


The Global Burden of Disease (GBD) study measures the health of populations worldwide and by country on an annual basis and aims at helping guide public policy on health issues. The GBD estimates for Spain in 2016 and recent trends in mortality and morbidity from 2006 to 2016 were recently published. According to these estimates, chronic kidney disease was the 8th cause of death in Spain in 2016. Among the top ten causes of death, chronic kidney disease was the fastest growing from 2006 to 2016, after Alzheimer disease. At the current pace of growth, chronic kidney disease is set to become the second cause of death in Spain, after Alzheimer disease, by 2100. Additionally, among major causes of death, chronic kidney disease also ranked second only to Alzheimer as the fastest growing cause of Years Lived with Disability (YLDs) and Disability Adjusted Life Years (DALYs). Public resources devoted to prevention, care and research on kidney disease should be in line with both its current and future burden.
El estudio Global Burden of Disease (GBD) mide la salud de las poblaciones en todo el mundo y en cada país de forma annual, y tiene como objetivo ayudar a orientar las políticas públicas sobre cuestiones de salud. Recientemente se publicaron las estimaciones GBD 2016 para España y las tendencias recientes en mortalidad y morbilidad de 2006 a 2016. Según estas estimaciones, la enfermedad renal crónica fue la octava causa de muerte en España en 2016. Entre las 10 principales causas de muerte, la enfermedad renal crónica fue la que más creció entre 2006 y 2016, después de la enfermedad de Alzheimer. Al ritmo actual de crecimiento, la enfermedad renal crónica se convertirá en la segunda causa de muerte en España, después del Alzheimer, hacia el 2100. Además, entre las principales causas de muerte, la enfermedad renal crónica también ocupa el segundo lugar después del Alzheimer como la que más creció en años vividos con discapacidad (AVD) y en años de vida ajustados por discapacidad (AVAD). Los recursos públicos dedicados a la prevención, atención e investigación de la enfermedad renal deberían estar en línea con su carga actual y futura.
The term kidney disease rapidly evokes the concepts of dialysis and transplantation, that is, renal replacement therapy for end-stage kidney disease. Indeed, the 57,429 persons (i.e. 0.1% of the population) living on dialysis or carrying a kidney graft in Spain in 2016 are estimated to consume 2–5% of the healthcare budget.1,2 Spain is a world leader in kidney transplantation and the Organizacion Nacional de Transplantes (ONT) continuous efforts ensure that this leadership position is maintained within the evolving public policy and healthcare frame.3,4 However, the point should not be missed that renal replacement therapy signals the failure of the healthcare system to prevent progression of kidney disease. In this regard, emphasis has moved in recent years to earlier diagnosis of kidney disease in order to treat early, thus preventing kidney disease progression and its potentially lethal complications.
One paradigm shift has been coining the term chronic kidney disease (CKD). According to the 2012 KDIGO (Kidney Disease: Improving Global Outcomes) definition, CKD is diagnosed when abnormalities of kidney structure or function are present for >3 months, with implications for health.5 Thus, the diagnosis of CKD is made in the presence for over 3 months of one marker of kidney damage (albuminuria >30mg/24h or >30mg/g urinary creatinine; or urine sediment abnormalities; or electrolyte and other abnormalities due to tubular disorders; or abnormalities detected by histology; or structural abnormalities detected by imaging; or history of kidney transplantation) or a decreased glomerular filtration rate (GFR; GFR <60ml/min/1.73m2, GFR categories G3–G5). In this regard, the CKD concept expands the prior concept of chronic kidney insufficiency that refers to kidney damage that has resulted in an (unspecified) decrease in GFR. CKD without renal insufficiency can now be diagnosed solely based on urinary albumin values. The immediate clinical implication is that in the absence of albuminuria assessment, CKD cannot be ruled out. This clearly expands the pool of undiagnosed CKD, since in primary care, albuminuria assessment is restricted to a few clinical situations (e.g. diabetes) and even for those situations, uptake by physicians is not universal. The KDIGO CKD concept also provides specific thresholds for eGFR and albuminuria that allow the diagnosis and categorization of CKD. And now comes the most interesting part of the CKD concept: these thresholds are based on epidemiological studies involving millions of individuals that indicate that the thresholds mark an increased risk not only of CKD progression to advanced stages, but also of all-cause and cardiovascular death, as well as of acute kidney injury.
Thus, the 57,429 Spanish persons on renal replacement therapy are only the tip of the iceberg of the healthcare consequences of kidney diseases. Over 4 million Spaniards (just over 10% of the adult population based on a recent SENEFRO study) have CKD and are at risk of premature death because of it.6 However, for many or even most of them, neither the patient, nor the physician is aware of the CKD diagnosis. It is thus estimated that the main impact of CKD is not what we see (persons on renal replacement therapy) but what we do not see (premature deaths, even before reaching the need for renal replacement therapy). In this regard, CKD is not usually listed as a cause of death in CKD patients who die prematurely because of the negative impact of CKD on different organs and systems. The Global Burden of Disease study is addressing such inconsistencies in the attributable cause of death on a worldwide basis and for over 200 causes of death.
What is the GBD study?The Global Burden of Disease (GBD) initiative of the Institute for Health Metrics and Evaluation (IHME) at the University of Washington measures the health of populations worldwide on an annual basis.7 GBD produces age-, sex-, and country-specific health estimates using highly standardized, validated approaches applied to all available data sources and adjusted for major sources of bias, so as worldwide results are comparable. The GBD 2016 report was published in September 2017.8–12 The recent publication of the country-specific GBD 2016 report provides interesting insights into the current and future burden of CKD in Spain.13
How does the GBD study attribute the cause of death?The GBD assess cause of death worldwide using a uniform methodology that has been extensively detailed in GBD publications.11,14 Specifically, it relies on robust statistical methods including the Cause of Death Ensemble model (CODEm) to generate estimates for each location, year, age, and sex. For GBD, each death is attributed to a single underlying cause – the cause that initiated the series of events leading to death – in accordance with International Classification of Diseases (ICD) principles.11 The GBD cause of death list is organized as a hierarchy, with each level composed of causes of death that are mutually exclusive and collectively exhaustive. For GBD 2016, separate estimates were developed for a total of 264 unique causes and cause aggregates. Multiple sources of data are, for Spain the main source is the Mortality Information System INEbase of the Spanish National Institute of Statistics (INE). Cause of death data are then standardized and processed in a uniform manner. This includes identifying and redistributing deaths assigned to ICD codes that cannot be underlying causes of death; are intermediate causes of death rather than the underlying cause (e.g., sepsis and heart failure); or lack specificity in coding. These so-called garbage codes are redistributed using the GBD method: deaths coded in this manner were reassigned to likely causes of death using different approaches.14
What did the GBD 2016 report for Spain say about CKD?According to GBD 2016 estimates, CKD was the 8th cause of death in Spain in 2016 (Table 1A).13 Among the top ten causes of death, CKD was the fastest growing from 2006 to 2016, after Alzheimer disease (Fig. 1A). Additionally, among the top ten causes of death, it also ranked second only to Alzheimer as the fastest growing cause of Years Lived with Disability (YLDs) (Fig. 1B) and Disability Adjusted Life Years (DALYs) (Fig. 1C). DALYs are the sum of years of potential life lost due to premature mortality and the years of productive life lost due to disability. At the current pace, CKD is set to become the second most frequent cause of death in Spain by 2100, after Alzheimer disease (Fig. 2).
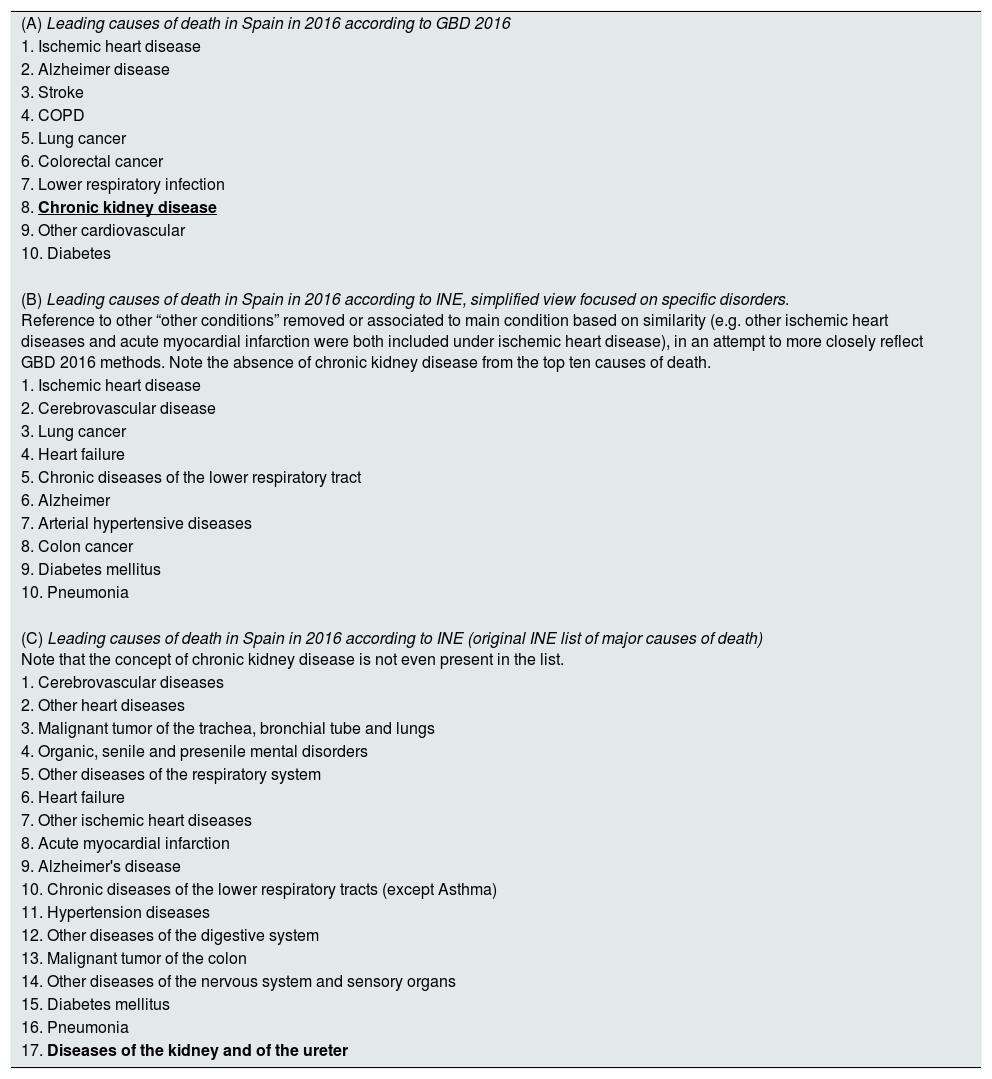
Leading causes of death in Spain in 2016 according to GBD and according to INE. The only major difference is in bold and underlined. INE (Instituto Nacional de Estadística) data were recorded from Basic cause of death statistics.17
| (A) Leading causes of death in Spain in 2016 according to GBD 2016 |
| 1. Ischemic heart disease |
| 2. Alzheimer disease |
| 3. Stroke |
| 4. COPD |
| 5. Lung cancer |
| 6. Colorectal cancer |
| 7. Lower respiratory infection |
| 8. Chronic kidney disease |
| 9. Other cardiovascular |
| 10. Diabetes |
| (B) Leading causes of death in Spain in 2016 according to INE, simplified view focused on specific disorders. Reference to other “other conditions” removed or associated to main condition based on similarity (e.g. other ischemic heart diseases and acute myocardial infarction were both included under ischemic heart disease), in an attempt to more closely reflect GBD 2016 methods. Note the absence of chronic kidney disease from the top ten causes of death. |
| 1. Ischemic heart disease |
| 2. Cerebrovascular disease |
| 3. Lung cancer |
| 4. Heart failure |
| 5. Chronic diseases of the lower respiratory tract |
| 6. Alzheimer |
| 7. Arterial hypertensive diseases |
| 8. Colon cancer |
| 9. Diabetes mellitus |
| 10. Pneumonia |
| (C) Leading causes of death in Spain in 2016 according to INE (original INE list of major causes of death) Note that the concept of chronic kidney disease is not even present in the list. |
| 1. Cerebrovascular diseases |
| 2. Other heart diseases |
| 3. Malignant tumor of the trachea, bronchial tube and lungs |
| 4. Organic, senile and presenile mental disorders |
| 5. Other diseases of the respiratory system |
| 6. Heart failure |
| 7. Other ischemic heart diseases |
| 8. Acute myocardial infarction |
| 9. Alzheimer's disease |
| 10. Chronic diseases of the lower respiratory tracts (except Asthma) |
| 11. Hypertension diseases |
| 12. Other diseases of the digestive system |
| 13. Malignant tumor of the colon |
| 14. Other diseases of the nervous system and sensory organs |
| 15. Diabetes mellitus |
| 16. Pneumonia |
| 17. Diseases of the kidney and of the ureter |
 % change in number of deaths 2006–2016. (B) % change in number of YLDs 2006–2016. Data for top ten causes of death in 2016 which are also among the top 30 causes of YLDs are shown. (C) % change in number of DALYs 2006–2016. COPD: Chronic Obstructive Pulmonary Disease; YLDs: Years Lived with Disability; DALYs: Disability Adjusted Life Years.")
Trends in top ten causes of death in Spain, 2006–2016. The top ten causes of death in 2016 in Spain in terms of number of deaths and their impact on YLDs and DALYs are shown. (A) % change in number of deaths 2006–2016. (B) % change in number of YLDs 2006–2016. Data for top ten causes of death in 2016 which are also among the top 30 causes of YLDs are shown. (C) % change in number of DALYs 2006–2016. COPD: Chronic Obstructive Pulmonary Disease; YLDs: Years Lived with Disability; DALYs: Disability Adjusted Life Years.

Predicted growth of the top eight causes of death from 2016 to 2100 in Spain, based on growth from 2006 to 2016 according to the GBD 2016 study. Alzheimer is predicted to become the most frequent cause of death by 2026 and is not represented in the graph due to its magnitude, which would preclude appreciating details for the other causes of death. The 2006–2016 change in number of deaths was extrapolated to predict annual number of deaths up to 2100. COPD: Chronic Obstructive Pulmonary Disease; YLDs: Years Lived with Disability; DALYs: Disability Adjusted Life Years.
The main source of health information in Spain is the INE, which is used to guide public policy.15 We grouped INE causes of death into a simplified view, aiming at using the same broad concepts as in GBD 2016, and identified ten top causes of death in 2016 according to INE (Table 1B). All categories of cause of death present in the top ten GBD 2016 list can be recognized in the INE ranking, with the exception of CKD. For this simplified view of INE data, we did not take into account items labeled “other”, because of their non-specific nature and for example, we grouped “acute myocardial infarction” together with “other ischemic heart diseases” in the same category of “ischemic heart disease”. Overall, the main difference with the GBD 2016 ranking is the presence of hypertension and the absence of CKD within the top ten causes of death in the simplified INE ranking. The term closest to the CKD concept, at position eleven (and, thus, not shown in Table 1B) if terms including “other” are excluded, is a wider category of “diseases of the kidney and of the ureter”. The fact that one of the top causes of death, according to the GBD 2016 methodology, is hidden from the view of policy makers may be considered a major flaw of the INE information system. This indeed may be one of the reasons for the growing impact of CKD on mortality, since funding for research and early intervention lags well behind other major causes of death.
Why GBD 2016 and INE data do not match?Spain GBD 2016 manuscript emphasized discrepancies between causes of death for Spain GBD 2016 and data from the INE that may impact public health policy planning.13 The discrepancies between INE and GBD may depend on the different definitions used. INE statistics follow the ICD-10 cause of death list. In this regard, several GBD 2016 and INE definitions differ. As examples, IHD is represented by two different categories in INE, “Acute myocardial infarction” and “Other ischemic heart diseases”. Hypertension is considered a garbage code in GBD and is redistributed to other causes of death. Several items labeled “other”, representing several different conditions, made it into the top ten ranking in INE. Overall, all conditions except one in the top ten causes of death according to GBD 2016 can be recognized in a simplified INE list (Table 1B), the sole exception being CKD. However, the original ICD-10-based INE rankings differ more from GBD 2016 data (Table 1C). This may reflect the absence of CKD from the ICD-10 cause-of-death lists as per guidance from the US Centers For Disease Control And Prevention (CDC),16 where the closest term, included within “diseases of the kidney and of the ureter”, is kidney failure. Kidney failure, according to the current consensus international KDIGO 2012 definition, is applied to those on or needing renal replacement therapy, and not to the wider CKD population. Additionally, GBD redistributes causes of death, so the called garbage codes, as explained above, based on a complex algorithm that takes into account an updated medical literature.11,14
Is Spain different from other countries in terms of the impact of CKD in mortality?Not really. According to GBD 2016, CKD was the 10th most frequent cause of death worldwide when assessed by the age-standardized death rate per 100,000, and together with Alzheimer and diabetes, it was among the three fastest growing causes of number of deaths or of age-standardized death rates, and the second fastest growing after Alzheimer in terms of YLL.11 Indeed, the CKD age-standardized death rate increased by 28.8% and the YLLs by 21% from 2006 to 2016 on a worldwide basis.
A dynamic versus a static viewIn conclusion, the recently published GBD 2016 Spain study should be a call to action for the medical community, healthcare authorities and the population at large. CKD lags well behind other major causes of death in terms of resources devoted to prevention, early therapy and research. Public resources devoted to prevention, care and research on kidney disease should be in line with both its current and future burden. Without a significant increase in funding for such activity that dramatically changes the 2006–2016 trend, CKD is set to become the second cause of death in Spain for future generations. GBD 2016 data, by providing a time series over the years, evaluated with the same methodology, standardized and consistent with the methods applied to other countries, provides a dynamic view of the evolving health landscape in Spain that allows planning for the future based on worrisome secular trends like the unrelenting rise of CKD as a major cause of death.
Conflict of interestAll authors, except MDSN, are members of the Council of the Spanish Society of Nephrology.
Research by the authors has been supported by FIS PI16/02057, PI18/01366, ISCIII-RETIC REDinREN RD016/0009 FEDER funds, Sociedad Española de Nefrología, Fundacion Renal Iñigo Álvarez de Toledo (FRIAT), ISCIII Miguel Servet (MDSN), Comunidad de Madrid Biomedicina B2017/BMD-3686 CIFRA2-CM.



