
Peritonitis is both a common and serious complication in peritoneal dialysis (PD). It also leads to morbidity and mortality and patients may need to be transferred to haemodialysis. All dialysis programmes should be aware of and monitor the rate of peritonitis they go through. The guidelines of the International Society for Peritoneal Dialysis cite an overall target rate of 0.5 episodes/year. Establishing appropriate protocols is essential to normalize clinical practice and achieve the best possible clinical outcomes.1,2
In PD, prevention of peritonitis is very important to reduce its rate.3 It has been suggested that retraining may reduce the risk of peritonitis. Peritonitis rates are significantly reduced in centres with active retraining programmes compared to those that do not; with retraining, peritonitis caused in particular by Gram-positive germs is reduced.4 A multicentre randomised trial analysing the relationship between retraining and the peritonitis rate was recently published including 671 patients from different countries. The relative risk in the rate of peritonitis was found to be 0.93 (95% CI: 0.75–1.16).5
At our hospital, we set ourselves the objective of improving our overall peritonitis rate. In 2014, we decided to start retraining all our patients. The nursing staff are responsible of the retraining. It is carried out 30 days after starting home dialysis, after each episode of peritonitis or prolonged hospitalisation, after any r interruption in PD, and periodically every six months. Retraining includes re-education on hand washing procedures, connecting, infection control, contamination risks and intraperitoneal medication application. As our rate did not improve, despite the fact that retraining was apparently being carried out, from 2016, periodic retraining was established every six months to achieve the primary objective, to reduce the rate of peritonitis, based on continuous quality improvement in our unit. We set a percentage to achieve the indicator of 90%, and we monitor it every six months.
Since the retraining began in 2014, we have kept a record of peritonitis episodes in exposed patients, the overall peritonitis rate and the type of germs responsible. We compare the peritonitis rate and the type of germ (Gram-positive or negative) establishing the cut-off point at 2016, when we established scheduled retraining as a quality indicator. We have always managed to maintain the periodic retraining indicator above 90% compliance, using the occasion of the six-monthly reviews carried out as part of follow-up. To compare the data, we used the Student's t-test for independent data in the case of the peritonitis rate, and the Chi-square test for the type of germs, obtaining a statistically significant difference (p < 0.05). The rest of the results are shown in Table 1.
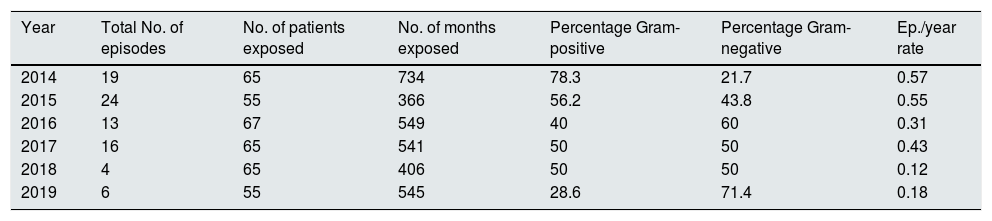
Results summary.
| Year | Total No. of episodes | No. of patients exposed | No. of months exposed | Percentage Gram-positive | Percentage Gram-negative | Ep./year rate |
|---|---|---|---|---|---|---|
| 2014 | 19 | 65 | 734 | 78.3 | 21.7 | 0.57 |
| 2015 | 24 | 55 | 366 | 56.2 | 43.8 | 0.55 |
| 2016 | 13 | 67 | 549 | 40 | 60 | 0.31 |
| 2017 | 16 | 65 | 541 | 50 | 50 | 0.43 |
| 2018 | 4 | 65 | 406 | 50 | 50 | 0.12 |
| 2019 | 6 | 55 | 545 | 28.6 | 71.4 | 0.18 |
Ep., episodes.
Despite following the recommendations established by the clinical guidelines, it was not until we established periodic retraining as a quality indicator that we were able to significantly reduce our peritonitis rate and change the spectrum of the causative germs. However, the improvement in the rate could also be due to other factors, as the design of our study means we cannot demonstrate causality. We conclude that continuous quality improvement initiatives based on scheduled retraining and site-specific outcomes could reduce peritonitis rates in PD. We believe that the root cause-effect analysis of specific local situations can lead to the design of ad-hoc strategies to improve clinical outcomes. There is still a limited amount of literature to support this practice.
Please cite this article as: Sastre López A, Linares Fano B, Aguilera Flórez A, Prieto Velasco M. El reentrenamiento programado reduce la tasa de peritonitis en diálisis peritoneal. Nefrologia. 2022;42:219–220.



