




We aimed to describe the thiamine status in hospitalized hypervolemic heart failure (HF) and/or renal failure (RF) patients treated with furosemide and to investigate whether there was a difference in furosemide-related thiamine deficiency between patients with RF and HF.
MethodsPatients who were diagnosed as hypervolemia and treated with intravenous furosemide (at least 40mg/day) were included in this prospective observational study. Whole blood thiamine concentrations were measured 3 times during hospital follow-up of patients.
ResultsWe evaluated 61 hospitalized hypervolemic patients, of which 22 (36%) were men and 39 (64%) were women, with a mean age of 69.00±10.39 (45–90) years. The baseline and post–hospital admission days 2 and 4 mean thiamine levels were 51.71±20.66ng/ml, 47.64±15.43ng/ml and 43.78±16.20ng/ml, respectively. Thiamine levels of the hypervolemic patients decreased significantly during the hospital stay while furosemide treatment was continuing (p=0.029). There was a significant decrease in thiamine levels in patients who had HF (p=0.026) and also, thiamine was significantly lower in HF patients who had previously used oral furosemide before hospitalization. However, these findings were not present in patients with RF.
ConclusionsThiamine substantially decreases in most hypervolemic patients receiving intravenous furosemide treatment during the hospital stay. Thiamine levels were significantly decreased with furosemide treatment in especially HF patients, but the decrease in thiamine levels did not detected at the same rate in RF patients. Diuretic-induced thiamine loss may be less likely in RF patients, probably due to a reduction in excretion.
Nos propusimos describir el estado de la tiamina en pacientes hospitalizados con insuficiencia cardíaca (IC) y/o insuficiencia renal (IR) hipervolémica tratados con furosemida, e investigar si había una diferencia en la deficiencia de tiamina relacionada con la furosemida entre los pacientes con IR y con IC.
MétodosEn este estudio observacional prospectivo se incluyeron pacientes con diagnóstico de hipervolemia y tratados con furosemida intravenosa (al menos 40 mg/día). Se midieron las concentraciones de tiamina en sangre total 3 veces durante el seguimiento hospitalario de los pacientes.
ResultadosSe evaluaron 61 pacientes hipervolémicos hospitalizados, de los cuales 22 (36%) eran hombres y 39 (64%) eran mujeres, con una edad media de 69,00±10,39 (45-90) años. Los niveles medios de tiamina en la línea de base y tras el ingreso hospitalario en los días 2 y 4 fueron de 51,71±20,66 ng/ml, 47,64±15,43 ng/ml y 43,78±16,20 ng/ml, respectivamente. Los niveles de tiamina de los pacientes hipervolémicos hipervolemia disminuyeron significativamente durante la estancia en el hospital mientras se mantenía el tratamiento con furosemida furosemida (p = 0,029). Hubo una disminución significativa de los niveles de tiamina en los pacientes que tenían IC (p = 0,026) y también, la tiamina fue significativamente menor en los pacientes con IC que habían habían utilizado previamente furosemida oral antes de la hospitalización. Sin embargo, estos hallazgos no se presentes en los pacientes con IC.
ConclusionesLa tiamina disminuye sustancialmente en la mayoría de los pacientes hipervolémicos que reciben tratamiento con furosemida intravenosa durante la estancia hospitalaria. Los niveles de tiamina se redujeron significativamente con el tratamiento con furosemida, especialmente en los pacientes con IC, pero la disminución de los niveles de tiamina no se detectó al mismo ritmo en los pacientes con IC. La pérdida de tiamina inducida por los diuréticos inducida por los diuréticos puede ser menos probable en los pacientes con insuficiencia cardiaca, probablemente debido a una reducción de la excreción.
Two major causes of hypervolemia are renal failure (RF) and heart failure (HF). Impaired renal function can be present in 50% of patients treated for acute HF.1 Even moderate degrees of renal insufficiency are independently associated with an increased risk of mortality from any cause in patients with HF.2 Patients with RF have a significantly increased risk of mortality, with half of these deaths attributed to cardiovascular disease. Therefore, RF and HF are two intertwined conditions.
Thiamine deficiency causes high-output HF and volume overload.3 The cardiovascular symptoms of thiamine deficiency may be difficult to distinguish from those of HF. Although overt symptoms and signs of thiamine deficiency might not be present, functional thiamine deficiency may contribute to various complications including hypervolemia and ultimately increased mortality in RF and HF patients. But, it is not known exactly how thiamine level is changing with diuretic treatment in hypervolemic patients with RF and/or HF.
Furosemide is a loop diuretic which is commonly used in hypervolemic patients in HF and RF. Studies of the association between the use of furosemide and thiamine levels gave conflicting results. Findings of two different studies were consistent with thiamine deficiency in a high proportion of patients treated with furosemide for HF.4,5 On the other hand, the other study found no significant difference in thiamine levels between a group with HF and a control group.6 Although there are studies evaluating thiamine deficiency in HF patients using diuretics as in the mentioned studies in the literature, there are not enough studies evaluating diuretic related thiamine deficiency in RF patients without HF. It is not known whether the effect of furosemide on thiamine levels is different when RF is present alone.
The incidence and consequences of thiamine deficiency and the related conditions of this deficiency among hypervolemic patients are not well known. For these reasons, in the performed study, we aimed (1) to describe the thiamine status in hypervolemic HF and/or RF patients treated with furosemide; (2) to establish the impact of ongoing doses of furosemide during hospitalization on thiamine blood concentrations; (3) to investigate whether there was a difference in furosemide-related thiamine deficiency between patients with RF and HF; and (4) to examine the potential role of renal function in conflicting results of the previous studies considering furosemide-related thiamine loss. Moreover, filling the gap in knowledge about the influence of furosemide on thiamine losses may help to establish what is an adequate dose of thiamine supplementation in hypervolemic patients with RF and/or HF.
Materials and methodsDesign and participantsWe conducted a prospective observational study in the department of internal medicine, nephrology and cardiology at a Tertiary Care Research Hospital. The study protocol was approved by the Ethics Committee of Erciyes University (Ethics Committee approval code: 307/2018). The study was conducted ethically in accordance with the World Medical Association Declaration of Helsinki. We obtained written informed consent from all patients.
We collected clinical data on 62 adult patients who diagnosed with hypervolemia due to HF and/or RF and hospitalized between February 2018 and February 2019. Of the 62 patients, 1 patient with insufficient clinical data were excluded. Finally, 61 patients were enrolled in this study and all patients finished the study with a full follow-up. The diagnosis of hypervolemia was made through the medical signs and symptoms, physical exam findings (ascites, crackles on auscultation, edema, high blood pressure, jugular vein distension), patient's medical history, and tests and exams including: abdominal ultrasound, electrocardiogram, echocardiography and chest X-ray. HF was diagnosed according to echocardiography and European Society of Cardiology 2016 guidelines7 and RF was diagnosed according to the criteria published by the 2012 KDIGO study group.8 RF patients involving stage 2–5 patients were chronic RF patients who had not yet undergoing dialysis.
Patients who were diagnosed as hypervolemia and treated with intravenous furosemide (at least 40mg/day) were included in the study. The exclusion criteria were as follows: patients taking vitamin and trace microelements supplementation, patients that were hospitalized<72h, unconscious patients, patients with acute infection, chronic illness such as neoplasia and liver disease, patients who previously underwent bowel surgery and patients reporting any amount of regular alcohol use. A chronic renal failure diet (∼1800 calories, controlled protein, limited potassium, phosphorus and sodium) was recommended to all patients included in the study during hospitalization. Patients were not allowed to use vitamin supplements during the duration of the study.
Whole blood thiamine concentrations were measured 3 times during hospital follow-up of patients. First measurements (baseline) were made in all subjects on the first day of hospitalization when furosemide treatment was not started yet. Second and third measurements were performed serially on the second and fourth days of hospitalization while furosemide treatment was continuing. Echocardiographic evaluations of patients were made at the time of hospitalization.
Data collectionAt the time of the patients’ enrollment, demographic information (age and sex) was recorded. Data on preexisting conditions including comorbidities, admission diagnosis, clinical characteristics, the condition that prompted admission, length of hospital stay (number of days between admission and discharge) and also destination post-hospital (home, transfer to intensive care unit or death) were obtained from the clinical files. We monitored and followed patients from admission to discharge from the hospital.
Echocardiographic evaluationEchocardiographic examination was performed with an echocardiography device (7 EPIQ Philips ultrasound, for Philips Healthcare) using a 2.5MHz transducer, in the left lateral decubitus position. The patients underwent M-mode echocardiography, two-dimensional echocardiography, pulsed and continuous wave Doppler, and color Doppler echocardiographic evaluations, respectively. From the parasternal long axis with M-mode (at mitral valve chordal level, perpendicular to the long axis of the ventricle), left ventricular end-diastolic diameter, left ventricular end-systolic diameter, interventricular thickness and posterior wall thickness were recorded.
Ejection fraction was calculated using the modified Simpson method. Left ventricular mass index was calculated using the following Devereux formula9–11:


Values below 115g/m2 among males and 95g/m2 among women were considered normal, while values above were considered as hypertrophic.
Patients who had suspicious symptoms, prior clinical history and physical examination for heart failure and who had normal or near normal ejection fraction (>50 percent) and evidence of cardiac dysfunction as a cause of symptoms (abnormal left ventricle filling and elevated filling pressures) diagnosed with heart failure with preserved ejection fraction or who had reduced ejection fraction and structural and/or functional impairment of the left ventricle diagnosed with heart failure with reduced ejection fraction.
Laboratory analysisOn admission, a routine blood sample was taken and tested for complete blood count, routine biochemical parameters. After an overnight fast, venous blood was collected from each subject into tubes containing EDTA. These samples were immediately frozen at -80°C in aliquots for later measurement of thiamine. A high performance liquid chromatography-based method (HPLC; Shimadzu, Immuchrom, Japan) was used to measure thiamine levels with the reference range of normality as 35–99ng/ml. Blood samples for thiamine measurement at baseline and on day 2 were obtained from 61 subjects. On day 4 of hospital stay, blood samples for thiamine measurement were obtained from 51 subjects.
Statistical analysisThe normality and the homogeneity of the data were evaluated by Shapiro–Wilk test and Levene test, respectively. Comparisons among the groups (RF, HF and RF+HF) for continuous variables were performed by using the Student t-test or one-way ANOVA for normal distribution and the Mann–Whitney U test or Kruskal–Wallis test for nonnormal distribution. Fisher test or the Chi-square test was used for all categorical data. The thiamine level differences over time within each group (RF, HF and RF+HF) were compared using a Friedman's non-parametric test. A separate Wilcoxon-signed rank test was used in paired comparisons of thiamine levels on different hospitalization days. All calculations used the SPSS statistical package (version 15.0; SPSS, Chicago, IL, USA). p<0.05 was considered statistically significant.
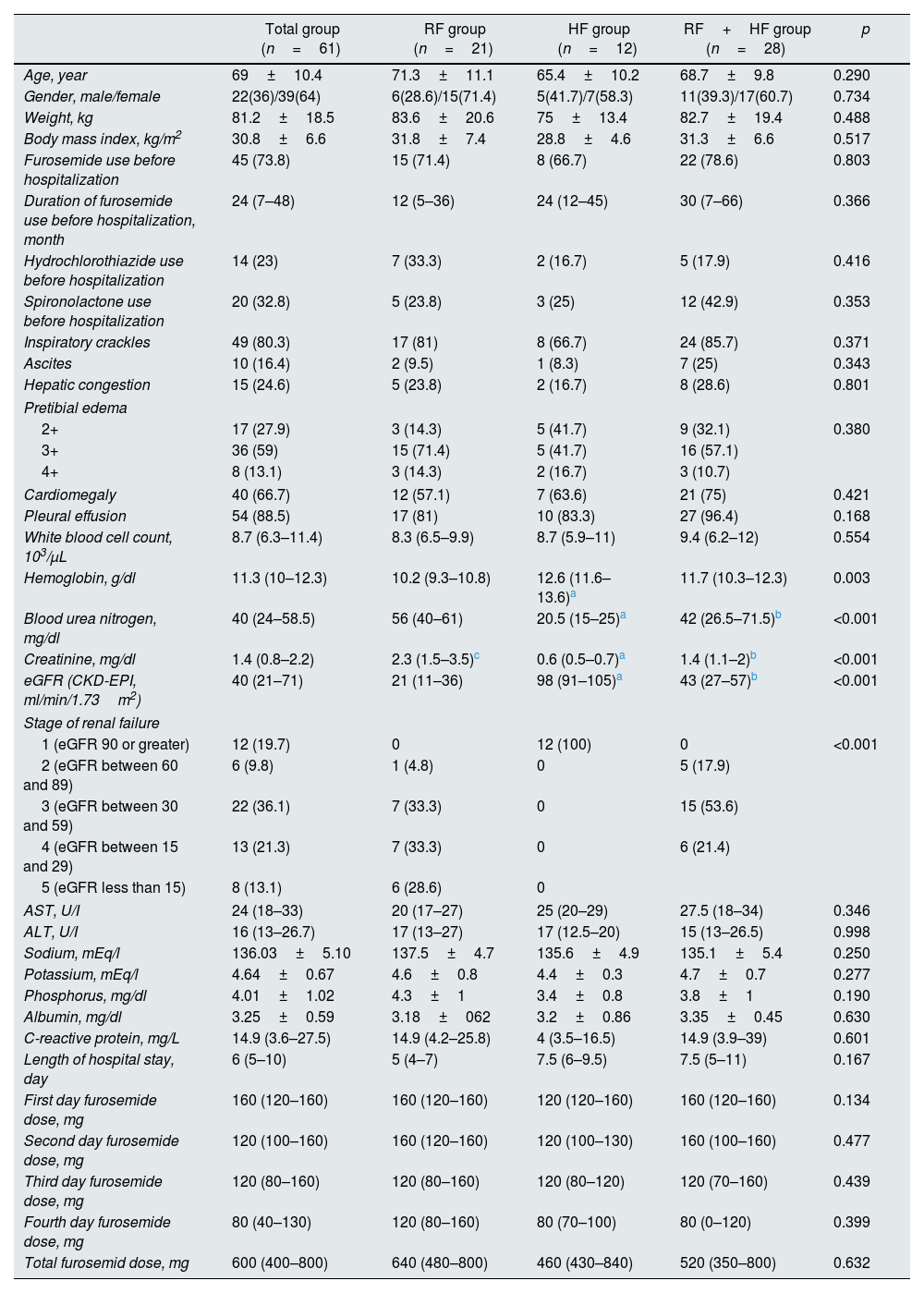
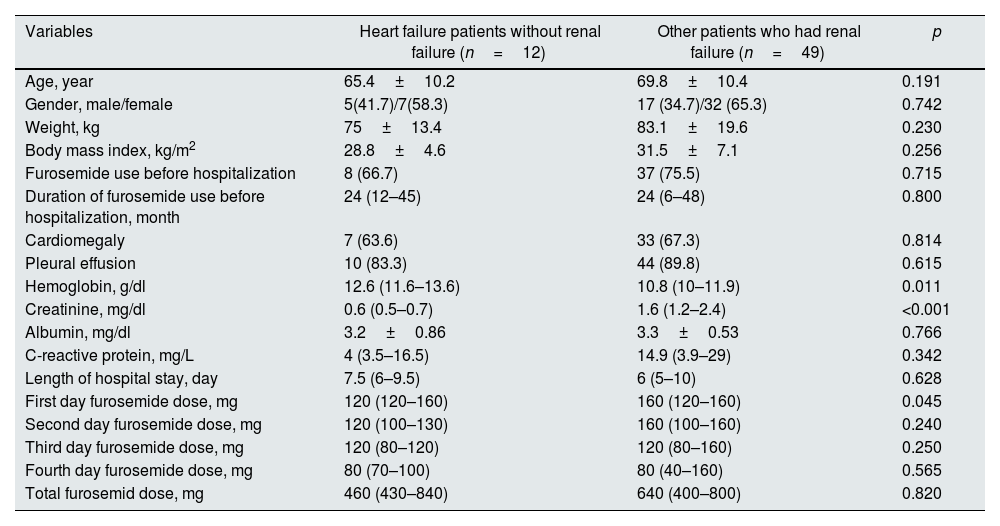
ResultsIn this study, we evaluated 61 patients who diagnosed with hypervolemia and hospitalized in the clinic, of which 22 (36%) were men and 39 (64%) were women, with a mean age of 69.00±10.4 (45–90) years. Patients baseline characteristics were as follows: 13 patients (21.3%) had hypertension, 42 patients (70.5%) had diabetes mellitus, and 45 patients (73.8%) were receiving furosemide treatment for at least 4 weeks before hospitalization. While RF and HF coexisted in 28 hypervolemic patients, 12 hypervolemic patients had only HF and 21 hypervolemic patients had only RF. Baseline and clinical follow-up characteristics of study participants were showed in Table 1 according to groups. There was no significant differences between the groups in terms of demographic, clinical and laboratory parameters, except for hemoglobin and renal function tests. Hemoglobin was significantly lower in RF patients than HF patients (p=0.003) and creatinine was significantly higher in RF patients than other groups (p<0.001) (Table 1). Furthermore, we compared demographic, clinical and laboratory parameters between HF patients without RF and other patients who had RF in Table 2. Patients who had RF had significantly lower hemoglobin value (p=0.011) and higher first day furosemide dose (p=0.045) than heart failure patients without renal failure.
Baseline and clinical follow-up characteristics of study participants according to groups.
| Total group (n=61) | RF group (n=21) | HF group (n=12) | RF+HF group (n=28) | p | |
|---|---|---|---|---|---|
| Age, year | 69±10.4 | 71.3±11.1 | 65.4±10.2 | 68.7±9.8 | 0.290 |
| Gender, male/female | 22(36)/39(64) | 6(28.6)/15(71.4) | 5(41.7)/7(58.3) | 11(39.3)/17(60.7) | 0.734 |
| Weight, kg | 81.2±18.5 | 83.6±20.6 | 75±13.4 | 82.7±19.4 | 0.488 |
| Body mass index, kg/m2 | 30.8±6.6 | 31.8±7.4 | 28.8±4.6 | 31.3±6.6 | 0.517 |
| Furosemide use before hospitalization | 45 (73.8) | 15 (71.4) | 8 (66.7) | 22 (78.6) | 0.803 |
| Duration of furosemide use before hospitalization, month | 24 (7–48) | 12 (5–36) | 24 (12–45) | 30 (7–66) | 0.366 |
| Hydrochlorothiazide use before hospitalization | 14 (23) | 7 (33.3) | 2 (16.7) | 5 (17.9) | 0.416 |
| Spironolactone use before hospitalization | 20 (32.8) | 5 (23.8) | 3 (25) | 12 (42.9) | 0.353 |
| Inspiratory crackles | 49 (80.3) | 17 (81) | 8 (66.7) | 24 (85.7) | 0.371 |
| Ascites | 10 (16.4) | 2 (9.5) | 1 (8.3) | 7 (25) | 0.343 |
| Hepatic congestion | 15 (24.6) | 5 (23.8) | 2 (16.7) | 8 (28.6) | 0.801 |
| Pretibial edema | |||||
| 2+ | 17 (27.9) | 3 (14.3) | 5 (41.7) | 9 (32.1) | 0.380 |
| 3+ | 36 (59) | 15 (71.4) | 5 (41.7) | 16 (57.1) | |
| 4+ | 8 (13.1) | 3 (14.3) | 2 (16.7) | 3 (10.7) | |
| Cardiomegaly | 40 (66.7) | 12 (57.1) | 7 (63.6) | 21 (75) | 0.421 |
| Pleural effusion | 54 (88.5) | 17 (81) | 10 (83.3) | 27 (96.4) | 0.168 |
| White blood cell count, 103/μL | 8.7 (6.3–11.4) | 8.3 (6.5–9.9) | 8.7 (5.9–11) | 9.4 (6.2–12) | 0.554 |
| Hemoglobin, g/dl | 11.3 (10–12.3) | 10.2 (9.3–10.8) | 12.6 (11.6–13.6)a | 11.7 (10.3–12.3) | 0.003 |
| Blood urea nitrogen, mg/dl | 40 (24–58.5) | 56 (40–61) | 20.5 (15–25)a | 42 (26.5–71.5)b | <0.001 |
| Creatinine, mg/dl | 1.4 (0.8–2.2) | 2.3 (1.5–3.5)c | 0.6 (0.5–0.7)a | 1.4 (1.1–2)b | <0.001 |
| eGFR (CKD-EPI, ml/min/1.73m2) | 40 (21–71) | 21 (11–36) | 98 (91–105)a | 43 (27–57)b | <0.001 |
| Stage of renal failure | |||||
| 1 (eGFR 90 or greater) | 12 (19.7) | 0 | 12 (100) | 0 | <0.001 |
| 2 (eGFR between 60 and 89) | 6 (9.8) | 1 (4.8) | 0 | 5 (17.9) | |
| 3 (eGFR between 30 and 59) | 22 (36.1) | 7 (33.3) | 0 | 15 (53.6) | |
| 4 (eGFR between 15 and 29) | 13 (21.3) | 7 (33.3) | 0 | 6 (21.4) | |
| 5 (eGFR less than 15) | 8 (13.1) | 6 (28.6) | 0 | ||
| AST, U/I | 24 (18–33) | 20 (17–27) | 25 (20–29) | 27.5 (18–34) | 0.346 |
| ALT, U/I | 16 (13–26.7) | 17 (13–27) | 17 (12.5–20) | 15 (13–26.5) | 0.998 |
| Sodium, mEq/l | 136.03±5.10 | 137.5±4.7 | 135.6±4.9 | 135.1±5.4 | 0.250 |
| Potassium, mEq/l | 4.64±0.67 | 4.6±0.8 | 4.4±0.3 | 4.7±0.7 | 0.277 |
| Phosphorus, mg/dl | 4.01±1.02 | 4.3±1 | 3.4±0.8 | 3.8±1 | 0.190 |
| Albumin, mg/dl | 3.25±0.59 | 3.18±062 | 3.2±0.86 | 3.35±0.45 | 0.630 |
| C-reactive protein, mg/L | 14.9 (3.6–27.5) | 14.9 (4.2–25.8) | 4 (3.5–16.5) | 14.9 (3.9–39) | 0.601 |
| Length of hospital stay, day | 6 (5–10) | 5 (4–7) | 7.5 (6–9.5) | 7.5 (5–11) | 0.167 |
| First day furosemide dose, mg | 160 (120–160) | 160 (120–160) | 120 (120–160) | 160 (120–160) | 0.134 |
| Second day furosemide dose, mg | 120 (100–160) | 160 (120–160) | 120 (100–130) | 160 (100–160) | 0.477 |
| Third day furosemide dose, mg | 120 (80–160) | 120 (80–160) | 120 (80–120) | 120 (70–160) | 0.439 |
| Fourth day furosemide dose, mg | 80 (40–130) | 120 (80–160) | 80 (70–100) | 80 (0–120) | 0.399 |
| Total furosemid dose, mg | 600 (400–800) | 640 (480–800) | 460 (430–840) | 520 (350–800) | 0.632 |
Data are expressed as the mean±SD, median (upper–lower quartile) or noun (percentage). eGFR: estimated glomerular filtration rate, CKD-EPI: Chronic Kidney Disease Epidemiology Collaboration, AST: aspartate aminotransferase, ALT: alanine aminotransferase.
Demographic, clinical and laboratory parameters of heart failure patients without renal failure and other patients who had renal failure.
| Variables | Heart failure patients without renal failure (n=12) | Other patients who had renal failure (n=49) | p |
|---|---|---|---|
| Age, year | 65.4±10.2 | 69.8±10.4 | 0.191 |
| Gender, male/female | 5(41.7)/7(58.3) | 17 (34.7)/32 (65.3) | 0.742 |
| Weight, kg | 75±13.4 | 83.1±19.6 | 0.230 |
| Body mass index, kg/m2 | 28.8±4.6 | 31.5±7.1 | 0.256 |
| Furosemide use before hospitalization | 8 (66.7) | 37 (75.5) | 0.715 |
| Duration of furosemide use before hospitalization, month | 24 (12–45) | 24 (6–48) | 0.800 |
| Cardiomegaly | 7 (63.6) | 33 (67.3) | 0.814 |
| Pleural effusion | 10 (83.3) | 44 (89.8) | 0.615 |
| Hemoglobin, g/dl | 12.6 (11.6–13.6) | 10.8 (10–11.9) | 0.011 |
| Creatinine, mg/dl | 0.6 (0.5–0.7) | 1.6 (1.2–2.4) | <0.001 |
| Albumin, mg/dl | 3.2±0.86 | 3.3±0.53 | 0.766 |
| C-reactive protein, mg/L | 4 (3.5–16.5) | 14.9 (3.9–29) | 0.342 |
| Length of hospital stay, day | 7.5 (6–9.5) | 6 (5–10) | 0.628 |
| First day furosemide dose, mg | 120 (120–160) | 160 (120–160) | 0.045 |
| Second day furosemide dose, mg | 120 (100–130) | 160 (100–160) | 0.240 |
| Third day furosemide dose, mg | 120 (80–120) | 120 (80–160) | 0.250 |
| Fourth day furosemide dose, mg | 80 (70–100) | 80 (40–160) | 0.565 |
| Total furosemid dose, mg | 460 (430–840) | 640 (400–800) | 0.820 |
Data are expressed as the mean±SD, median (upper–lower quartile) or noun (percentage). eGFR: estimated glomerular filtration rate, CKD-EPI: Chronic Kidney Disease Epidemiology Collaboration.
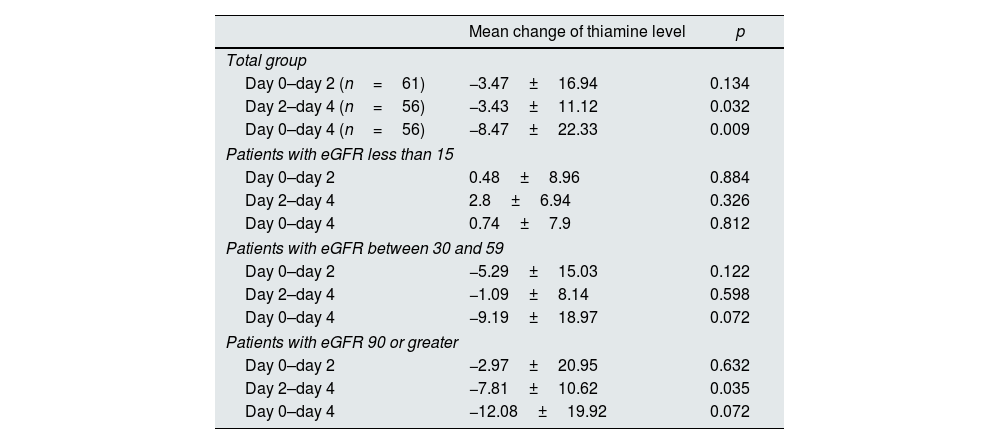
In all subjects, the baseline and post-hospital admission days 2 and 4 whole blood mean thiamine levels in the hospital were 51.71±20.66ng/ml, 47.64±15.43ng/ml and 43.78±16.20ng/ml, respectively. Thiamine levels of the hypervolemic patients decreased significantly during the hospital stay while furosemide treatment was continuing (p=0.029) (Table 3). Thiamine deficiency (thiamine levels<35ng/ml) was detected in 19.7% (n=12) of our patients at the time of hospitalization, 44.3% (n=27) of patients had thiamine deficiency on the 4th day of hospitalization. There was a significant decrease in thiamine levels in patients who had eGFR 90 or greater during hospital stay (Table 3). However, there was no such decrease in stage 5 RF patients and there was even an increase (Table 3), although they had higher first day furosemide dose (Table 2).
The mean changes of thiamine levels in total group and patients with different eGFR during hospital stay.
| Mean change of thiamine level | p | |
|---|---|---|
| Total group | ||
| Day 0–day 2 (n=61) | −3.47±16.94 | 0.134 |
| Day 2–day 4 (n=56) | −3.43±11.12 | 0.032 |
| Day 0–day 4 (n=56) | −8.47±22.33 | 0.009 |
| Patients with eGFR less than 15 | ||
| Day 0–day 2 | 0.48±8.96 | 0.884 |
| Day 2–day 4 | 2.8±6.94 | 0.326 |
| Day 0–day 4 | 0.74±7.9 | 0.812 |
| Patients with eGFR between 30 and 59 | ||
| Day 0–day 2 | −5.29±15.03 | 0.122 |
| Day 2–day 4 | −1.09±8.14 | 0.598 |
| Day 0–day 4 | −9.19±18.97 | 0.072 |
| Patients with eGFR 90 or greater | ||
| Day 0–day 2 | −2.97±20.95 | 0.632 |
| Day 2–day 4 | −7.81±10.62 | 0.035 |
| Day 0–day 4 | −12.08±19.92 | 0.072 |
Data are expressed as the mean±SD. eGFR: estimated glomerular filtration rate.
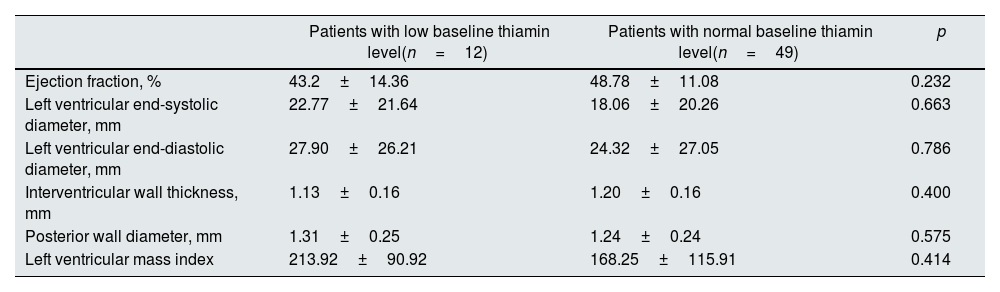
Patients with low thiamine levels had longer hospital stay (10.9±7.9 day, 7.3±3.8 day; respectively), although not statistically significant (p=0.148). There was no significant difference in echocardiographic findings at the time of hospitalization in patients with low thiamine levels (Table 4).
Comparison of echocardiographic findings in patients with low and normal thiamine levels at the time of hospitalization.
| Patients with low baseline thiamin level(n=12) | Patients with normal baseline thiamin level(n=49) | p | |
|---|---|---|---|
| Ejection fraction, % | 43.2±14.36 | 48.78±11.08 | 0.232 |
| Left ventricular end-systolic diameter, mm | 22.77±21.64 | 18.06±20.26 | 0.663 |
| Left ventricular end-diastolic diameter, mm | 27.90±26.21 | 24.32±27.05 | 0.786 |
| Interventricular wall thickness, mm | 1.13±0.16 | 1.20±0.16 | 0.400 |
| Posterior wall diameter, mm | 1.31±0.25 | 1.24±0.24 | 0.575 |
| Left ventricular mass index | 213.92±90.92 | 168.25±115.91 | 0.414 |
Hemodialysis treatment was needed in 12 patients (19.7%). Thiamine levels in patients who needed hemodialysis were significantly decreased during hospital stay (p=0.032). However, there was no significant decrease in thiamine levels in patients who did not require hemodialysis (p=0.193) (Fig. 1).

During hospital follow-up, 8.2% of the patients (n=5) died. There was no significant difference in thiamine levels between patients who had death and patients who had no death from hypervolemia, but thiamine levels were lower in patients who had death (37.30±8.09, 48.14±15.64; respectively, p=0.178).
To better establish the effects of RF and HF on thiamine levels, it was investigated for three different groups. One of the groups (n=12) consisted only patients who had HF, the other group (n=21) consisted only patients who had RF alone and RF and HF coexisted in patients in the third group (n=28). While there was no significant change in thiamine levels in patients who had RF alone, there was a significant decrease in patients who had HF and patients who had HF and RF in paired comparisons of thiamine levels on different hospitalization days (Fig. 2).
 over time in only RF patients (a), only HF patients (b), and HF and RF coexisted patients (c). The thiamine level changes over time within each group (RF, HF and RF+HF) were compared using a Friedman")
Serial whole blood thiamine concentrations (ng/ml) over time in only RF patients (a), only HF patients (b), and HF and RF coexisted patients (c). The thiamine level changes over time within each group (RF, HF and RF+HF) were compared using a Friedman's non-parametric test and p values were 0.829, 0.078 and 0.042; consecutively. A separate Wilcoxon-signed rank test was used in paired comparisons of thiamine levels on different hospitalization days and p values were shown in figure.
We investigated the effects of furosemide on baseline thiamine levels in the HF and RF patients who had recieved furosemide for more than 4 weeks before the hospitalization. Baseline thiamine was significantly lower in HF patients who had previously used furosemide (Table 5). But, there was no significant difference in baseline thiamine levels at the time of hospitalization in RF patients and patients who had HF and RF.
The relationship between furosemide use and baseline thiamine concentrations (ng/ml) in the HF and RF patients who had received furosemide for more than 4 weeks before the hospitalization.
| Subjects receiving furosemide before hospitalization | Subjects not receiving furosemide before hospitalization | p | |
|---|---|---|---|
| Baseline thiamine of HF patients | n=845.38±10.94 | n=468.43±21.64 | 0.031 |
| Baseline thiamine of RF patients | n=1545.10±17.71 | n=640.1±3.4 | 0.523 |
| Baseline thiamine of HF and RF coexisted patients | n=2257.9±23.7 | n=650.8±24.9 | 0.521 |
In this prospective observational study, it was found that thiamine levels decreased gradually with furosemide treatment in hospitalized hypervolemic patients and this finding was prominent in HF patients. Significant depletion of thiamine was present in hypervolemic HF patients receiving chronic diuretic therapy prior to hospital admission. However, these findings were not present in patients with RF. To date, there are many studies related to this subject in HF patients, but a few studies have evaluated furosemide related thiamine status in RF patients and those studies yielded conflicting results.12 There is no comparative study in the literature and this is the first time that the differences in thiamine levels between RF and HF patients are described in association with furosemide treatment. Our study reveals that furosemide related thiamine deficiency is not as prominent in RF patients as in HF patients.
Thiamine is eliminated from the body by renal excretion that is dependent on glomerular filtration rate and on thiamine plasma concentrations.13 Several studies documented thiamine deficiency secondary to diuretic therapy.5,14,15 The mechanism of thiamine deficiency with diuretic therapy is increased urinary thiamine excretion, which depends on urinary flow rate. 14,16–18 However, our study and Saka et al.’s study which investigated thiamine status in end-stage chronic kidney disease patients did not show any such correlation.19 The reason for the difference between this study and previous studies could be as follows. In most previous studies, diuretics were used in patients with congestive heart failure in whom kidney function was not severely impaired.5,16,20,21 In those cases, urinary flow rate might have increased in response to diuretic therapy. In contrast, the diuretic response is poor in RF patients, such as those in our study. This could explain why the current study showed no significant association between blood thiamine concentration and loop diuretic usage in RF patients. We thought that the poor diuretic response in RF patient population and therefore inadequate increase in urinary thiamine excretion secondary to diuretic therapy were the main contributing factors to this outcome. Although it was not significant, there was an increase in thiamine levels on the second day of hospitalization in patients with RF. This may be associated with impaired renal function in these patients due to acute phase of disease in the early period of hospitalization. On the other hand, thiamine levels in patients who needed hemodialysis were significantly decreased during hospital stay in our study. This observation is in accordance with the previous findings of Heinz et al.22 and Jankowska et al.23
In the study of Brady et al.,24 it was found that HF patients appeared more likely to have evidence of thiamine deficiency. Seligmann et al.4 showed that long-term high-dose furosemide treatment has been shown to induce clinically significant thiamine deficiency in an elderly HF patient population. Lubetsky et al.’s study findings suggest that diuretic-induced thiamine deficiency may occur not only in HF patients undergoing long-term furosemide therapy but also in other patient groups using other diuretics or experiencing polyuric states.18 But, furosemide therapy did not influence the blood thiamine level in Yue et al.’s study in which the included HF patients were treated with furosemide.6 The reason for this difference in thiamine status between studies may be related to renal function of patients. In the study of Yue et al., there was no information about the renal functions of the patients.
Nazmi et al. did not find a significant difference in red cell thiamine pyrophosphate concentration comparing older adult inpatients who were taking furosemide and found no relationship between thiamine concentration and furosemide dose.25 In Nazmi et al.’s study, there was a weak relationship between glomerular filtration rate and thiamine concentration, those with higher glomerular filtration rate had lower erythrocyte thiamine pyrophosphate concentration. These results support our findings that preserved renal function was needed for furosemide-induced thiamine deficiency.
Thiamine deficiency has been closely linked with cardiovascular disease. In this study, we also examined the cardiovascular effects of thiamine deficiency in hypervolemic patients at the time of hospitalization. But, we did not find significant difference in echocardiographic findings of patients with low thiamine levels. This result may be related to the lower percentage of patients with thiamine deficiency compared to the literature and related to the fact that echocardiographic evidence of thiamine deficiency is not apparent until deficiency is severe. On the other hand, there are some studies with conflicting results regarding the use of thiamine in heart failure treatment. In Smithline et al.’s study, the administration of thiamine did not improve dyspnea in acute heart failure patients.26 However, Schoenenberger et al. showed a significant improvement in ejection fraction with thiamin treatment in chronic stable heart failure patients.27 Additional studies are needed to understand the cardiac effects of thiamine.
Our study has several limitations. First, the number of patients was relatively small. Second, we did not evaluate the daily urine output of patients and did not measure urinary thiamine levels. Third, we used a HPLC method to determine whole blood thiamin levels and it may not fully reflect thiamine deficiency. There are more sensitive methods like erythrocyte thiamin pyrophosphate assay that show state of thiamine deficiency. Fourth, RF and HF are two conditions that can often accompany each other and it can be difficult to distinguish one from the other in hypervolemic patients in some cases.
In conclusion, we report that thiamine substantially decreases in most hypervolemic patients receiving intravenous furosemide treatment during the hospital stay. The quantity of this decrease was associated with etiology of hypervolemia. Thiamine levels were significantly decreased with furosemide treatment in especially HF patients, but the decrease in thiamine levels did not detected at the same rate in RF patients. Also, thiamine deficiency at hospital admission was present in most patients receiving chronic oral diuretic therapy for HF. But this was not the case for RF patients receiving chronic oral diuretic therapy. These results suggest that diuretic-induced thiamine loss may be less likely in RF patients, probably due to a reduction in excretion. Thiamine therapy cannot yet be recommended for all patients treated with furosemide, more clinical trials are needed. Our study presents a new perspective about the association between furosemide treatment and thiamine deficiency.
Financial disclosureNone declared.
Conflict of interestThe authors have no conflicts of interest to declare.



