritoneal Dialysis.
| TOTDEP | TOTSUBJ | TOTOBJEC | TOTAL_CSCDP | ||
|---|---|---|---|---|---|
| N | Valid | 107 | 107 | 107 | 107 |
| Missing | 0 | 0 | 0 | 0 | |
| Percentiles | 10 | 5.00 | 1.00 | 3.00 | 16.00 |
| 20 | 7.00 | 3.60 | 5.00 | 22.00 | |
| 30 | 9.00 | 5.00 | 6.00 | 24.00 | |
| 40 | 11.00 | 6.00 | 8.00 | 32.00 | |
| 50 | 13.00 | 9.00 | 11.00 | 34.00 | |
| 60 | 16.00 | 10.00 | 13.80 | 37.80 | |
| 70 | 18.00 | 11.00 | 16.00 | 44.00 | |
| 80 | 23.00 | 15.00 | 21.40 | 52.00 | |
| 90 | 27.00 | 20.40 | 26.20 | 61.20 |
TOTAL_CSCDP: total questionnaire score; TOTDEP: dependency; TOTOBJEC: objective overload; TOTSUBJ: subjective overload.
Table populated with the questionnaire scores. Items rated from 0 to 4.
Cut-off points for 3 overload levels of the Overload Questionnaire for Carers of Patients on Peritoneal Dialysis.
| Degree of overload | Degree of dependency | Subjective overload | Objective overload | Total questionnaire |
|---|---|---|---|---|
| Slight or none | 1–9 | 1–5 | 1–7 | 1–25 |
| Mild to moderate | 10–17 | 6–11 | 8–15 | 26–40 |
| Moderate to severe | 18 or more | 12 or more | 16 or more | 41 or more |
Based on the questionnaire score. Each item rated from 0 to 4.
This study, carried out on 107 PD patients and their carers, confirms the results obtained in our previous paper in which the CSCDP was developed.24 It shows that the scale has excellent reliability and good validity, and can determine the rating scales and cut-off points for different degrees of carer overload. The sample of patients obtained from 8 hospitals with ongoing PD programmes supports the value of our results.
Carmona Moriel et al.22 applied our questionnaire to 18 carers of PD patients using a 1–5 rating scale. They reported an average overload score of 41.89±14.93; if we had scored the items from 1 to 5, we would have obtained a similar average of 44.27±14.35 points for overload. These results indicate that the CSCDP obtains similar results in an independent sample.
The reliability of the questionnaire is confirmed, insofar as in the high internal consistency of the 3 definitive dimensions used in the first validation study24 (Cronbach's α 0.86–0.89) has been reproduced in this new sample (Cronbach's α 0.887). Similarly, the acceptable results of the limited test-retest reported in our previous study shows the stability of the questionnaire over time.
Content validity was already evaluated by our group during development of the questionnaire by eliminating items that were not consistent with the purpose of the questionnaire.24
The exploratory factor analysis of the main components of the CSCDP reveals some interesting information with regard to construct validity. Component 2 correlates solely with patient dependency items, while component 1 correlates with all the objective or repercussion overload items, which is consistent with the design of the questionnaire. In contrast, subjective overload correlates with components 1 and 3, suggesting that some items in this dimension are perceived by the carers as an objective overload or as something with repercussions on their life, while the items that correlate with component 3 should relate to the carer's personal perception of caring for or helping the patient. Either way, the 2 overload dimensions measure the carer's perception of their relationship with the patient in respect of aspects that impact on the life and on the most personal feelings of the carer, which we conceive as overload. Moreover, the dependency dimension is well delimited and differentiated from the other 2 dimensions, all of which confirms the construct validity of the questionnaire.
To test the criterion validity, we compared the CSCDP with two similar questionnaires: the ZBI29,30 and the SF-36.28
The ZBI, widely used internationally33–37 and translated and validated in Spanish,31,32 consists of 22 items to evaluate the carer's overload. Items are rated from 0 to 4 in the English versions and in some Spanish versions13,22,32 and from 1 to 5 in other Spanish versions, including the validated version.31,32 The results of this scale vary considerably, depending on the rating system used and the population studied.
The score awarded to the items (0–4 or 1–5) will determine the cut-off points for different degrees of overload. The version in English and languages other than Spanish, with 22 items and a rating scale of 0–4, considers 4 levels of overload (see the methods section), but is only an approximation, since the results vary greatly depending on the population studied or the patients’ diseases.17,34,37 In the validated Spanish version with a 1 to 5 rating scale, 3 degrees of overload were determined with 2 cut-off points: no overload-slight overload 46/47, mild overload-severe overload 55/56.31 In a subsequent study, the cut-off points were re-set to 56/57 and 59/60, respectively, relative to a general health status questionnaire.32 Most Spanish studies, even those using the 0–4 rating scale22,38 or the 21-item ZBI44 use this classification; the resulting confusion has been described by Álvarez et al.45
It is interesting to note that studies published in English have reported the wide range of mean scores, from 22.40 to 39.10, obtained when applying the ZBI in diseases such as cancer, dementia and acquired brain injury.34,46 Likewise, in studies on carers of patients with PD, or PD vs. HD, the average scores range from 20.4 to 43.75, with no significant differences between the 2 treatments,2,13,14,37 although a Japanese study reported surprisingly low scores of between 12.5 and 14.1 points in PD.39
In our subjects, the ZBI and CSCDP showed good correlation (r=0.683). This was confirmed in the overload dimensions, and is further evidence of criterion validity. Carmona Moriel et al. confirmed the very good correlation (r=0.875; p=0.000) between both questionnaires administered in the same visit.22 In our study, however, they were separated by at least 15 days, and were not administered in the same order, which may explain in part the different degree of correlation. This good correlation confirms the criterion validity of the CSCDP.
The analysis of correspondence between the 3 (grouped) levels of overload of the ZBI and the tertiles of the CSCDP shows acceptable, though not excellent, levels of correspondence (Kendall's τ-b 0.570; p<0.001). This could be due to several factors: (1) changes in the carer's perception of overload in the time elapsed between the 2 questionnaires; however, the conditions that can lead to overload in the PD carer do not change in that 15–30 day period, so any perceived change would be minor; (2) the established degrees of overload do not correspond entirely; (3) the 2 instruments do not measure the same type of overload; for example, the dependency dimension of the CSCDP has very little correlation with the ZBI, and the exploratory factor analysis of the main components of the ZBI shows that 1 of the first 3 has no correlation at all with the CSCDP. When different scales measure different types of overload, this can affect the correspondence between different degrees used in the scales, and highlights the need to use questionnaires designed specifically for PD.
The SF-36 Health QuestionnaireUnsurprisingly, the patients’ perceived physical functioning, physical role, general health and vitality was worse than their carers, a finding also reported by other authors.1,39 In addition, the health status of our patients was significantly worse in all dimensions than in the corresponding population group.43 In contrast, carers (mostly women) scored worse in physical role, bodily pain, social functioning and emotional role than the corresponding population group.43
It is striking that in the CSCDP, dependency only correlated with the patients’ health but not with the carers’ overload, while the carers’ subjective and objective overload correlated significantly with the health of the carers themselves – a correlation already reported by other authors.13,37 In addition, in the CSCDP, carers of patients who needed help to perform PD and who, therefore, are more dependent scored higher in dependency, but not in subjective or objective overload. This means that, as shown in our previous study,24 carers perceive the patient's health problems and dependency, including performing the PD, to be separate from their overload which, in contrast, they perceive as being affected by their own state of health.
ScalesTable 7 shows the cut-off points for the 3 levels of dependency and overload in CSCDP scores (0–4 rating scale), based on their correspondence with the ZBI classification. Although these rating scales have not been finalised, they can already be used in clinical practice.
Overload among the carers of patients with various diseases has led to the introduction of respite programmes. Although these programmes are highly rated by carers, they provide little solid evidence, and further studies with better defined objectives are needed before firm conclusions can be drawn.8–12
Limitations of the studyUnlike other studies on specific diseases, we did not determine cut-off points for depression or other borderline situations of carers.35 Such data would be important when planning respite programmes for overburdened carers.
In summary, this study has re-confirmed the internal consistency reliability of the CSCDP. Factor analysis has shown the questionnaire to have good construct validity and good correlation, using the ZBI as a benchmark of general carer overload. This corroborates the criterion validity of the questionnaire.
The correspondence between the degrees of overload measured in these 2 instruments was only good or acceptable. This suggests that they do not measure the same type or intensity of overload, and could support the effectiveness of the questionnaire as a specific instrument for this patient population.
We found mild to moderate degrees of overload in our sample, with quite a wide range of scores. This is largely consistent with studies on general carer overload, and on dialysis carers.
The rating scale questions of the CSCDP can be used in clinical practice to differentiate the degrees of dependence or overload presented by carers of PD patients.
Conflicts of interestThe authors declare that they have no conflicts of interest concerning the preparation and publication of this article.
For their contribution, which was necessary to carry out the study: C. Bermúdez, Ana Rodriguez Carmona, Miguel Perez Fontan, from H. Juan Canalejo, A Coruña; Dolores Carreras, Mercé Borras, from H. Arnau de Vilanova, Lleida; Olga Celadilla, Gloria del Peso, Auxiliadora Bajo, Rafael Selgas, from H. La Paz, Madrid; Paquita Gruart, Maria Teresa Gonzalez, from H. de Bellvitge, L’Hospitalet de Llobregat; Conchita Blasco, Esther Ponz, from Consorci Hospitalari del Parc Taulí, Sabadell; Ester Vilaplana, from H. de la Vall d’Hebron, Barcelona; Antonio Morey, from H. Son Dureta, Palma de Mallorca.
Please cite this article as: Teixidó-Planas J, Tarrats Velasco L, Arias Suárez N, Cosculluela Mas A. Sobrecarga de los cuidadores de pacientes de diálisis peritoneal. Validación de cuestionario y baremos. Nefrologia. 2018;38:535–544.



