






Glomerular filtration rate (GFR) is a useful index in many clinical conditions. However, very few studies have assessed the performance of full age spectrum (FAS) equation and the Asian modified Chronic Kidney Disease-Epidemiology Collaboration (CKD-EPI) equation in the approximation of GFR in Chinese patients with chronic kidney disease.
ObjectiveThis study aimed to compare the diagnostic performance of the above two creatinine-based equations.
MethodsA well designed single-center cross-sectional study was performed and the GFR was determined by 3 methods separately in the same day: technetium-99m-diethylene triamine pentaacetic acid (99mTc-DTPA) dual plasma sample clearance method (mGFR); FAS equation method; Asian modified CKD-EPI equation method. The gold standard method was the mGFR. Equations performance criteria considered correlation coefficient, bias, precision, accuracy and the ability to detect the mGFR less than 60ml/min/1.73m2.
ResultsA total of 160 patients were enrolled. The diagnostic performance of FAS showed no significant difference in the correlation coefficient (0.89 vs 0.89), precision (15.9 vs 16.1ml/min/1.73m2), accuracy (75.0% vs 76.3%) and the ability to detect the mGFR less than 60ml/min/1.73m2 (0.94 vs 0.94) compared with the Asian modified CKD-EPI equation in all participants. The FAS showed a negative bias, while the new CKD-EPI equation showed a positive bias (−1.20 vs 1.30ml/min/1.73m2, P<0.001). However, they were all near to zero. In the mGFR<60ml/min/1.73m2 subgroup and mGFR>60ml/min/1.73m2 subgroup were consistent with that in the whole cohort. The precision and accuracy decreased when GFR>60ml/min/1.73m2 in both equations.
ConclusionsThe FAS equation and the Asian modified CKD-EPI equation had similar performance in determining the glomerular filtration rate in the Chinese patients with chronic kidney disease. Both the FAS equation and Asian modified CKD-EPI can be a satisfactory method and may be the most suitable creatinine-based equation.
La tasa de filtración glomerular (TFG) es un índice útil en muchas condiciones clínicas. Sin embargo, muy pocos estudios han evaluado el rendimiento de la ecuación FAS (full age spectrum) y la ecuación CKD-EPI (Chronic Kidney Disease-Epidemiology Collaboration) modificada para Asia en la aproximación de TFG en pacientes chinos con enfermedad renal crónica.
ObjetivoEl objetivo de este estudio fue comparar el rendimiento diagnóstico de las dos ecuaciones anteriores basadas en creatinina.
MétodosSe realizó un estudio transversal unicéntrico y bien diseñado, calculándose separadamente la TFG mediante tres métodos en el mismo día: método mGFR (aclaramiento de muestra de plasma dual con 99mTc-DTPA [tecnecio-99m marcado con triamina dietileno de ácido pentaacético]), el método de ecuación FAS y el de ecuación CKD-EPI modificada para Asia. El método de referencia fue mGFR. Los criterios de rendimiento de las ecuaciones consideraron coeficiente de correlación, sesgo, precisión, exactitud y capacidad de detectar un valor de mGFR inferior a 60 mL/min/1,73 m2.
ResultadosSe incluyó un total de 160 pacientes. El rendimiento diagnóstico de FAS no reflejó diferencia significativa en cuanto a coeficiente de correlación (0,89 vs. 0,89), precisión (15,9 vs. 16,1 mL/min/1,73 m2), exactitud (75 vs. 76,3%) y capacidad de detectar un valor de mGFR inferior a 60 mL/min/1,73 m2 (0,94 vs. 0,94) en comparación con la ecuación CKD-EPI modificada para Asia, en todos los participantes. La ecuación FAS reflejó un sesgo negativo, mientras que la nueva ecuación CKD-EPI reflejó un sesgo positivo (-1,20 V vs.1,30 mL/min/1,73 m2, p < 0,001). Sin embargo, todos los valores se aproximaron a cero. En el subgrupo mGFR < 60 mL/min/1,73 m2 y el subgrupo mGFR > 60 mL/min/1,73 m2 los valores fueron consistentes con respecto a la cohorte total. La precisión y exactitud se redujeron cuando TFG > 60 mL/min/1,73 m2 en ambas ecuaciones.
ConclusionesLa ecuación FAS y la ecuación CKD-EPI modificada para Asia reflejaron un desempeño similar a la hora de determinar la tasa de filtración glomerular en los pacientes chinos con enfermedad renal crónica. Ambos pueden ser métodos satisfactorios y las ecuaciones más idóneas basadas en creatinina.
Chronic kidney disease (CKD) has been considered as a public health problem worldwide.1–4 The glomerular filtration rate (GFR) is valuable for the diagnosis, classification, management, monitoring the therapeutic effect and predicting the prognosis in the CKD patient.5–7 Unfortunately, GFR cannot be obtained accurately and simply. The inulin clearance rate, the golden standard for determining GFR, is not simple and cannot be applied routinely. As an alternative, several available methods were developed to evaluate GFR.8–15 These methods are much more convenient and less costly than the golden method. The GFR-estimating equations have been recommended as noninvasive alternatives.16 Among the equations, the creatinine-based equations were widely used because of the simple and practicable procedure. The most popular creatinine-based equations for estimating GFR are modified diet in renal disease (MDRD) equation and chronic kidney disease epidemiology collaboration (CKD-EPI) equation. The CKD-EPI equation developed in 2009 is widely used to evaluate the GFR and may be more accurate than the other equations; however, this equation did not refer to the racial variation.17–19 The researchers developed a modified CKD-EPI equation that included a four-level race variable10 including the Asian race. Our previous study showed that the Asian modified CKD-EPI equation lead to more accurate GFR estimation than the original one in Chinese patients with CKD.20 A new equation, full age spectrum (FAS) equation, was developed in 2016, which can be applicable to all ages.8 Our previous study revealed that the FAS equation was valid in the approximation of GFR in Chinese patients with CKD.21
We hypothesized whether both equations are equal in performance in a Chinese population with chronic kidney disease. Here, a well-designed cross-sectional study was set up in this study to compare the performance of the FAS equation and the Asian modified CKD-EPI equation.
Materials and methodsEthics statementThe study protocol was approved by Hebei Medical University ethical committee (NO. 2017-027-1), and the written informed consent was obtained from each participant.
PatientsThose subjects with the following criteria were identified and enrolled in the study: (1) Chinese patients; (2) at least 18 years of age; (3) the participants met the diagnostic standard for CKD.22 Patients with acute kidney function deterioration, edema, cardiac insufficiency, pleural or abdomen effusion, disabled limb, and treated with cimetidine or trimethoprim or replacement therapy were excluded.17,23–24 The patients were categorized into 2 subgroups based on the GFR calculated by reference method: lower-GFR subgroup (mGFR <60ml/min/1.73m2) and higher-GFR subgroup.
(mGFR>60ml/min/1.73m2).
The GFR measurement by dual plasma sample clearance method (mGFR)The 99mTc-diethylene triamine pentaacetic acid (99mTc-DTPA) dual plasma sample clearance method was employed as the reference method. The main procedure was collecting the blood sample 2 and 4h after the 99mTc-DTPA injection. And then we measured the radioactivity of the blood sample immediately. The mGFR was calculated from a single exponential formula. The detailed procedure was described previously.17,23
The measurement of serum creatinineThe blood samples were collected between 6:30 and 8:00a.m. and then the blood samples were transferred to the laboratory within 2h. The blood samples were analyzed after they were centrifuged at 3000rpm for 15min. All the staffs in the laboratory underwent the same training and operated the biochemical analyzer according to the standard operation procedure. The serum creatinine (Scr) was automatically measured by the enzymatic IDMS-traceable method using a biochemical analyzer (VITROS 5.1, Johnson Company, USA; reagents from the same company).
GFR measurement by FAS equation (eGFR-FAS)The FAS equation was as follows8:



Q-values are the mean or median Scr value for age-/sex-specific healthy populations.10 The units of Scr and age were mg/dL and year respectively.
GFR measurement by Asian modified CKD-EPI equation (eGFR-CKD-EPI)The Asian modified CKD-EPI equation is as follows10:
Female with the concentration of serum creatinine≤0.7mg/dl,

Female with the concentration of serum creatinine≥0.7mg/dl,

Male with the concentration of serum creatinine≤0.9mg/dl,

Male with the concentration of serum creatinine≥0.9mg/dl,

The unit of Scr and age was mg/dL and year respectively.
Statistical analysisAll Statistical analyses were performed using SPSS (version 17.0, SPSS. Chicago IL, USA) and Medcalc (version 4.3, Medcalc software, Mariekerke, Belgium). The normal distribution data was expressed by means of mean and standard deviation. The non-normal distribution data was expressed as median and interquartile range (M(QR)). The parameters of bias, precision, and accuracy were employed to compare the performance of the eGFR-FAS and eGFR-CKD-EPI. Bias was defined as eGFR minus mGFR. The standard deviation of the bias was considered as precision. The percentage of eGFR within 30% deviation of mGFR (P30) was employed as accuracy. The association between mGFR and eGFR was analyzed by means of the correlation analysis using the coefficient of Pearson. Wilcoxon Z test, F test were used to compare the bias, precision, accuracy and correlation coefficient. The receiver operating characteristic (ROC) curve illustrated the diagnostic ability for detecting the mGFR<60ml/min/1.73m2 of the two equations and the Z-test was employed to compare the area under curve (AUC).
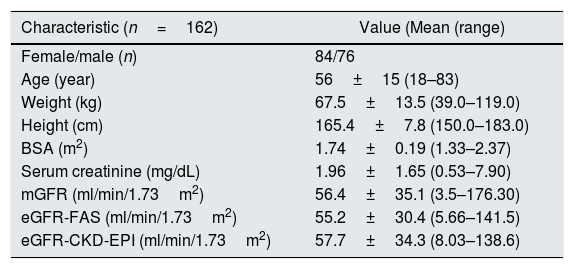
ResultsParticipants’ characteristicsA total of 160 patients (mean age 56±15 years) were enrolled in this study, including 76 males and 84 females. The values of serum creatinine, and mGFR were 1.96±1.65mg/dL, and 56.4±35.1ml/min/1.73m2, respectively. The eGFR-FAS and the eGFR-CKD-EPI were 55.2±30.4 and 57.7±34.3ml/min/1.73m2, respectively. The range that the values reached with the eGFR equations were less than those shown with mGFR. The mGFR reached 176.3ml/min/1.73m2 while eGFR-FAS only was 141.5ml/min/1.73m2. With eGFR-CKD-EPI it reached 138.6ml/min/1.73m2. A wide variety of clinical diagnoses led to chronic kidney disease were included in the study including chronic glomerulonephritis in 52 cases, diabetic nephropathy in 36 cases, chronic pyelonephritis in 30 cases, hypertensive nephropathy in 21 cases and other causes or unknown causes in the remaining 23 cases. The basic characteristics of the patients are shown in Table 1.
The characteristics of the patients.
| Characteristic (n=162) | Value (Mean (range) |
|---|---|
| Female/male (n) | 84/76 |
| Age (year) | 56±15 (18–83) |
| Weight (kg) | 67.5±13.5 (39.0–119.0) |
| Height (cm) | 165.4±7.8 (150.0–183.0) |
| BSA (m2) | 1.74±0.19 (1.33–2.37) |
| Serum creatinine (mg/dL) | 1.96±1.65 (0.53–7.90) |
| mGFR (ml/min/1.73m2) | 56.4±35.1 (3.5–176.30) |
| eGFR-FAS (ml/min/1.73m2) | 55.2±30.4 (5.66–141.5) |
| eGFR-CKD-EPI (ml/min/1.73m2) | 57.7±34.3 (8.03–138.6) |
Abbreviations: CKD, chronic kidney disease; mGFR, the GFR measured by the 99mTc-DTPA dual plasma clearance rate method; eGFR-FAS, the GFR estimated by the FAS equation; eGFR-CKD-EPI, the GFR estimated by the Asian modified CKD-EPI equation.
The scatter plots showed both eGFR-FAS and eGFR-CKD-EPI were highly associated with mGFR, and the correlation coefficients were 0.89 (P<0.001) and 0.89 (P<0.001). The linear regression was therefore constructed and the regression equations of eGFR-FAS and mGFR was eGFR-FAS=11.56+0.78mGFR (P<0.001). The regression equations of eGFR-CKD-EPI and mGFR was eGFR-CKD-EPI=9.32+0.87mGFR (P<0.001) (Figs. 1 and 2). Indeed, there was a close relationship between eGFR-FAS and Scr both in men and women (Fig. 3). Bland–Altman plots for the agreement of eGFR-FAS and eGFR-CKD-EPI against mGFR are depicted in Fig. 4. The limit of agreement for the eGFR-FAS and eGFR-CKD-EPI was 61.9 and 63.3ml/min/1.73m2, respectively. There was a tendency of both the equations to make greater errors when the values of mGFR were higher.




The Bland–Altman plots of difference versus mGFR in patients with CKD about the two equations. The mGFR are given on the X axis, and the difference of eGFR and mGFR is given on the Y axis. The solid long lines show mean difference and the dotted long lines represent the 95% limits of agreement. Abbreviations: eGFR-FAS-GFR: estimated by the FAS equation; eGFR-CKD-EPI-GFR: estimated by the Asian modified CKD-EPI equation.
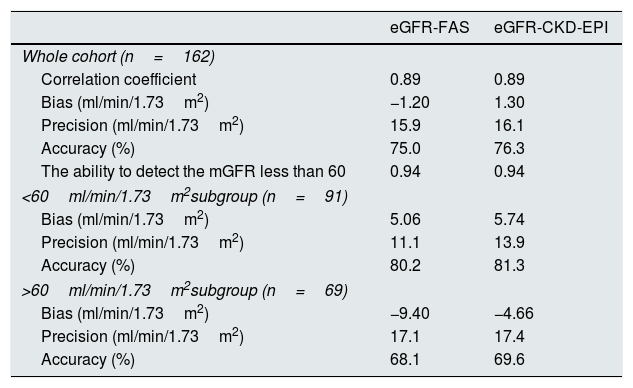
In the whole cohort, the bias of eGFR-FAS and eGFR-CKD-EPI was −1.20ml/min/1.73m2 and 1.30ml/min/1.73m2 respectively. There was significant difference in the performance of bias (Z=−10.97, P<0.001). The precision of eGFR-FAS was not significantly lower than that of eGFR-CKD-EPI (15.9ml/min/1.73m2 vs 16.1ml/min/1.73m2; F=1.025, P=0.875). The eGFR-FAS and the eGFR-CKD-EPI also revealed the similar performance of accuracy (75.0% vs 76.3%, P=0.424). Regarding the correlation coefficient, the FAS equation did not have a superior performance compared with the Asian modified CKD-EPI equation (0.89 vs 0.89, Z=−0.087, P=0.930).
The AUCs of were 0.94 (0.90–0.97) for FAS equation, 0.94 (0.90–0.97) for Asian modified CKD-EPI equation. There were no significant differences in the abilities (AUCs) of the equations to detect the mGFR less than 60ml/min/1.73m2 (Z=0.221, P=0.825) (Fig. 5). When the sensitivity and specificity were most satisfactory, the cut-off value of eGFR-FAS was 60.8ml/min/1.73m2 (sensitivity: 92.3%; specificity: 82.6%) and the cut-off value of eGFR-CKD-EPI was 60.3ml/min/1.73m2 (sensitivity: 84.6%; specificity: 92.8%).

The performance of bias, precision and accuracy in the mGFR<60ml/min/1.73m2 subgroup and mGFR>60ml/min/1.73m2 subgroup were consistent with that in the whole cohort. (The comparison of the two equations is shown in Table 2.)
The comparison between eGFR-FAS and eGFR-CKD-EPI.
| eGFR-FAS | eGFR-CKD-EPI | |
|---|---|---|
| Whole cohort (n=162) | ||
| Correlation coefficient | 0.89 | 0.89 |
| Bias (ml/min/1.73m2) | −1.20 | 1.30 |
| Precision (ml/min/1.73m2) | 15.9 | 16.1 |
| Accuracy (%) | 75.0 | 76.3 |
| The ability to detect the mGFR less than 60 | 0.94 | 0.94 |
| <60ml/min/1.73m2subgroup (n=91) | ||
| Bias (ml/min/1.73m2) | 5.06 | 5.74 |
| Precision (ml/min/1.73m2) | 11.1 | 13.9 |
| Accuracy (%) | 80.2 | 81.3 |
| >60ml/min/1.73m2subgroup (n=69) | ||
| Bias (ml/min/1.73m2) | −9.40 | −4.66 |
| Precision (ml/min/1.73m2) | 17.1 | 17.4 |
| Accuracy (%) | 68.1 | 69.6 |
Abbreviations: eGFR-FAS, GFR estimated by FAS equation; eGFR-CKD-EPI, GFR estimated by Asian modified CKD-EPI equation.
Our previous study revealed that both the Asian modified CKD-EPI equation and the FAS were valid in determining the GFR in Chinese patients with chronic kidney disease, however, we had no knowledge about which method would be more preferable.
To clarify this issue, a well-designed comparative study was set up. In this study, we analyzed the correlation coefficient, bias, precision, accuracy and the capacity for detecting CKD between the FAS equation and the Asian modified CKD-EPI equation with the 99mTc-DTPA dual plasma clearance method as the golden method. The main finding of our study was that the Asian modified CKD-EPI equation and the FAS equation showed no significant difference in determining the GFR in Chinese patients with chronic kidney disease. The most important indexes, correlation coefficient, accuracy and the capacity for detecting CKD of the two equations revealed no difference. Although the two equations showed a positive bias/a negative bias, they were all near to zero and it was considered no clinical difference. According to the results of this study and our previous study, we strongly recommended that the FAS equation and the Asian modified CKD-EPI equation both are the most suitable formula based on the level of serum creatinine to estimate the glomerular filtration rate of the Chinese patients with chronic kidney disease. However, the two equations both work worse in groups with mGFR greater than 60ml/min/1.73m2 with less accuracy and less precision than in patients with mGFR less than 60ml/min/1.73m2.
There were several similar studies aimed to the comparison of FAS equation and CKD-EPI equation in determination of GFR in Chinese patients with chronic kidney disease.25–27 Our study was different from the previous study in two ways. First, the reference method of the previous study was the 99mTc-DTPA renal dynamic imaging or the EPI_Cr_CysC equation.26,27 It should be noted that the 99mTc-DTPA renal dynamic imaging was not so accurate to be the reference method.21,23 The relevant research results would not be reliable otherwise. The EPI_Cr_CysC equation was an empirical equation and there was no recommendation that it could be used as the reference method to determine GFR. Fortunately, the reference method of our study was the 99mTc-DTPA dual plasma clearance method, which was more accurate and widely employed as the golden standard; therefore, the results of our study would be more accurate. Second, this study focused on the equations based on the serum creatinine, while the previous study focused on the equations based on the combination of serum cystatin C and creatinine or cystatin C.25,26 The previous study compared the accuracy of the original CKD-EPI equation and FAS equation but not the Asian modified CKD-EPI equation,27 while our previous study indicated that the modified one was more accurate than the original one.20
The limitation of the present study was that the pediatric patients with CKD were not enrolled. Our future study will be focused on the estimated GFR of Chinese pediatric patients with CKD.
ConclusionsIn conclusion, both the FAS equation and the Asian modified CKD-EPI equation are effective methods to determine the glomerular filtration rate of the chronic kidney disease patients. Neither the FAS equations nor the Asian modified CKD-EPI equation has a superior performance compared with the other one and both of them can be the satisfactory choice in clinical practice.
The glomerular filtration rate (GFR) is a useful index in the management of the chronic kidney disease (CKD) patients. Both the full age spectrum equation and the Asian modified CKD-EPI equation are valid in the approximation of GFR in Chinese patients with CKD, however, it is unclear whether these equations are equal in performance in a Chinese population with CKD. Thus, a cross-sectional study was set up in this study to compare the performance of the FAS equation and the Asian modified CKD-EPI equation. Our results revealed that The FAS equation and the Asian modified CKD-EPI equation had similar performance. Both the FAS equation and Asian modified CKD-EPI can be a satisfactory method and may be the most suitable creatinine-based equation in determining the GFR of the Chinese CKD patients.
This project was partially funded by Natural Science Foundation of Hebei Province (H2020206422).
Conflict of interestThe authors have declared that no conflict of interest exists.



