



The adoration for a “perfect body” has been installed in our society. Between 6 and 10% of the clients of a gym use drugs and hormones to increase performance,1 and in selected populations, such as weightlifters and bodybuilders, the abuse of these substances is much higher, reaching up to 44%.2
The danger is not so much from the substances themselves, but from the way they are used: without medical supervision, making different combinations, and at doses much higher than usual in clinical practice. The real consequences of this abuse are not totally known. Due of this polypharmacy, it is often difficult to determine the specific agent responsible for kidney injury in these patients.
The kidney is one of the organs affected by these practices, and nephrology consultations in this population are becoming more frequent, which requires greater knowledge on the part of the nephrologist about this emerging pathology and a high level of suspicion, since the patient does not always recognize this abuse.
Although it is difficult to know the true dimension of the renal pathology associated with these substances, it is relevant for the nephrologist to know that approximately a 30% of anabolic users develop dependency and, therefore, would be at greater risk of developing the medical consequences of the prolonged use of these substances.3
The objective of this manuscript is not to make a systematic review of the literature but simply to call the attention and increase the knowledge of the nephrologist regarding the substances that are commonly consumed by some athletes, identifying which of them and how can they affect the kidney. This will be useful to interpret the renal injuries and to learn how to advice about the consumption of these type of substances.
Interpretation of the formulas to estimate glomerular filtration rateThe formulas used to estimate glomerular filtration rate (GFR) include levels of serum creatinine and are influenced by muscle mass and dietary intake, particularly by the supply of creatine.4 Creatine spontaneously and irreversibly becomes creatinine, so those who take creatine or have an important muscle mass can be falsely diagnosed of decreased renal function using the current formulas.5 Cystatin C is also influenced by gender, muscle mass, and steroid intake, so it would not bring advantages in this specific population. Although in research work the GFR has been assessed by the clearance of other exogenous substances as inulin or radioactive isotopes (99TmDTPA or 51Cr-EDTA),5 the best alternative in our conditions in this type of population is the use of 24h creatinine clearance.
Hyperproteic dietsIncrease of high-quality protein intake before and after exercise, improves the adaptive response to exercise,6 increase the synthesis of glycogen and proteins, and reduce their degradation.7 Therefore, the International Society of Sports Nutrition in 2007 and 2017 considers safe and adequate a protein intake of 1.4–2.0g/kg/day.8 Subsequent studies conducted in rats9 and in trained humans showed that a high protein intake (2.51–3.32g/kg/day), during one year, did not produce alterations in lipids, liver function or renal function.10,11 However, the reality is that athletes, even amateurs, increase the protein intake to levels higher than recommended, reaching up to 5g/kg/day and for prolonged periods of time.12
The normal physiological response of the kidney to high protein intake is to increase GFR,13 reaching a normal or above normal renal function; these are hyperfiltration states, so called renal functional reserve (RFR). Although these diets may be safe in a trained healthy population, some authors warn about possible dangers, especially in patients with previous kidney disease.14 It is suggested that this permanent challenge of RFR may cause and/or accelerate the deterioration of renal function.15,16 It has been demonstrated an association between high protein intake and worsening of renal function.16
Another risk of the hyperproteic diet is dehydration, by increasing the renal excretion of solutes – urea and other nitrogenous wastes–, which requires greater water consumption, especially if there is diabetes, hypertension or cardiovascular disease. And it is an independent risk factor for the development of kidney stones in predisposed individuals.17 They are also associated with an increased risk of type 2 diabetes due to diets with high acid load.18
Nutritional supplementsSome nutrients used as nutritional supplements such as l-carnitine, choline/phosphatidylcholine, tryptophan and tyrosine, may produce toxic effects in patients with chronic kidney disease (CKD), as they modify the gut microbiota, increasing the number of bacteria that process these compounds into uremic toxins –N-trimethylamine oxide (TMAO), p-cresyl sulfate, indoyl sulfate and indole-3-acetic acid. These toxins are associated with an increased risk of death and cardiovascular disease.19
Creatine is widely used to increase muscle mass and improve athletic performance. It may increase creatinine levels without causing damage to renal function: in trained athletes, creatinine supplementation for 3 months had no detrimental effects on renal function, measured by 51 Cr-EDTA.20 The problem is that, in this context, an elevation of serum creatinine may reflect creatine supplementation or a real kidney damage, and the nephrologist must differentiate both situations by calculating the 24h creatinine clearance.
Anabolic androgenic steroids (AAS)The current extent of the use and adverse effects of anabolic androgenic steroids (EAA) is unknown, but there is a significant hidden consumption by professional and amateur athletes worldwide, including adolescents.21
AAS include testosterone and the numerous synthetic analogs that are modified to increase anabolic effects.22 They are formulated for oral, parenteral administration: intramuscular, subcutaneous, or transdermal injections. They are used in cycles of 6–12 weeks, and then suspended for a long or short period or continue the consumption at a lower dose. Occasionally, they are administered using a pyramidal pattern, starting with a low daily dose at the beginning until the maximum dose is reached, then gradually decreasing it until its withdrawal (Table 1). The amount consumed exceed the therapeutic doses by 10 and 100 times, often combining several preparations, oral and parenteral.
Example of a steroid cycle used in sport.
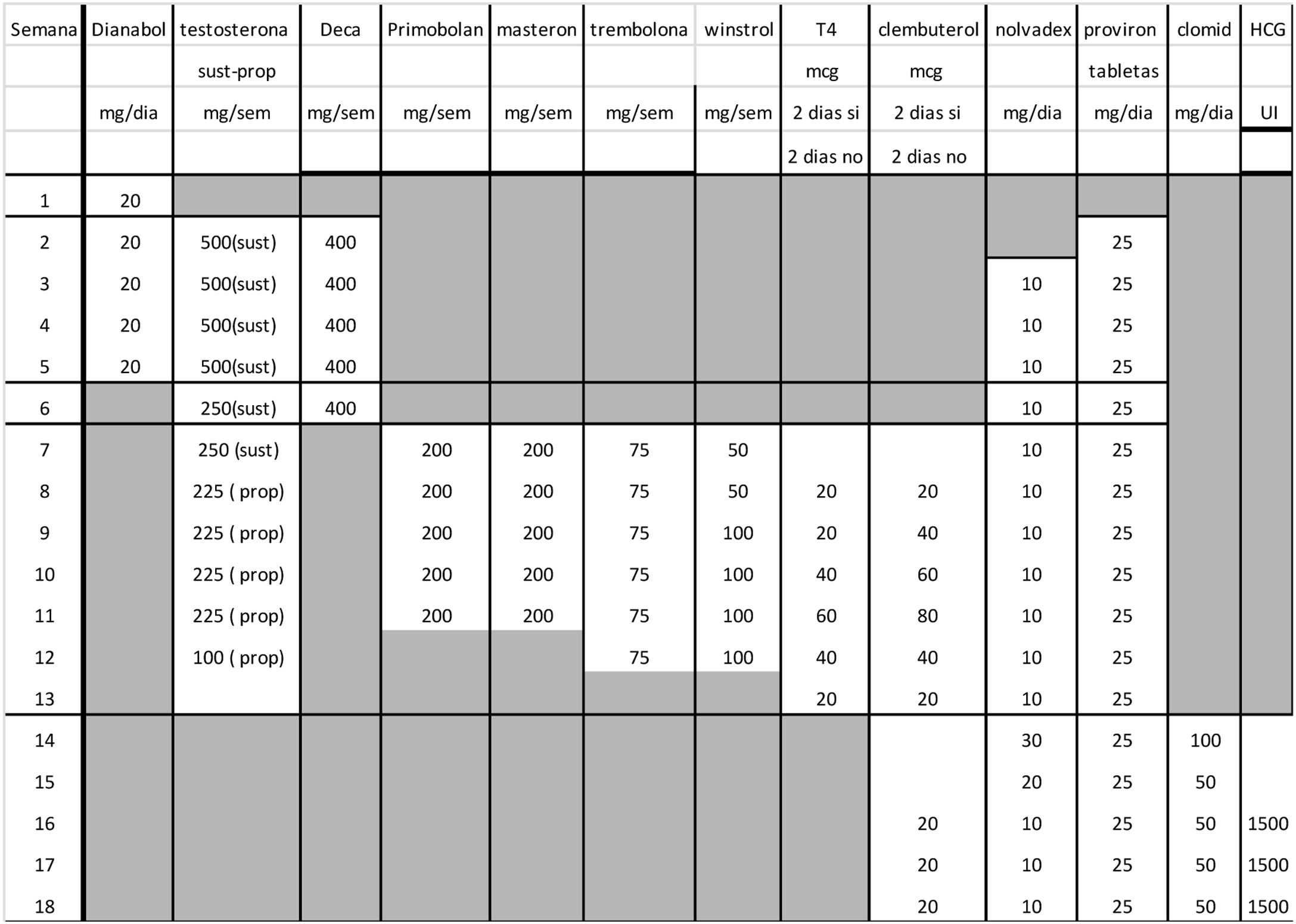
Dianabol: methandrostenolone (oral tablets of 10mg).
Testosterone: (1) sustanon: 400mg/ml (contains a mixture of testosterones: 60mg of testosterone propionate, 110mg of testosterone phenylpropionate, 110mg of testosterone isocaproate and 120mg of testosterone decanoate); intramuscular injection; (2) propionate: testosterone propionate (intramuscular injection of 100mmg/ml).
Deca: nandrolone decanoate (solution for injection of 200mg/ml).
Primobolan: methenolone enanthate (intramuscular solution for injection 10 ampoules of 1ml).
Masteron: drostanolone propionate (injectable solution of 100mg/ml).
Trenbolone: trenbolone acetate (solution 100mg/ml injectable).
Winstrol: stanozolol (oral tablets of 10mg).
T4: levothyroxine sodium (oral tablets of 100μg).
Clenbuterol: clenbuterol (oral tablets of 0.02μg).
Nolvadex: tamoxifen (oral tablets of 20mg).
Provirón: 25mg tablets.
Clomid: clomiphene; 50mg tablets.
HCG: human chorionic gonadotropin; injectable solution in doses of 1500UI.
Source: information extracted from the clinical history of a bodybuilder patient with focal and segmental glomerulonephritis in a nephrology outpatient clinic.
During the last 4 years, there has been a 3 fold increase in liver complications (cholestatic liver disease and cholestatic liver disease) and renal complications (acute biliary nephropathy or biliary nephrosis,23 focal and segmental glomerulosclerosis (FSGS) and tubulointerstitial nephropathy (NTI)) associated with AAS requiring hospitalization even dialysis.24 A recent study conducted in 22 healthy biopsied adults who recognized more than 6 years consumption of high doses of proteins and AAS revealed FSGS in 8 patients, nephroangiosclerosis in 4, chronic interstitial nephritis in 3, acute interstitial nephritis in 2, nephrocalcinosis with interstitial nephritis chronic in 2 and single patients with membranous glomerulopathy, semilunar glomerulopathy and sclerosing glomerulonephritis. Patients with FSGS had a longer duration of exposure, late presentation and worse prognosis, and those with interstitial disease had a shorter exposure and an earlier presentation and the lesions improved or stabilized after the cessation of this practice.25 The fact that FSGS affects bodybuilders after long-term abuse of AAS suggests that AAS are podocytic toxins.26 The levels of testosterone, creatinine, urea and urate increased with the use of these substances.27 The decrease in GFR, the fibrosis and proliferation of renal cells may be due to overexpression of nephrin and podocin genes induced oxidative stress.28
Altered lipid profile, left ventricular hypertrophy and elevated blood pressure in young athletes should suspect the consumption of these substances, since they have a role in the regulation of cardiovascular function: release of nitric oxide (NO), mobilization of calcium, vascular apoptosis, hypertrophy, calcification, senescence and generation of reactive oxygen species.29 The risk of death in chronic users of AAS is 4.6 times higher than in normal population adjusted for age.30
ClenbuterolClenbuterol, a bronchodilator used for the treatment of asthma, is also used for its anabolic properties. Clenbuterol may produce arrhythmias and electrolyte alterations (hypokalemia, hypomagnesemia and hypophosphatemia) that can cause sudden death.31
Exercise rhabdomyolysisTraining reduces the risk of developing rhabdomyolysis, but in the presence of profuse sweating, the lack of adequate water and electrolyte replacement together with a high temperature may affect to even trained athletes, increasing the risk of renal failure. Any healthy person subjected to extreme and strenuous exercise may have an episode of rhabdomyolysis with acute renal failure and dialysis requirements, which have been described even after the first class of spinning.32
ConclusionsA recent systematic search of electronic databases concludes that the literature describing the dietary intake practices of competitive bodybuilders is outdated and often of poor quality33; and for all of this, some authors warn of the risk, and recommend to analyze serum creatinine and proteinuria before starting to consume this type of diet and supplements, since CKD is often silent and patients may be unaware of this condition.34
Physicians and patients should be aware that, in patients with CKD, and even in healthy people, certain practices associated with sports can deteriorate the health.
Please cite this article as: Arenas Jiménez MD. Cuando el deporte deja de ser salud: dietas, suplementos y sustancias para aumentar el rendimiento y su relación con el riñón. Nefrologia. 2019;39:223–226.



