



Mouth ulcers are a cutaneous complication that can often affect kidney transplant patients, mostly due to the effect of immunosuppressive treatment.
Even so, before asserting that said complication is indeed secondary to drugs, it is very important to establish a differential diagnosis with other mouth ulcer causes, such as systemic diseases or viral infections, which are also common in these patients.
Las úlceras orales son una de las complicaciones cutáneas que pueden afectar con frecuencia a los pacientes trasplantados renales, debido muchas veces al efecto del tratamiento inmunosupresor.
Aun así, es importante, antes de asegurar que dicha complicación es secundaria a los fármacos, establecer el diagnóstico diferencial con otras causas de úlceras orales como pueden ser enfermedades sistémicas o infecciones virales, también frecuentes en este tipo de pacientes.
Differential diagnosis of oral ulcers is often difficult, because it covers a large number of disorders. Some infections such as the herpes virus, bullous, autoimmune and hematologic diseases and some malignancies are just a few examples of what may ulcerate the oral mucosa.1 In immunocompromised patients, some unusual disorders, otherwise uncommon in immunocompetent individuals, should also be considered, such as fungal infections, cytomegalovirus (CMV) or drug-induced ulcers. The latter are normally produced by immunosuppressive drugs and are therefore usually seen in polymedicated patients who are susceptible to all kinds of infections, which makes correct diagnosis even more complex.2 Unlike some immunosuppressants, where a higher capacity for resulting in oral ulcers has been demonstrated (mTOR inhibitors are most commonly associated with this type of ulcers), as far as we know, mycophenolate mofetil (MMF) has been noted to rarely cause oral ulcers with only 9 patients reported.1–6
Here we report one new case of MMF-induced oral ulcerations. We also review all patients in the literature with this uncommon side effect.
ReportA 67 year-old man with renal insufficiency due to polycystic kidney disease and arterial hypertension underwent a kidney transplant in 2015. He received immunosupressive treatment with metilprednisolone (5mg/d), tacrolimus (16mg/d) and MMF (2g/d). Nine months after kidney transplantation 3 painful oral ulcers appeared on both sides of the tongue and on the oral mucosa. He also presented intense odynophagia, difficulty swallowing, decreased intake and weight loss without fever. On examination, 2 major aphthous ulcers, with surrounding edema and erythema were present on his tongue (Fig. 1) and 1 smaller erosion was observed in his buccal mucosa (Fig. 2).


Apart from the immunosupressive treatment, at this moment he was also taking oral valganciclovir because of a CMV infection reactivation. The blood sample test showed leukopenia, anemia and thrombocytopenia with a stable renal function (creatinine 2.2mg/dl) and a normal hepatic profile. Levels of tacrolimus were correct in relation with the time after kidney transplantation.
Cultures of the oral lesions were negative for herpes simplex virus types 1 and 2, CMV, and fungus. Rapid plasma reagin (RPR) and HIV antibody testing results were nonreactive.
Oral biopsy showed nonspecific inflammatory changes on hematoxylin–eosin (H&E) staining. Finally MMF was subsequently discontinued. After 4 days, the patient's oral ulcers decreased considerably in size, with a significant reduction in his oral pain, improving the ability to eat and drink. After 9 days, complete healing of the patient's ulcers was observed. The patient has since remained off MMF with no recurrences of his ulcerations.
DiscussionMMF is a powerful immunosuppressant that is often used to prevent acute rejection in hematopoietic stem cell or solid organ transplant patients as well as in some autoimmune diseases.7,8 Its mechanism of action is based on inhibition of purine synthesis via inhibition of the inosine phosphate dehydrogenase enzyme. This results in a decrease in lymphocyte proliferation that is responsible for the immunosuppressive effects of the drug.7,8 Its most common side effects are digestive in the form of diarrhea or vomiting with extremely varied other adverse effects. Among them, oral ulcers are one of the less frequent and therefore less known by dermatologists.
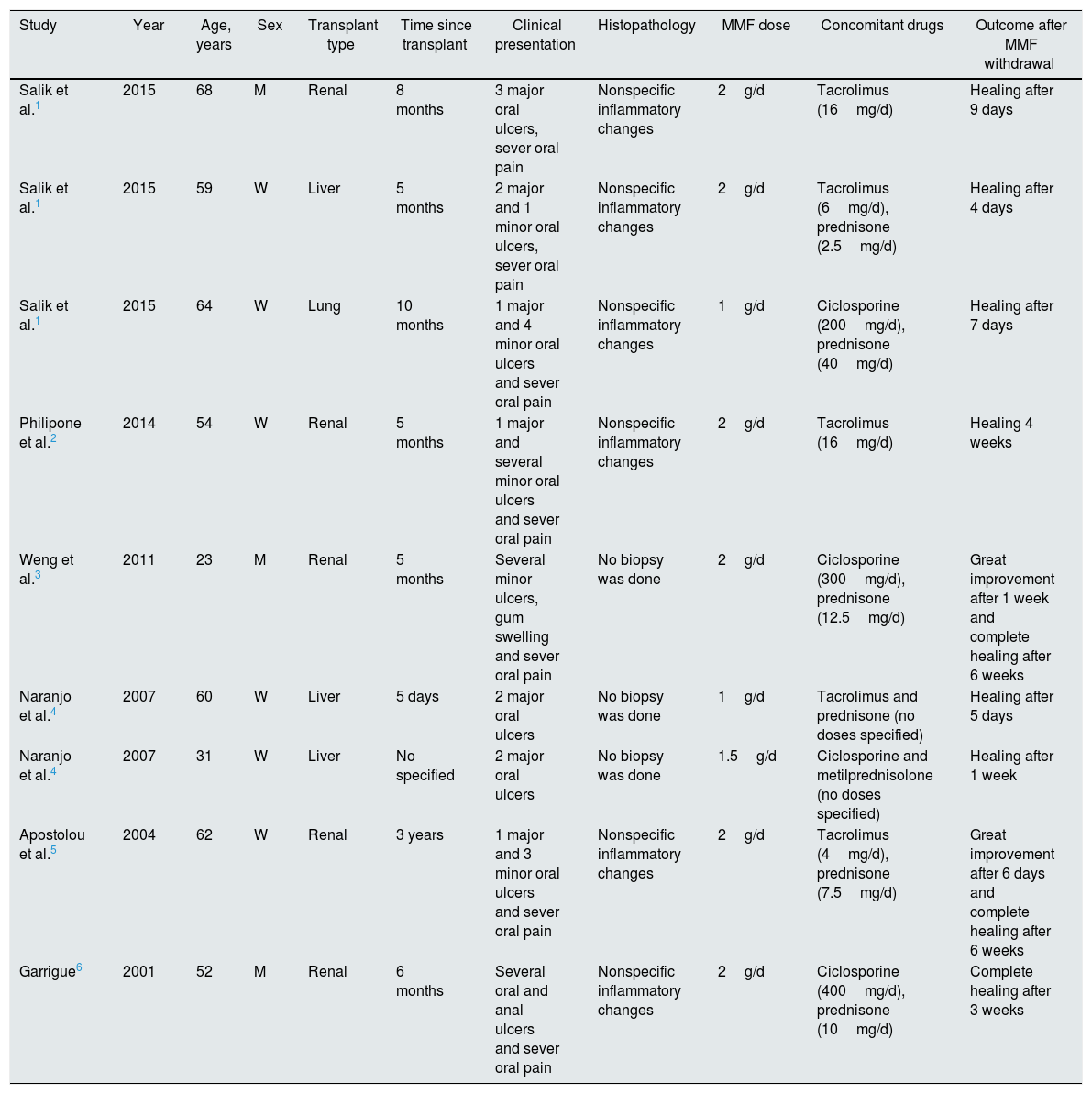
We searched PubMed with the terms “mycophenolate mofetil” and “oral ulceration” and found 9 cases in the English-language literature. Characteristics of the patients are shown in Table 1.
Characteristics of the patients included in the study.
| Study | Year | Age, years | Sex | Transplant type | Time since transplant | Clinical presentation | Histopathology | MMF dose | Concomitant drugs | Outcome after MMF withdrawal |
|---|---|---|---|---|---|---|---|---|---|---|
| Salik et al.1 | 2015 | 68 | M | Renal | 8 months | 3 major oral ulcers, sever oral pain | Nonspecific inflammatory changes | 2g/d | Tacrolimus (16mg/d) | Healing after 9 days |
| Salik et al.1 | 2015 | 59 | W | Liver | 5 months | 2 major and 1 minor oral ulcers, sever oral pain | Nonspecific inflammatory changes | 2g/d | Tacrolimus (6mg/d), prednisone (2.5mg/d) | Healing after 4 days |
| Salik et al.1 | 2015 | 64 | W | Lung | 10 months | 1 major and 4 minor oral ulcers and sever oral pain | Nonspecific inflammatory changes | 1g/d | Ciclosporine (200mg/d), prednisone (40mg/d) | Healing after 7 days |
| Philipone et al.2 | 2014 | 54 | W | Renal | 5 months | 1 major and several minor oral ulcers and sever oral pain | Nonspecific inflammatory changes | 2g/d | Tacrolimus (16mg/d) | Healing 4 weeks |
| Weng et al.3 | 2011 | 23 | M | Renal | 5 months | Several minor ulcers, gum swelling and sever oral pain | No biopsy was done | 2g/d | Ciclosporine (300mg/d), prednisone (12.5mg/d) | Great improvement after 1 week and complete healing after 6 weeks |
| Naranjo et al.4 | 2007 | 60 | W | Liver | 5 days | 2 major oral ulcers | No biopsy was done | 1g/d | Tacrolimus and prednisone (no doses specified) | Healing after 5 days |
| Naranjo et al.4 | 2007 | 31 | W | Liver | No specified | 2 major oral ulcers | No biopsy was done | 1.5g/d | Ciclosporine and metilprednisolone (no doses specified) | Healing after 1 week |
| Apostolou et al.5 | 2004 | 62 | W | Renal | 3 years | 1 major and 3 minor oral ulcers and sever oral pain | Nonspecific inflammatory changes | 2g/d | Tacrolimus (4mg/d), prednisone (7.5mg/d) | Great improvement after 6 days and complete healing after 6 weeks |
| Garrigue6 | 2001 | 52 | M | Renal | 6 months | Several oral and anal ulcers and sever oral pain | Nonspecific inflammatory changes | 2g/d | Ciclosporine (400mg/d), prednisone (10mg/d) | Complete healing after 3 weeks |
MMF, mycophenolate mofetil.
Since the first case reported in 2001, 9 additional cases of MMF-oral ulcerations have been described (including our patient) presenting as very painful ulcers1 (2 or more ulcers per patient), located in the oral mucosa. One case had also anal ulcers and another, edema in gums. To date, all cases published, are in patients who have undergone a solid organ transplant and the dose of MMF that they were receiving, ranged from 1 to 2g/d. In all the cases, the ulcers healed quickly once the drug was stopped. In every reported case improvement of the lesions is observed within the first 4–10 days and complete healing is seen in 6 weeks at most.1–6 Our patient referred significant improvement only four days after stopping the drug. These lesions are usually not accompanied by other side effects and the interval time between starting the drug and the appearance of the ulcers varies greatly, with described cases ranging from 1 week to 3 years.
From the microscopic point of view no specific findings are observed, usually showing nonspecific mixed inflammatory infiltrates with a negative immunofluorescence.1
Despite of this, in our opinion biopsy should always be performed in order to rule out other common diseases such as fungal infections or CMV.
Regarding the pathogenesis of these lesions, most authors propose their appearance as the result of a direct cytotoxic effect of the drug on the mucosa although this point is not yet fully proven.
In conclusion, oral ulcers caused by MMF are a rare cause of oral ulcers that dermatologists should be aware of.
Conflict of interestsThe authors declare no conflict of interests.



