












Cognitive impairment is defined as a newly appeared deficit in at least two areas of cognitive functions, including disturbances in memory, executive functioning, attention or speed of information processing, perceptual motor abilities, or language. Cognitive impairment is highly prevalent in ESRD patients when compared with the general population. It has also been associated with a decreased quality of life. Cognitive functions in patients with ESRD showed improvement with dialysis and renal transplantation. These findings illustrate the potential importance of evaluating and comparing the effects of hemodialysis and transplantation regarding cognitive performance and thus quality of life in ESRD patients and normal subjects. This study was carried out in 100 patients (50 ESRD patients on regular hemodialysis for at least 6 months and 50 post-transplant patients who had maintained successful kidney graft for at least 3 months). All patients underwent laboratory and psychometric scoring tests, including trail making test part A, trail making test part B, digit span, and mini-mental state examination. Thirty healthy adults matched by age and sex served as a control group. The results showed significant differences in cognitive function tests results between transplant and hemodialysis patients (P<0.01), suggesting that transplant patients were superior in their cognitive performance, with the correction of anemia being the most important factor for improving cognitive performance in both groups. There were no significant differences between transplant patients and control subjects in psychometric measures (P>0.05).
ConclusionRenal transplantation as a modality of treatment, in ESRD patients, is superior to hemodialysis in terms of cognitive performance improvement.
El deterioro cognitivo se define como un déficit de nueva aparición en al menos dos áreas de las funciones cognitivas, incluidas las alteraciones de la memoria, la función ejecutiva, la atención o la rapidez de procesamiento de la información, las capacidades motoras perceptivas o el lenguaje. El deterioro cognitivo tiene una prevalencia elevada en los pacientes con ERT en comparación con la población general. También se ha asociado a una reducción de la calidad de vida. Las funciones cognitivas de los pacientes con ERT mostraron una mejoría con la diálisis y con el trasplante renal. Estas observaciones ilustran la posible importancia de la evaluación y comparación de los efectos de la hemodiálisis y el trasplante sobre la función cognitiva y, por tanto, sobre la calidad de vida, en relación con los pacientes con ERT y los individuos normales. El estudio se llevó a cabo en un total de 100 pacientes (50 pacientes con ERT en hemodiálisis regular durante un mínimo de 6 meses y 50 pacientes trasplantados que habían mantenido un buen funcionamiento del injerto renal durante un mínimo de 3 meses). En todos los casos se realizaron análisis de laboratorio y tests psicométricos como el test del trazo (trail making test) parte A, el test del trazo parte B, el test de memoria inmediata de números (digit span) y la mini mental state examination, y se compararon con los de 30 adultos sanos igualados en cuanto a edad y sexo, que se utilizaron como grupo de control. Los resultados pusieron de manifiesto diferencias significativas en los tests de función cognitiva entre los pacientes trasplantados y los hemodializados (p<0,01), y sugirieron que los pacientes trasplantados obtenían mejores resultados de función cognitiva y que la corrección de la anemia era el factor más importante en esa mejora en ambos grupos. No hubo diferencias significativas entre los pacientes trasplantados y los individuos de control por lo que respecta a los parámetros psicométricos (p>0,05).
ConclusiónEl trasplante renal como modalidad de tratamiento, en los pacientes con ERT, es superior a la hemodiálisis por lo que respecta a la mejora de la función cognitiva.
Cognitive impairment is defined as a new deficit in at least two areas of cognitive functioning. These may include disturbances in memory (learning or recalling new information), executive functioning (e.g., planning, reasoning), attention or speed of information processing (e.g., concentration, rapidity of assimilating or analyzing information), perceptual motor abilities (e.g., integrating visual, tactile, or auditory information with motor activities), or language (e.g., word-finding difficulties, reduced fluency).1 Cognitive impairment is a well-recognized manifestation of uremia.2 The severity of kidney disease is associated with the severity of cognitive impairment, independent of age, education and other key confounders.3 In hemodialysis patients, the prevalence of cognitive impairment has been estimated at 30–60% at least twice the values observed in age-matched controls.4 Diagnosis of cognitive impairment is important as cognitive impairment and dementia are associated with an increased risk of death in dialysis patients.1 Recent data in this regard suggest that individuals at all stages of CKD may have a higher risk of developing dementia and cognitive impairment than those without CKD.4 Cognitive function in patients with ESRD has improved with renal transplantation.2 Studies on outcomes after transplantation have traditionally measured post-operative survival and complication rates. One area that has received less attention is the impact of dialysis and transplantation on neuropsychological functioning.5
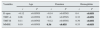
Materials and methodsThis cross-sectional design study was conducted on (100) Egyptian patients as well as (30) healthy subjects (control group) matched as regards age, sex and education. The patients were classified into two groups. Group I: Included (50) ESRD patients on regular hemodialysis, thrice weekly, 4h for each session. All patients were on regular HD for at least 6 months. This interval was to ensure enough time for maintenance HD to correct and avoid uremic complications. Group II: Included (50) post renal transplantation patients who had maintained successful kidney graft for at least 3 months duration. This interval was to ensure some distance from potential early post-operative complications and to allow some time for adjustment of the transplant and immunosuppressive regimen. We excluded from the study patients with evident cerebrovascular disease, thyroid disease, severe anemia, uncontrolled hypertension, malnutrition, major psychiatric illness, major visual or hearing impairment, unstable coronary heart disease, collagen vascular disease and vasculitis. All the medications were revised to exclude any drugs that might have an effect on the cognitive function except steroids and cyclosporine in all transplantation patients group. We obtained history, clinical examination and laboratory investigations from all the patients. Psychometric tests were done on the dialysis off day, which included trail making test part A (TMT-A) that requires participants to connect 25 randomly arranged numbers in the proper order, trail making test part B (TMT-B), which requires that the subject connects with lines in a given sequence circled digits and letters randomly distributed on a page as shown in Fig. 1. The prescribed sequence is from 1 to A to 2 to B to 3 to C, etc., and performance is scored in terms of time to complete the task correctly. The TMT-B assesses attention, visual scanning, psychomotor speed and ability to sequence to shift the cognitive set.6 The digit span (D-span) psychometric test is a widely used auditory verbal short-term (working) memory test. It requires the subject to repeat a spoken string of digits, two trials each, for stings three to nine digits in the forward order and two to eight digits in the reverse order.7 The psychometric mini-mental state examination as shown in Table 1 is a widely used well validated screening tool for cognitive impairment. It tests five areas of cognitive function; the first area includes orientation, which is assessed by asking the usual questions about time, day, date and location; the second area includes registration, which is actually a short term memory test where the subject must recall three objects named by the examiner; the third and fourth area include attention and calculation, which are measured by having the subject begin with the number 100 and count backwards by seven (serial 7s); then, recall by which the subject must recall the three objects named previously. Finally, language functions are assessed by having the subject name simple objects, repeat a sentence and follow a three-stage command. A constructional task is also included in the language section where the subject must copy overlapping pentagons. Each discrete subtask completed correctly earns one point toward a maximum score of 30. The mild cognitive impairment score ranges between 26 and 28, moderate cognitive impairment score between 18 and 25 and severe impairment below 18.12.8
Mini-mental state examination.
| Item | Maximum score |
|---|---|
| Orientation | |
| What is the (year) (season) (date) (month)? | 5 |
| Where are we (state) (country) (town) (hospital) (floor)? | 5 |
| Registration | |
| Name three objects: 1s to say each. Ask the patients for all three. Give 1 point for each correct answer. Repeat them until all three can be repeated | 3 |
| Attention and calculation | |
| Serial subtraction of 7.1 point for each correct. Stop after five answers. Alternatively: Spell “world” backwards | 5 |
| Recall | |
| Ask for the three objects repeated above. 1 point for each correct | 3 |
| Language | |
| Name a pencil and a watch | 2 |
| Repeat the following: “No ifs, ands or buts” | 1 |
| Follow a three-stage command: “Take a paper in your right hand, fold it in half and put into the floor” | 3 |
| Read and obey the following: “Close your eyes” | 1 |
| Write a sentence | 1 |
| Copy a design of two intersecting pentagons | 1 |
The statistical analysis of data was performed by using excel program and the statistical package for social science (SPSS) program version 10. The description of the data done was written in the form of the mean (±) SD for quantitative data. The analysis of the data was done to test statistically significant difference between groups, where P-value less than 0.05 was considered as significant. For quantitative data, Student's t-test was used to compare the two groups and paired sample t-test was used to compare one group at different measurements. One way analysis of variance (ANOVA) test with post hoc analysis was used to compare more than two groups. To test the association between variables, Pearson correlation co-efficiency test was used.
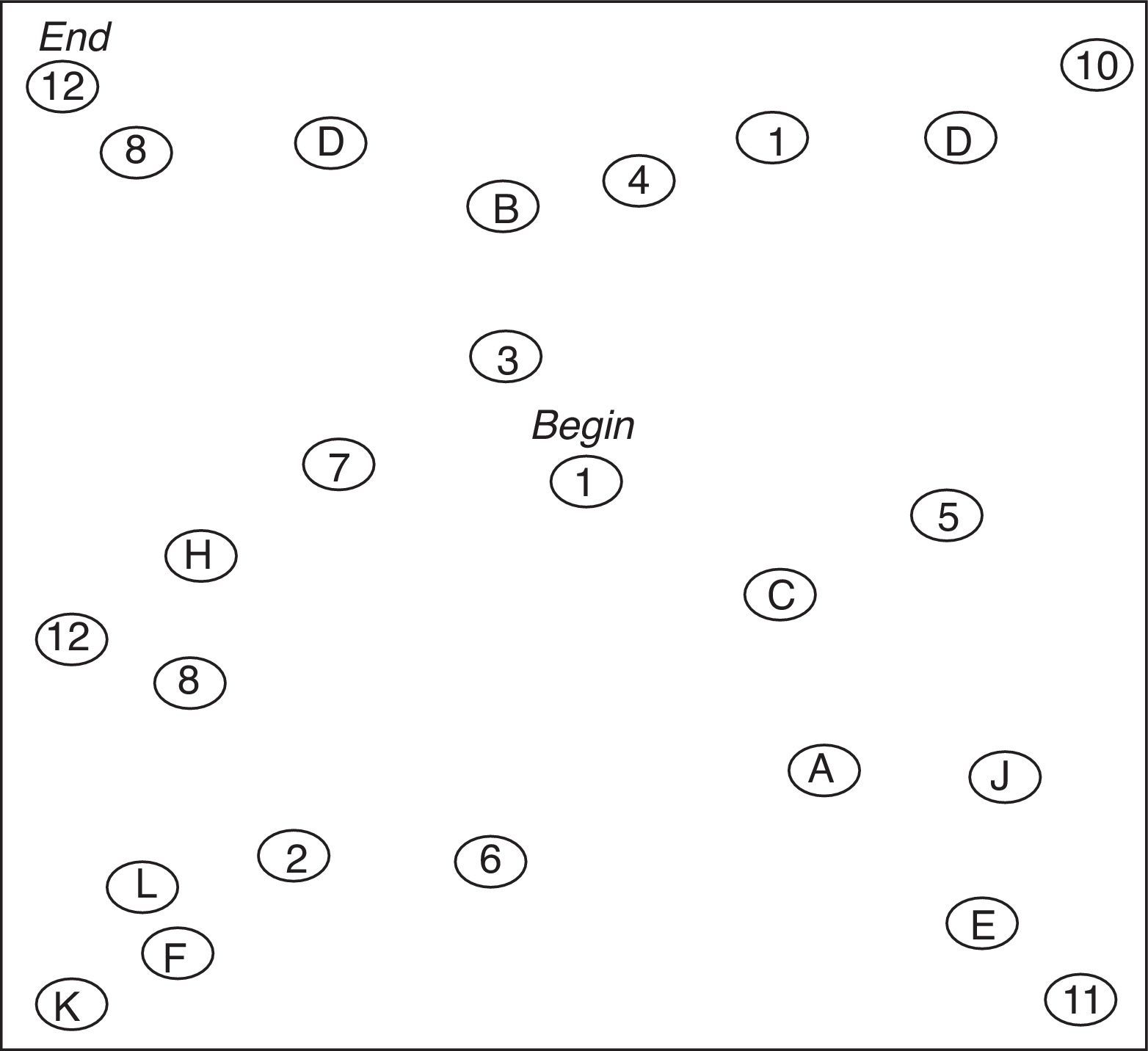
ResultsThis study included 100 patients in addition to 30 healthy controls, 60% males and 40% females with a median age of 45 years and a range from 22 to 60 years, and the mean of the education period was 8.14±3.5 years. There were no significant differences in the gender, median age and education years among the different study groups or controls. Table 2 showed no significant difference could be detected between group I and group II as regard albumin, calcium and phosphorous, on other hand there was significant difference as regard hemoglobin levels. Table 3 showed that transplantation group had better cognitive performance than ESRD patients. Group II had a higher values of d-span, while TMT-A & B were higher among group I with highly statistically significant difference in between by using unpaired t-test. Table 4 showed that ESRD patients had cognitive impairment when compared to control group, but in Table 5 we can see that transplantation group perform as normal as control group as no statistically significant difference could be detected between both groups as regard psychometric measures by using unpaired t-test. Also Fig. 2 showed that transplantation group had equal cognitive performance to control group. And both had better cognitive function when compared to ESRD patients. In Table 6 we can see that in group I there was no statistically significant correlation between psychometric measures versus age, duration, and URR, on the other hand there was significant correlation between psychometric measures and hemoglobin levels. As regards transplantation group there was significant positive correlation between duration versus MMSE and between hemoglobin levels versus psychometric measures by using correlation co-efficient test. On the other hand, no statistically significant correlation was found between other psychometric measures versus age and duration as shown in Table 7. In group II, no significant correlation was found between cyclosporine level and psychometric measures.
Comparison between group I versus group II as regard psychometric tests.
| Variables | Group IN=50 | Group IIN=50 | t | P |
|---|---|---|---|---|
| D-span | 3.9±1.5 | 7.5±1.5 | 7.7 | <0.01 |
| TMT-A | 97±41 | 33.7±8 | 10 | <0.01 |
| TMT-B | 194±72 | 110±28.6 | 7.6 | <0.01 |
| MMSE | 28.4±7 | 30±1.3 | 1.1 | >0.05 |
Bold: these values are significant values to differentiate them from non significant values.
Correlation between psychometric tests versus each other and versus other variables among group I.
| Variables | Age | Duration | Hemoglobin | URR | ||||
|---|---|---|---|---|---|---|---|---|
| r | P | r | P | r | P | r | P | |
| D-span | −0.02 | >0.05 | −0.04 | >0.05 | 0.3 | <0.05 | 0.17 | >0.05 |
| TMT-A | 0.07 | >0.05 | 0.10 | >0.05 | 0.32 | <0.05 | 0.2 | >0.05 |
| TMT-B | 0.15 | >0.05 | −0.09 | >0.05 | 0.39 | <0.05 | 0.08 | >0.05 |
| MMSE | 0.09 | >0.05 | 0.14 | >0.05 | 0.45 | <0.05 | 0.25 | >0.05 |
Correlation between psychometric tests versus each other and versus other variables among group II.
| Variables | Age | Duration | Hemoglobin | |||
|---|---|---|---|---|---|---|
| r | P | r | P | r | P | |
| D-span | −0.12 | >0.05NS | −0.14 | >0.05NS | 0.4 | <0.05S |
| TMT-A | 0.06 | >0.05NS | 0.16 | >0.05NS | 0.32 | <0.05S |
| TMT-B | 0.11 | >0.05NS | −0.12 | >0.05NS | 0.39 | <0.05S |
| MMSE | 0.19 | >0.05NS | 0.36 | <0.05S | 0.33 | <0.05S |
Cognitive declines are seen in end-stage renal disease (ESRD) in patients on chronic hemodialysis. Several studies have shown elevated risk of dementia in patients with ESRD. However, modest cognitive declines appear to begin prior to the point where mild or modest kidney disease has progressed to ESRD. There is evidence that the rate of cognitive decline is associated with deterioration in kidney function.9 Kidney transplantation (TX) is considered to be the preferred treatment for end-stage renal disease (ESRD). Studies on outcomes after TX have traditionally measured post-operative survival and complication rates. One area that has received less attention is the impact of dialysis and TX on neuropsychological (NP) functioning. This area deserves attention as cognitive capacity is intimately connected to outcomes such as activities of daily living and social and vocational adjustments, and has also been found to be an independent predictor of mortality.5 Our study focused on evaluating cognitive functions in ESRD on regular hemodialysis with URR>60% and transplantation patients, who were followed till their renal functions stabilized. There were marked cognitive impairment among ESRD patients on regular HD when compared to control group as shown in Table 4 (P<0.01). This was in agreement with other studies.10,11 There were highly significant differences between hemodialysis patients and transplantation groups as regards mean values of cognitive function tests score as shown in Table 3 (P<0.01). Other study5 emphasized our finding and demonstrated improvements in cognition following kidney transplantation also it showed that there was no significant cognitive impairment in transplantation group as compared with control group (P>0.05), which emphasized our finding as shown in Table 5. Also, in our study there was significant correlation between hemoglobin level and cognitive function tests in HD patients as shown in Table 6 (P<0.05) and this was in agreement with the studies of other investigators.7,12 Finally, In our study, there were no significant correlation between cyclosporine trough level and psychometric tests among transplantation patients as shown in Table 8. Limitations of our study included: (1) Not all possible parameters were included such as dietary habits, atherosclerosis, genetic factors, peritoneal dialysis, different age and ethnic groups, medications and immunosuppression drugs and their use for longer durations. Further investigations including important different confounders are required. (2) This was a cross-sectional study; thus, associations between hemodialysis and cognitive impairment suggest, but do not provide evidence for a causal relation. It is necessary to conduct a longitudinal study for longer durations to clarify the reason for impaired cognition in hemodialysis patients proving that hemodialysis is a sure independent risk factor for cognitive impairment. In conclusion, in our study we found marked cognitive impairment in HD population when compared to both transplantation and control groups. This high prevalence of cognitive impairment among hemodialysis patients has adverse implications for hospitalization and reduced life expectancy. Therefore, cognitive impairment in hemodialysis patients should be routinely monitored carefully and treated in an appropriate manner. Renal transplantation as a modality of treatment, in ESRD patients, is superior to hemodialysis in terms of improving cognitive performance.
Conflict of interestThe authors declare no conflict of interest.



