












Introducción: La supervivencia entre la hemodiálisis (HD) y la diálisis peritoneal (DP) son equivalentes, siendo los factores de comorbilidad asociados los que ejercen más influencia sobre la mortalidad. En los más recientes estudios, el pronóstico de la DP peritoneal ha mejorado proporcionalmente más que el de la HD, aunque esto no ha significado un aumento en la utilización de este tratamiento. Objetivos: Conocer si la DP en nuestro medio ha mejorado en el tiempo con respecto a sus resultados. Conocer la influencia de la comorbilidad y las características del tratamiento en los resultados finales. Métodos: Pacientes incidentes en DP en Andalucía entre 1999 y 2010. La cohorte se ha dividido en dos grupos: antes y después de 2004. Estadística: medias ± desviación estándar, frecuencias, test de χ2, t de Student, determinación de riesgos (con intervalo de confianza al 95%), Kaplan-Meyer, log-rank y modelo multivariante de riesgo proporcional de Cox. Resultados: 1464 pacientes incidentes en DP, 537 antes de 2004 y 927 posterior a 2004. Las características basales de ambos grupos (edad, diabetes) eran similares, si bien el primer grupo presentaba más enfermedad cardiovascular y comorbilidad medida por Charlson. En el segundo período se usó más DP automática y soluciones de bicarbonato e icodextrina. La supervivencia global de los pacientes fue 55 meses de mediana y 65 de media. En todos los subgrupos (edad, diabetes, enfermedad cardiovascular, tipo de técnica, diabetes) existe una mejor tendencia para la supervivencia en el segundo período (con significación para tipos de técnica, edad y diabéticos). Fueron factores independientes de riesgo la edad, la enfermedad cardiovascular, la diabetes mellitus y ser incidente antes de 2004. Esta última variable pierde significación cuando se incluyen las soluciones de bicarbonato e icodextrina, que sí se muestran como factores independientes de riesgo. La supervivencia de la técnica mostró una mediana de 68 meses y una media de 73 meses. Fueron factores independientes de riesgo para la técnica las soluciones de diálisis y el período de inicio de DP. Conclusiones: La DP ha mejorado sus resultados en los últimos años; probablemente las nuevas soluciones están influyendo positivamente. Por tanto, debería implementarse su uso a través de criterios de eficacia, libre elección, eficiencia, y desarrollarse plenamente las unidades de DP en los Servicios de Nefrología.
Introduction: Survival rates between haemodialysis (HD) and peritoneal dialysis (PD) are the same but the associated comorbidity factors have a great impact on mortality. In the most recent studies the prognosis for PD has improved more than that for HD, although this has not meant an increase in the use of this treatment. Objectives: To determine whether the PD has improved over time with respect to its outcomes in our community, and determine the influence of comorbidity and treatment characteristics on the final results. Methods: Incident patients undergoing DP in Andalusia between 1999 and 2010. The cohort was divided into two groups: before and after 2004. Statistics: mean ± standard deviation, frequency, chi-square test, Student's t-test, risk determination (95% confidence interval), Kaplan-Meyer, log-rank and multivariate Cox proportional hazards models. Results: 1464 incident patients undergoing DP, 537 before 2004 and 927 after 2004. The baseline characteristics of both groups (age, diabetes) were similar, although the first group had more severe cardiovascular disease and higher Charlson comorbidity index. In the second period, more automatic PD and solutions of bicarbonate and icodextrin were used. The overall survival rate for patients was 55 months median and 65 mean. Within all subgroups (age, diabetes, cardiovascular disease, technique type) there was a greater tendency towards survival in the second period (the technique type, age and diabetes were found to be statistically significant variables). Age, cardiovascular disease, diabetes mellitus and incident cases before 2004 were all independent risk factors. This latter variable lost significance as bicarbonate or icodextrin-based solutions were introduced, which were independent risk factors. Technique survival showed a median of 68 months and a mean of 73 months. Dialysis solutions and the period when the DP was initiated were independent risk factors for the technique. Conclusions: DP has shown improved results in recent years; probably the new solutions are having a positive influence. As such PD should be implemented applying the criteria of effectiveness, free choice, efficiency and PD units should be fully developed within Nephrology Departments.
INTRODUCTION AND OBJECTIVES
As it is well known through the latest publications and comparative analysis, survival rate between haemodialysis (HD) and peritoneal dialysis (PD) techniques are the same, with similar long-term results, but the associated comorbidity factors have a great impact on the mortality rates of dialysis patients.1-3 Advanced age, diabetes mellitus and complications arising from arteriosclerosis seem to be definitive influencing factors and may explain with a wide enough margin most deaths in the multivariate models, therefore, having more connection with survival rate than with dialysis itself.4,5
However, PD is used much less than it would be expected on the light of such publications.6 Medical and, what is more concerning, non-medical factors, such as financing and knowledge and experience of each medical unit or centre, may have influenced this matter. Nonetheless, in the most recent studies prognosis for PD has improved proportionately more than that of HD,7-9 yet this has not meant an increase in the usage of this treatment.
The primary objective of the present study focuses, therefore, in determining whether PD has improved over time, within our environment, with respect to results in both patient survival and technique during two study periods: before and after 2004.
As secondary objectives, we will describe basic characteristics of patients in both periods, associated comorbidity and technical characteristics of the treatment. We will also determine how these factors have influenced the results at the end of the follow-up period.
PATIENTS AND METHODS
This is a cohort study conducted in 1464 patients diagnosed with stage V chronic kidney disease and currently on PD technique in the Autonomous Community of Andalusia between 1 January 1999 and 31 December 2010. Children under the age of 14 have been excluded.
The cohort has been divided into two periods, before and after 1 January, 2004, the turning point was established by the introduction of more biocompatible solutions with bicarbonate and icodextrin. These comparative studies will be conducted between the two groups in terms of initial comorbidity, patient survival and technique survival.
All the information comes from Andalusia's Transplants Coordination Authority information system database (Andalusian Regional Ministry of Health). For the present study, we have collected various demographic variables, (such as sex and age at the start of technique treatment), aetiology of kidney disease, technique aspects, (such as automated PD (APD) or continuous ambulatory PD), type of solutions (lactate or bicarbonate with low glucose degradation products [GDP], icodextrin), implant technique and type of catheter, comorbidity at the beginning, Charlson index, average time spent in the technique, state at the end of follow-up (deceased, transplanted, transferred to HD or remains alive on technique) and cause of death if it occurred.
The statistical analysis was carried out using central tendency and dispersion measures (mean ± standard deviation) for quantitative variables, and frequencies for qualitative variables; for inferential statistics, the comparison of data using χ2 tests and Student's t-tests according to variable type, risk determination and 95% confidence intervals, survival curves and Kaplan-Meyer log-rank test for curve comparison. For the multivariate analysis, we used the Cox proportional hazards model.
RESULTS
Patient characteristics
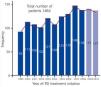
The study has 1464 patients in PD (as of 31 December 2010 there were 352 patients in the programme). Mean age: 55±17 years, 40% of patients in their 60s, 70s and 80s. Sex: Male: 57%. Female: 43%. Mean permanence: 22±21 months. The most prevalent initial kidney diseases were diabetic nephropathy and glomerular pathology. Annual incidence rate is shown in Figure 1.
Comparative data between both groups (incident patients before and after 2004)
The baseline characteristics of patients (Table 1) between the two groups are quite similar, with similar average age, similar percentages of patients older than 55 and 70 years, as well as almost identical percentages of diabetic patients. There were, however, significant differences in cardiovascular comorbidity, as reflected in the Charlson index difference. In the analysis of the Charlson categories, we note that there were no changes with respect to the groups of medium risk (Charlson index: 4-6), but there was a significant decrease of comorbid patients (Charlson index: ≥ 7) as well as an increase in patients with less comorbidity (Charlson index ≤ 3) on the second period studied.
The most prevalent aetiologies of initial kidney disease did not show significant differences between the two periods, diabetic nephropathy and glomerular diseases stand out as the most important ones, although they switch first and second position in each period.
Baseline technical aspects: Table 2 presents the different PD techniques used among the groups. We must emphasize a more progressive use of APD since 51% of patients in the second period used this modality, with statistical difference when compared to the first period (34.5%). Similarly, more icodextrin solutions and solutions with bicarbonate and low GDP are used.
In recent years (second period) percutaneous techniques for the implementation of catheter have significantly increased, which may be interpreted as a greater autonomy of nephrology equipment for PD.
We have carried out a comparative analysis by periods (Table 3) of the three major causes of patient release from PD programme (death, transplant and transfer to HD). For this purpose, we matched the follow-up time in both periods to 60 months. We observed that for the same time, the percentage of total releases in the period previous to 2004 is 87.5% at 5 years, higher than 61.2% outputs for incident patients after 2004. There is a declining trend of release by death (41.3% versus 27.6%), as well as an increase of release by transplant (30.6% versus 37.3%) and by transfer to HD (28.1% versus 35.1%). These differences are statistically significant.
The causes of death are similar in both periods, cardiovascular death being the most prominent.
Analysis of patient’s survival
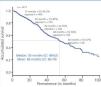
The overall patient’s survival on PD technique in Andalusia in the period 1999-2010 had a median of 55 months and an average of 65 months (Figure 2).
The main risk factors for patient survival at the beginning of technique were: age, diabetes mellitus, cardiovascular disease, the type of PD technique (APD or CAPD) and the initial time of treatment (pre- or post- 2004), as shown in Figure 3.
When analysing the influence of the factors mentioned on survival, stratifying it by periods (before or after 2004), we observed that in all subgroups there was a better trend for survival in the second time period; reaching statistical significance in the subgroups of any type of technique, any age group and non-diabetic patients (Table 4).
We used Cox regression to assess the independence of the different risk factors and their influence on survival. The following factors were significant: (a) age (treated as a continuous variable), (b) cardiovascular disease, c) diabetes mellitus and d) being an incident patient during the first time period studied (prior to 2004) (Table 5).
Influence of new solutions on patient survival
In the studied population we have been able to show how significantly those patients treated with bicarbonate and low GDP and with icodextrin, at some point in their evolution showed better survival compared to those who used other types of solutions, as seen in Figure 4.
Until now we have seen that certain factors influence patient survival, such as diabetes, cardiovascular disease, age, type of PD technique, as well as the start period of technique. We just saw how the employment of new solutions also makes a difference in survival. But, are all these independent factors, or are they perhaps related? To answer this question we have built the following multivariate model (Table 6), where we observe that once solutions are introduced to the equation, the influence that time period held over survival loses significance.
Analysis of technique survival
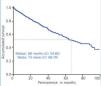
The overall survival of patients on PD technique in Andalusia in the period 1999-2010 had a median of 68 months and an average of 73 months (Figure 5).
Among the factors that influence the most in the overall technique survival we find, again, the use of new bicarbonate and icodextrin solutions (Figure 6).
And as with the parallel analysis of patient survival, in the case of technique survival we also want to know which of these factors influence independently, through a multivariate Cox regression. The use of icodextrin and bicarbonate are shown as independent factors, as well as the start period of PD, which did not lose its statistical significance in this analysis (Table 7).
DISCUSSION
In spite of the fact that therapeutic equivalence between PD and HD has been demonstrated, in Spain, and in recent years, we've seen only a minimal increase in the use of the first, carried on with variability among different communities and centres.10,11
However, for some time now, there are many publications that have demonstrated this therapeutic equivalence12 or even considered PD better than HD for certain groups of patients or in the initial period of renal replacement therapy.13-15
Along this line we proposed to study how the population treated with PD had behaved in Andalusia with respect to patient survival and technique during a long follow-up period of 12 years. As a response to the primary objective of our study and in light of the above results, we can state that PD within our environment has improved over time with respect to its results, both in patient survival and technique, during the most recent period.
There are several factors that influence this better prognosis. On patient survival, comorbid factors, such as diabetes, cardiovascular disease or age of the patient, have a great deal of influence at the beginning of the technique, but also, and in a very important way, the type of technique used (APD or CAPD) and the usage of the new solutions, more biocompatible and with less glucose concentration as osmotic agent. So much so, that the best results of the second period studied are clearly more conditioned by the increased use of these solutions over the last few years than by the time period itself, as other authors have reported.16,17
It seems that there are several points where the new solutions impact these results. When it comes to bicameral solutions with bicarbonate18: in the first place, the suppression of GDP during manufacturing and storage of bags; secondly, the reduction of exposure to glucose, and, finally, the use of a more physiological buffer, such as bicarbonate. And as to the impact of solutions of icodextrin: on the one hand, through the reduction of exposure to glucose with this alternative osmotic agent. And on the other hand as a strategy for patients over hydrated due to insufficient peritoneal ultrafiltration, especially patients with hyperpermeable peritoneum indicated as temporary or permanent, or in long episodes (both in CAPD as in APD)19 .
Similarly, technique survival improved in the second period studied. This being an independent factor because in addition to the better protection of the peritoneal membrane due to the use of more biocompatible solutions (which proved to be independent factors as well), the technique experience accumulated, the better selection of PD patients in medical centres, more appropriate dialysis doses, better handling of the volume and more adequate treatment of complications such as peritonitis might have influenced the results.20, 21
We may finally conclude that PD, both within our environment and in general, has improved its performance in the last few years, unlike that of HD, which has remained stable.7And that the new solutions play an important role in these better results, because they affect both in better technique prognosis, probably through minimising disruptions of the membrane and infections, as well as in a better patient prognosis through a proper balance of fluids for maintaining ultrafiltration and the reduction of systemic inflammatory effects.22 Since data for our study was collected from medical records, it is not possible to account for all prognostic factors that might have weight in the evaluation of risks, like factors of inflammation-malnutrition, etc. , and also in non-randomized populations there is always a residual adjustment not measured that may have limited the accuracy of results.
For all these reason, and in light of the current results, we can make our own assertion that the effectiveness of PD versus that of HD cannot be postulated as a discriminating feature. And that the low level of use of the first as renal substitute treatment in Spain, as well as in other countries, is conditioned by non-medical criteria, and therefore its use should be implemented through criteria of free choice, efficiency23 and development of PD units in nephrology departments.24
Conflicts of interest
The authors affirm that they have no conflicts of interest related to the contents of this article.

Figure 1. Incident patients in peritoneal dialysis per year

Figure 2. Overall curve of patient survival, 1999-2010 period

Figure 3. Influence of risk factors in patient survival (log-rank)

Figure 4. Influence of new solutions (bicarbonate and icodextrine) on patient survival (log-rank)

Figure 5. Overall technique&

Figure 6. Influence of new solutions on technique survival (log-rank)

Table 1. Baseline characteristics

Table 2. Technical aspects of peritoneal dialysis per time period

Table 3. Causes of release from peritoneal dialysis technique and causes of death

Table 4. Survival rate stratified by risk factors and time period

Table 5. Multivariate study: Cox proportional hazards models

Table 6. Multivariate study: Cox proportional hazard models

Table 7. Technique&



