
The success of cancer treatment implies the need to use diagnostic procedures, as well as therapeutic agents—not exempt from nephrotoxicity—which may lead to the development of chronic kidney disease (CKD) in patients who survive cancer. Furthermore, it is known that patients on dialysis and who have had kidney transplants have a greater risk of developing cancers; however, the association between CKD and cancer is more contested. These arguments are only some of those for which studies in the area of Onco-nephrology are becoming increasingly important.1,2 Regarding the review by Francisco et al. about onco-nephrology, which argues for the creation of a new working group within the Sociedad Española de Nefrología [Spanish Society of Nephrology] and highlights the lack of studies on the CKD-cancer connection and a CKD prevalence which ranges between 15 and 25% depending on the series,3 the results of kidney function, prevalence of CKD (defined by glomerular filtration rate <60ml/min/1.73m2) and type of cancer are presented in a cohort of non-hospitalised cancer patients, before carrying out a computed tomography scan with intravenous iodinated contrast medium for the monitoring of the clinical course of their disease.
It is a cross-sectional descriptive study from a database of 202 outpatients of the Hospital de Segovia, from the period of March to July 2016, in which the development of kidney disease was analysed by contrast prior to carrying out the computed tomography. From this database, 163 cancer outpatients were selected, of whom 90 were males (55.2%) with a mean age of 64.58 (range 22–87). The overall blood test data of the 163 cancer patients are: creatinine (mg/dl) 0.93±0.47 (0.6–5.2); urea (mg/dl) 42.00±15 (28–150); haematocrit (%) 42.96±4 (27.90–53); in urine (one urination): protein/creatinine (mg/mg): 0.11±0.18 (0–2.15); the estimated GFR by MDRD-4 (ml/min/1.73m2) is 83.17±19 (9.16–124). Of the total number of cancer patients, 19 (11.65%) have MDRD-4 <60ml/min/1.73m2: one patient in stage 5, eight patients in stage 3b and ten patients in stage 3a. In Table 1, the total frequency of cancer is presented, as well as the comparison according to the cut-off point of 60ml/min/1.73m2 for GFR; 35 patients have metastatic disease. Regarding the cancer treatments received prior to the performance of the control computed tomography scan with contrast: 102 (62.6%) patients had received chemotherapy: 68 platinum-based; 46 other chemotherapy agents; 61 (37.4%) had received radiotherapy; 128 (78.5%) had undergone surgery; 20 (12.3%) had a history of immunotherapy and 18 patients (11%) had received hormone therapy. One hundred and four patients (63.8%) had been treated with a combination of two or three types of cancer therapy. Only seven patients reported having used non-steroidal anti-inflammatories on the days prior to undergoing the computed tomography.
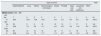
Frequency of cancers: overall and comparison according to glomerular filtration rate cut-off of 60ml/min/1.73m2.
| Type of cancer | Total | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Gastrointestinal | Lung | Kidney | Gynaecological (not breast) | Breast | Prostate | Head and neck | Leukaemia and lymphoma | Other | ||
| MDRD (ml/min./1.73m2) | ||||||||||
| <60 | ||||||||||
| No. | 7 | 3 | 3 | 3 | 0 | 1 | 1 | 1 | 0 | 19 |
| % | 36.8 | 15.8 | 15.8 | 15.8 | 0.0 | 5.3 | 5.3 | 5.3 | 0.0 | 100.0 |
| >60 | ||||||||||
| No. | 53 | 11 | 9 | 16 | 12 | 10 | 7 | 17 | 9 | 144 |
| % | 36.8 | 7.6 | 6.3 | 11.1 | 8.3 | 6.9 | 4.9 | 11.8 | 6.3 | 100.0 |
| Total | ||||||||||
| No. | 60 | 14 | 12 | 19 | 12 | 11 | 8 | 18 | 9 | 163 |
| % | 36.8 | 8.6 | 7.4 | 11.7 | 7.4 | 6.7 | 4.9 | 11.0 | 5.5 | 100.0 |
The kidney is an undesirable target (due to suffering from toxic consequences) of the active treatment of cancer (main target). In this study, we found a CKD prevalence of below 12%, lower than that reported in other series.3 Despite the fact that more than 60% of these patients had also received chemotherapy (including platinum-based), as well as combination therapies, this lower prevalence than that reported in other series may perhaps be justified by the fact that the patients were not undergoing active treatment when we created the cut-off point and we considered stable (non-hospitalised) patients who attended to undergo a computed tomography for the monitoring of the clinical course of their cancer. Furthermore, iodinated contrast media administered intravenously has been described as an inducer of acute kidney injury in patients with cancer, especially in unstable patients3,4: in this study, the assessment of kidney function was carried out prior to the administration of contrast, which means that the presence of this did not influence the results that we present.
Moreover, with regard to the most common types of cancer, Galceran et al. analysed the incidence of cancer in Spain in 2015 and report that, overall, the five most common types were gastrointestinal, prostate, lung, breast and urinary tract cancers.5 Our data also reflect the high prevalence of gastrointestinal cancers, with these being the most common of the entire series, and if we consider them according to the cut-off point of 60ml/min/1.73m2 of GFR. A high frequency of kidney cancer has been reported among patients on dialysis.6 In our study, although only one patient was in stage 5 of CKD (but without having started dialysis), if we include only patients with CKD we find that, after gastrointestinal cancers, kidney cancer, gynaecological cancers (not breast) and lung cancer are also the most common in patients with a worse degree of kidney function. However, these results should be considered with caution, as the number of patients with CKD is below twenty in this series and, therefore, it would be interesting to carry out more studies with a larger sample size which includes patients with GFR <60ml/min/1.73m2 to reach more robust conclusions.
In conclusion, in our study the prevalence of CKD in non-hospitalised cancer patients is lower than that reported in other series; the most common cancers are gastrointestinal cancers, both in patients with improved kidney function and with CKD.
Conflicts of interestThere are no conflicts of interest.
Please cite this article as: Heras Benito M, Calle García L, Fernández-Reyes Luis MJ. A propósito de la onconefrología: enfermedad renal crónica en pacientes oncológicos no hospitalizados. Nefrologia. 2020;40:365–366.



