
Kidney transplantation (KT) should be postponed in those people with active bacterial, fungal, viral and parasitic processes, since these must be treated and resolved previously. The objective of this study is to present the screening circuit implemented by the Nephrology clinic and describe the prevalence of tropical and imported infections in KT candidates born or coming from endemic areas.
Materials and methodsDescriptive cross-sectional study, carried out in 2021. Sociodemographic and clinical variables, serological data of general infections and specific tests of tropical infectious diseases were collected. A descriptive analysis of the data was carried out.
Results67 TR candidates from Latin America (32.8%), North Africa (22.4%), Sub-Saharan Africa (14.9%) and Asia (29.9%) were included. 68.7% were men and the mean age was 48.9 ± 13.5 years. After the general and specific studies, 42 (62.7%) patients were referred to the Infectious Diseases Service to complete this study or indicate treatment. 35.8% of the patients had eosinophilia, and in one case parasites were detected in feces at the time of the study. Serology for strongyloidiasis was positive in 18 (26.9%) cases, while positive serology for other tropical infections was hardly detected. 34.3% of patients had latent tuberculosis infection.
ConclusionsThe prevalence of tropical and imported infections in migrant candidates for RT was low, except for strongyloidiasis and latent tuberculosis infection. Its detection and treatment are essential to avoid serious complications in post-TR. To this end, the implementation of an interdisciplinary screening program from the KT access consultation is feasible, necessary and useful.
El trasplante renal (TR) debe posponerse en aquellas personas con procesos bacterianos, fúngicos, virales y parasitarios activos, ya que éstos deben ser tratados y resueltos previamente. El objetivo de este estudio es presentar el circuito de cribado puesto en marcha desde la consulta de Nefrología y describir la prevalencia de infecciones tropicales e importadas en candidatos a TR nacidos o procedentes de áreas endémicas.
Materiales y métodosEstudio descriptivo de corte transversal, llevado a cabo en el año 2021. Se recogieron variables sociodemográficas, clínicas, datos serológicos de infecciones generales y pruebas específicas de enfermedades infecciosas tropicales. Se realizó un análisis descriptivo de los datos.
ResultadosSe incluyeron 67 candidatos a TR procedentes de América Latina (32,8%), África del Norte (22,4%), África Subsahariana (14,9%) y Asia (29,9%). El 68,7% eran hombres y la edad media fue de 48,9 ± 13,5 años. Tras los estudios general y especifico, se derivaron 42 (62,7%) pacientes al Servicio de Enfermedades Infecciosas para completar este estudio o indicar tratamiento. El 35,8% de los pacientes presentaban eosinofilia, detectando en un caso parásitos en heces en el momento del estudio. La serología para estrongiloidiasis resultó positiva en 18 (26,9%) casos, mientras que apenas se detectaron serologías positivas para otras infecciones tropicales. Un 34,3% de pacientes presentaba infección tuberculosa latente.
ConclusionesLa prevalencia de infecciones tropicales e importadas en personas migrantes candidatas a TR fue baja, exceptuando la estrongiloidiasis y la infección tuberculosa latente. Su detección y tratamiento son imprescindibles para evitar complicaciones graves en el posTR. Para ello, la puesta en marcha de un programa de cribado interdisciplinar desde la consulta de acceso al TR es factible, necesaria y útil.
As of January 1 st 2022, there were 5,417,883 foreigners resident in Spain; the figure has tripled in the last 20 years. Morocco is the leading country of origin and Latin America is the leading region of origin, with more than one million of immigrants.1,2
The risk of kidney disease is higher among some minority populations due to a higher prevalence of cardiovascular risk factors and more limited access to health resources.3 According to data from the Registre de Malalts Renals de Catalunya (RMRC), 11.7% of patients who started renal replacement therapy in 2021 were born outside Spain. During the first 9 months of 2022, 19% of the people on the waiting list for kidney transplants (KT) in Catalonia came from other countries. Morocco was, in both cases, the most frequent country of origin the RMRC reports. Adequate care for this population, including the endemic infectious pathology of their countries of origin, is essential for the correct assessment of the KT candidate and post-transplant outcomes.
Within the framework of the Sustainable Development Goals, the World Health Organisation (WHO) has developed a structured plan to address neglected tropical diseases (NTDs).4 These are 20 diseases prevalent in tropical areas that affect more than one billion people in impoverished socio-economic circumstances.4 The causative agents are different pathogens including viruses, bacteria, parasites, fungi and toxins and have devastating social, economic, sanitary and health consequences for the population.5,6 The processes of climate change, globalization and migration have been linked to an increase in the spread of these diseases in previously non-endemic territories, such as Spain.7–9
The international KDIGO guidelines10 (Kidney Disease: Improving Global Outcomes on KT candidate evaluation and management recommends postponing the procedure in all those with active bacterial, fungal, viral and parasitic processes, as these should be treated and resolved prior to KT. In addition, people at risk of having been in contact with NTD, due to being born in or living in an endemic area, should be screened for potentially treatable chronic infections.10
NTDs in the renal transplant population have been reported to be more prevalent in areas including Brazil, Argentina, Mexico, India, China and thoughout Africa, due to their geographical location, the endemic presence of NTDs and particularities of health, surveillance and disease notification systems.11 However, current migratory flows and globalization make it necessary to screen for NTDs in foreign-born KT candidates.7,12 The importance of this screening is directly related to the reduction of infectious complications and mortality after TR.11–13 However, health training in international health is limited,14 which may lead to under-diagnosis of these diseases in non-endemic settings.15,16 Although there are specialists in tropical diseases in many health centers, not all of them have a specific service that can adapt screening of foreign-born patients according to their country of origin.
The main objective of this study is to present the screening method implemented at the KT center and used in this context, as well as to describe the courses of the most prevalent tropical and imported infections in migrant KT candidates in our setting.
Material and methodsStudy designThis is a descriptive cross-sectional study. The research presented complies with the guidelines for reporting observational studies of the STROBE (Strengthening the Reporting of Observational studies in Epidemiology) statement.17
Scope of the study and implementation of a screening program for NTDsThe study was conducted in a tertiary level university hospital. In this center, more than 100 KT procedures are performed annually, which means that more than 500 people in a situation of access to KT (active on the list, under study, temporarily excluded) are assessed every year.18
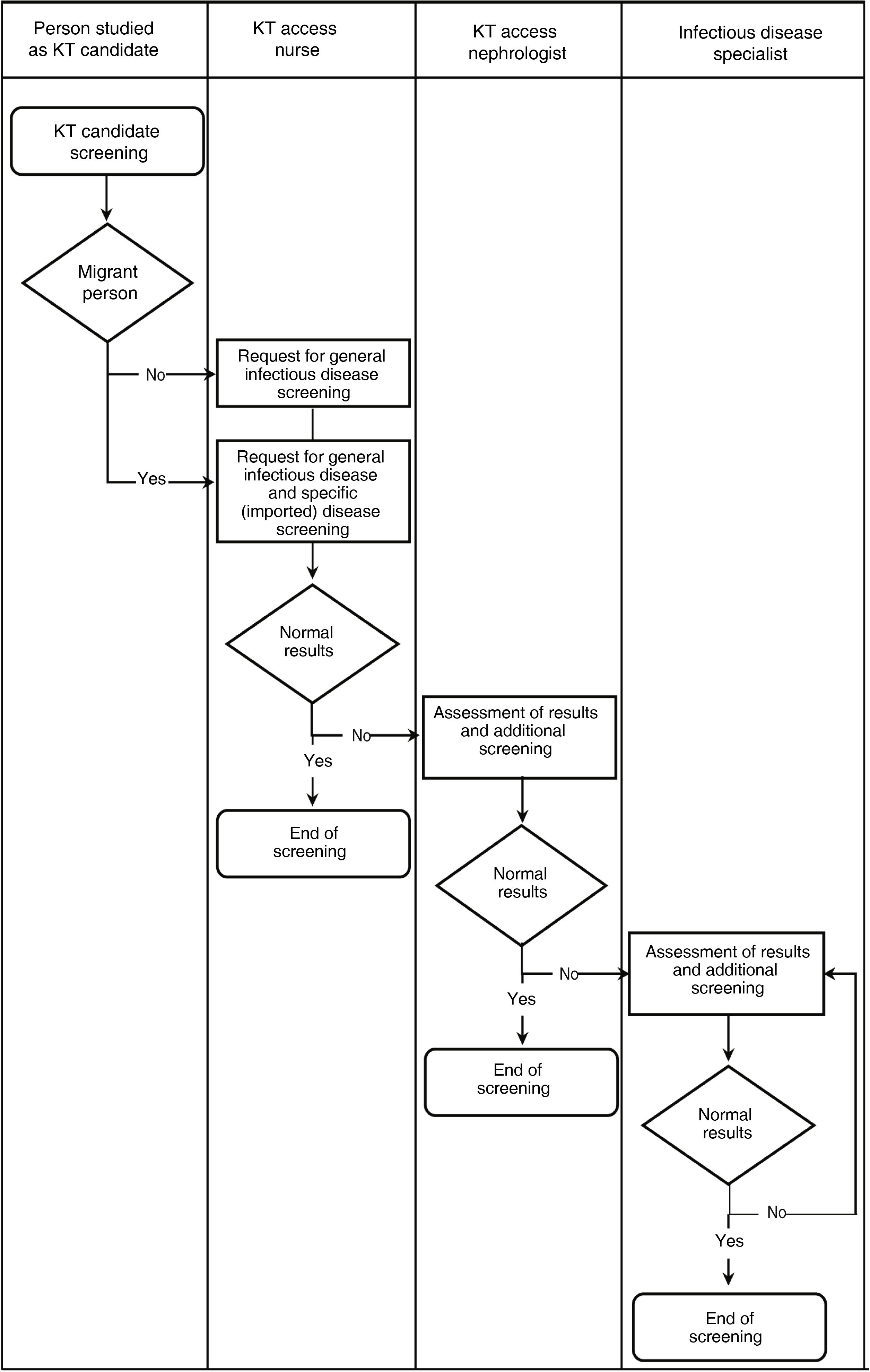
The medical and surgical assessment of the candidate is the responsibility of the referring nephrologist and urologist. The management and optimisation of the process is the responsibility of the KT access nurse. These three professionals assess the suitability of the KT candidate, considering all areas of the candidate's life. In addition, other members of the interdisciplinary team intervene in this assessment process, depending on the needs of the KT candidate, including psychologists, cardiologists, anesthesiologists, pulmonologists, nutritionists, infectious disease specialists and social workers, among others. Their actions and referrals are included in the service's protocols, following the recommendations established in the international reference clinical practice guidelines.10
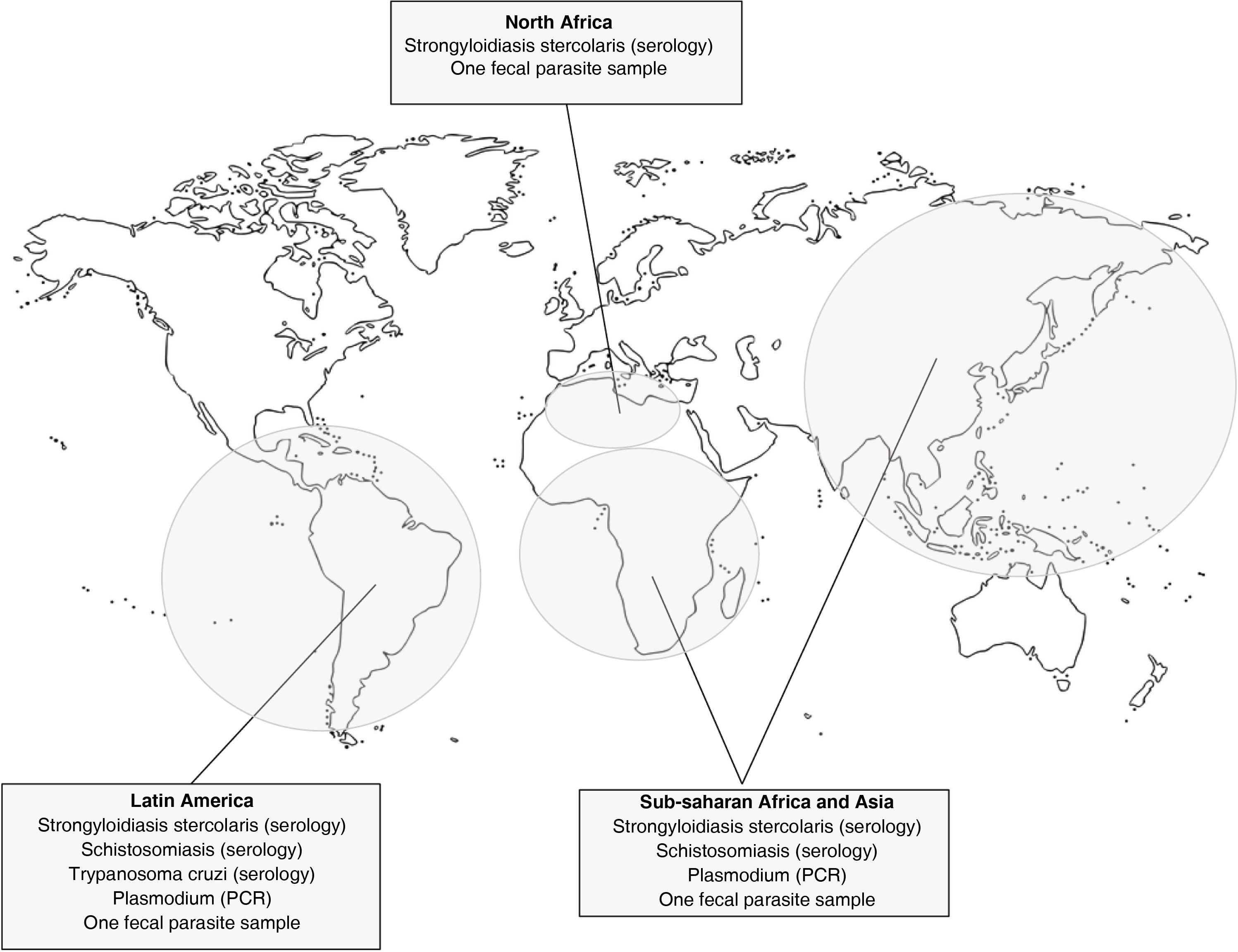
In September 2019, in collaboration with the infectious diseases service, the hospital updated its protocol on screening for tropical infections in KT candidates. The new protocol specifies the complementary examinations that should be performed depending on the geographical origin of the patient and based on the reference literature.19–21 The protocol only considers the most prevalent NTDs in our setting (Fig. 1). The nurse is responsible for obtaining an initial medical history and requesting the relevant tests, and the nephrologist is responsible for assessing the results and refering the candidate to the infectious disease doctor, if required (Fig. 2). This protocol applies to migrants entering the KT program for the first time. In addition, reassessment of the candidate should be considered if there is a long waiting list or candidates had travelled to endemic areas.

Proposal for a screening protocol for imported diseases in migrant kidney transplant candidates according to origin.
*After the initial protocol, Plasmodium sp. screening by serology and peripheral blood smear has been replaced by PCR testing, with better sensitivity for detection.
**In addition, after the initial study, tests for HTLV I-II, Histoplasma capsulatum and Entamoeba histolytica have been removed from the screening.
**For detection of parasites in feces, analysis of the fresh sample is recommended.
Abbreviations: HTLV I-II, human T-cell lymphotropic viruses type I and II.

All people born in Latin America, North Africa, Sub-Saharan Africa or Asia who were on the waiting list for KT or who accessed KT during 2021 were included in the study.
Variables and data collectionThe following variables were recorded using the electronic medical records of the center:
- a)
Socio-demographic variables: age; sex; body mass index (BMI); area of origin; time since arrival in Spain; time of evaluation for inclusion on the waiting list; language use; social support and socio-economic status;
- b)
Clinical variables: hypertension (HT); diabetes mellitus (DM); heart failure; ischemic heart disease; peripheral vascular disease; cerebral vascular disease; chronic obstructive pulmonary disease; etiology of renal disease; renal replacement therapy (RRT) modality; previous RRT and symptoms of imported infectious diseases;
- c)
Infectious screening variables:
c.1) Serologies for general infectious disease: hepatitis A virus; hepatitis B surface antigen; antibody to hepatitis B virus surface antigen; isolated core antibody to hepatitis B virus; antibody to hepatitis C virus; human immunodeficiency virus; cytomegalovirus; mumps virus; rubella virus; varicella virus; Epstein-Barr virus; measles virus; interferon-gamma release assay (IGRA) for tuberculosis;
(c.2) Specific tests for tropical infectious diseases (Fig. 1): Antigen and peripheral blood smear (PBF) screening for blood parasites; parasite studies in feces collected by concentration system; serology for Strongyloides stercoralis, human T-cell lymphotropic viruses type I and II; Entamoeba histolytica; Plasmodium; Histoplasma capsulatum; Trypanosoma cruzi and Schistosoma sp;
c.3) Presence of eosinophilia in the hemogram.
AnalysisA descriptive analysis was made of the variables studied, showing absolute and relative frequencies for qualitative variables, mean and standard deviation for quantitative variables if they followed a normal distribution, and median and interquartile range in the case of non-normal distribution. The results were analyzed with IBM SPSS® statistics version 26 (IBM Corporation).
Ethical considerationsThis study is based on the basic principles guiding care and research in the field of health and social care as set out in the Declaration of Helsinki.22 In accordance with Spain's Organic Law 3/2018, of 5 December, on the protection of personal data and guarantee of digital rights23 and European Regulation 2016/679 on data protection,24 anonymity and confidentiality have been guaranteed by not recording personally identifiable data. The Research Ethics Committee of Parc de Salut Mar approved this study 2020/9418/I.
ResultsWe collected data from 67 KT candidates from Latin America (32.8%), North Africa (22.4%), Sub-Saharan Africa (14.9%) and Asia (29.9%). This sample corresponded to 38.5% of the total number of people on the waiting list for KT at the center analyzed during 2021.
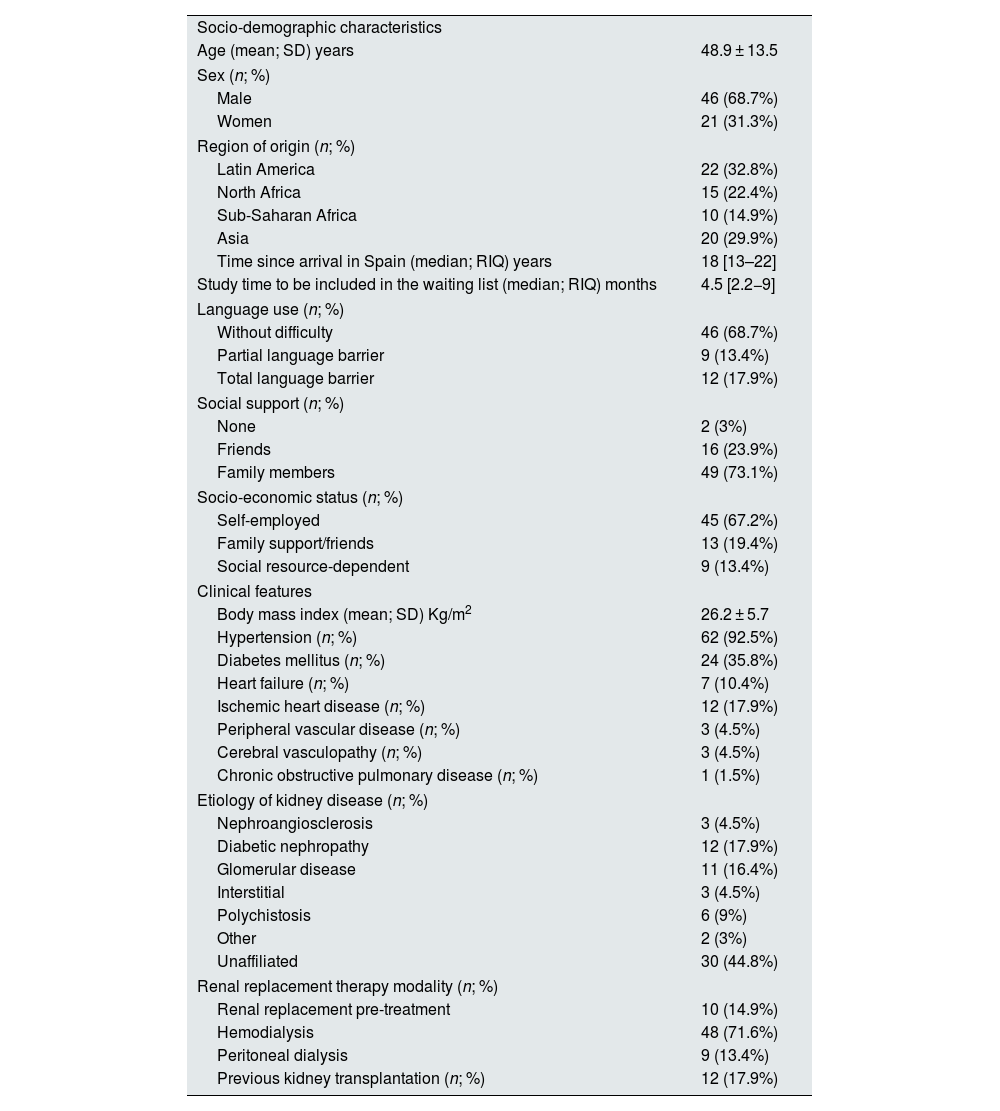
The sociodemographic and clinical variables are described in Table 1. The mean age was 48.9 ± 13.5 years and 68.7% were male. Most of the patients included had no difficulty in the use of the Spanish language (68.7%), had social support from friends or family (97%) and were socioeconomically independent (67.2%). However, almost a third of the patients had language or socio-economic difficulties and were referred to the center's social worker or the assigned primary care center to assess their individual needs.
Socio-demographic and clinical characteristics of the analyzed kidney transplant candidates (n = 67).
| Socio-demographic characteristics | |
| Age (mean; SD) years | 48.9 ± 13.5 |
| Sex (n; %) | |
| Male | 46 (68.7%) |
| Women | 21 (31.3%) |
| Region of origin (n; %) | |
| Latin America | 22 (32.8%) |
| North Africa | 15 (22.4%) |
| Sub-Saharan Africa | 10 (14.9%) |
| Asia | 20 (29.9%) |
| Time since arrival in Spain (median; RIQ) years | 18 [13–22] |
| Study time to be included in the waiting list (median; RIQ) months | 4.5 [2.2−9] |
| Language use (n; %) | |
| Without difficulty | 46 (68.7%) |
| Partial language barrier | 9 (13.4%) |
| Total language barrier | 12 (17.9%) |
| Social support (n; %) | |
| None | 2 (3%) |
| Friends | 16 (23.9%) |
| Family members | 49 (73.1%) |
| Socio-economic status (n; %) | |
| Self-employed | 45 (67.2%) |
| Family support/friends | 13 (19.4%) |
| Social resource-dependent | 9 (13.4%) |
| Clinical features | |
| Body mass index (mean; SD) Kg/m2 | 26.2 ± 5.7 |
| Hypertension (n; %) | 62 (92.5%) |
| Diabetes mellitus (n; %) | 24 (35.8%) |
| Heart failure (n; %) | 7 (10.4%) |
| Ischemic heart disease (n; %) | 12 (17.9%) |
| Peripheral vascular disease (n; %) | 3 (4.5%) |
| Cerebral vasculopathy (n; %) | 3 (4.5%) |
| Chronic obstructive pulmonary disease (n; %) | 1 (1.5%) |
| Etiology of kidney disease (n; %) | |
| Nephroangiosclerosis | 3 (4.5%) |
| Diabetic nephropathy | 12 (17.9%) |
| Glomerular disease | 11 (16.4%) |
| Interstitial | 3 (4.5%) |
| Polychistosis | 6 (9%) |
| Other | 2 (3%) |
| Unaffiliated | 30 (44.8%) |
| Renal replacement therapy modality (n; %) | |
| Renal replacement pre-treatment | 10 (14.9%) |
| Hemodialysis | 48 (71.6%) |
| Peritoneal dialysis | 9 (13.4%) |
| Previous kidney transplantation (n; %) | 12 (17.9%) |
SD: standard deviation; IQR: interquartile range.
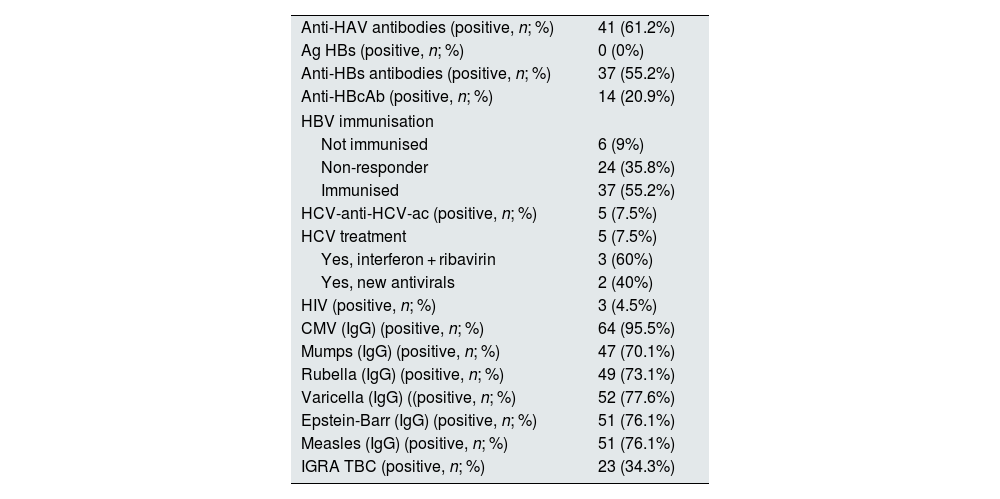
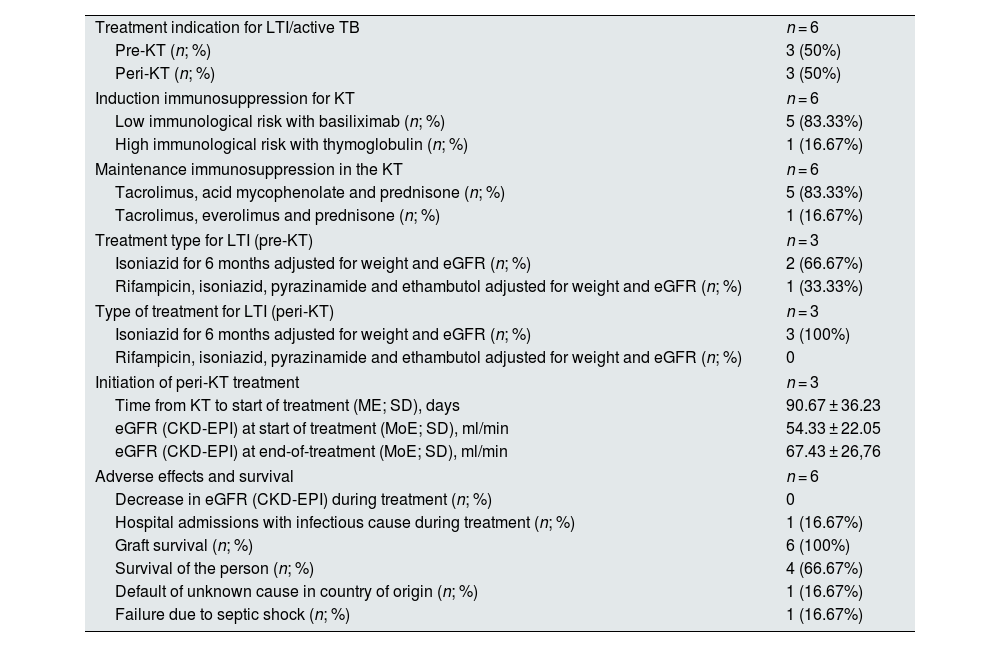
The general screening of this population for infectious diseases is detailed in Table 2. Most patients included were correctly immunised, either naturally or by vaccination, against the common viruses. Despite this, 44.8% of patients were found to be non-immunised or non-responders to the hepatitis B virus vaccine. 34.3% (n = 23) of the patients were diagnosed with latent tuberculosis infection (LTBI) by a positive IGRA test (Quantiferon® TB Gold plus) and were referred to the infectious diseases service. Depending on the risk of reactivation and time of diagnosis, specific treatment with isoniazid was indicated for 6 months during waiting list time (pre-KT, n = 8) or during peri-KT (n = 15, patients who were on pre-dialysis at the time of assessment). During the study period, 6 of these patients received a renal graft after a mean of 2.3 years on the waiting list (3 had been treated pre-KT― and one of them additionally received a boost with isoniazid for 3 months post-KT― and three were treated peri-KT). Patients with an indication for peri-KT treatment who did not undergo transplantation during the study period remained untreated until the start of dialysis (Table 3).
General screening for infectious diseases in renal transplant candidates (n = 67).
| Anti-HAV antibodies (positive, n; %) | 41 (61.2%) |
| Ag HBs (positive, n; %) | 0 (0%) |
| Anti-HBs antibodies (positive, n; %) | 37 (55.2%) |
| Anti-HBcAb (positive, n; %) | 14 (20.9%) |
| HBV immunisation | |
| Not immunised | 6 (9%) |
| Non-responder | 24 (35.8%) |
| Immunised | 37 (55.2%) |
| HCV-anti-HCV-ac (positive, n; %) | 5 (7.5%) |
| HCV treatment | 5 (7.5%) |
| Yes, interferon + ribavirin | 3 (60%) |
| Yes, new antivirals | 2 (40%) |
| HIV (positive, n; %) | 3 (4.5%) |
| CMV (IgG) (positive, n; %) | 64 (95.5%) |
| Mumps (IgG) (positive, n; %) | 47 (70.1%) |
| Rubella (IgG) (positive, n; %) | 49 (73.1%) |
| Varicella (IgG) ((positive, n; %) | 52 (77.6%) |
| Epstein-Barr (IgG) (positive, n; %) | 51 (76.1%) |
| Measles (IgG) (positive, n; %) | 51 (76.1%) |
| IGRA TBC (positive, n; %) | 23 (34.3%) |
HBcAg: hepatitis B virus core antibody isolate; HBsAg: hepatitis B virus surface antigen antibody; HCV: hepatitis C virus core antibody isolate; HBsAg: hepatitis B surface antigen; CMV: cytomegalovirus; IgG: immunoglobulin G; IGRA: Interferon-Gamma Release Assay; TBC: tuberculosis; KT: renal transplant; IgG: immunoglobulin G; IGRA: Interferon-Gamma Release Assay; TB: tuberculosis; KT: renal transplantation; HAV: hepatitis A virus; HBV: hepatitis B virus; HCV: hepatitis C virus; HIV: human immunodeficiency virus.
Treatment for latent tuberculosis infection in the sample that was transplanted during the study time (n = 6).
| Treatment indication for LTI/active TB | n = 6 |
| Pre-KT (n; %) | 3 (50%) |
| Peri-KT (n; %) | 3 (50%) |
| Induction immunosuppression for KT | n = 6 |
| Low immunological risk with basiliximab (n; %) | 5 (83.33%) |
| High immunological risk with thymoglobulin (n; %) | 1 (16.67%) |
| Maintenance immunosuppression in the KT | n = 6 |
| Tacrolimus, acid mycophenolate and prednisone (n; %) | 5 (83.33%) |
| Tacrolimus, everolimus and prednisone (n; %) | 1 (16.67%) |
| Treatment type for LTI (pre-KT) | n = 3 |
| Isoniazid for 6 months adjusted for weight and eGFR (n; %) | 2 (66.67%) |
| Rifampicin, isoniazid, pyrazinamide and ethambutol adjusted for weight and eGFR (n; %) | 1 (33.33%) |
| Type of treatment for LTI (peri-KT) | n = 3 |
| Isoniazid for 6 months adjusted for weight and eGFR (n; %) | 3 (100%) |
| Rifampicin, isoniazid, pyrazinamide and ethambutol adjusted for weight and eGFR (n; %) | 0 |
| Initiation of peri-KT treatment | n = 3 |
| Time from KT to start of treatment (ME; SD), days | 90.67 ± 36.23 |
| eGFR (CKD-EPI) at start of treatment (MoE; SD), ml/min | 54.33 ± 22.05 |
| eGFR (CKD-EPI) at end-of-treatment (MoE; SD), ml/min | 67.43 ± 26,76 |
| Adverse effects and survival | n = 6 |
| Decrease in eGFR (CKD-EPI) during treatment (n; %) | 0 |
| Hospital admissions with infectious cause during treatment (n; %) | 1 (16.67%) |
| Graft survival (n; %) | 6 (100%) |
| Survival of the person (n; %) | 4 (66.67%) |
| Default of unknown cause in country of origin (n; %) | 1 (16.67%) |
| Failure due to septic shock (n; %) | 1 (16.67%) |
eGFR, estimated glomerular filtration rate; IGRA, Interferon-Gamma Release Assay; LTI, latent tuberculosis infection; ME, mean; SD, standard deviation; KT, renal transplant.
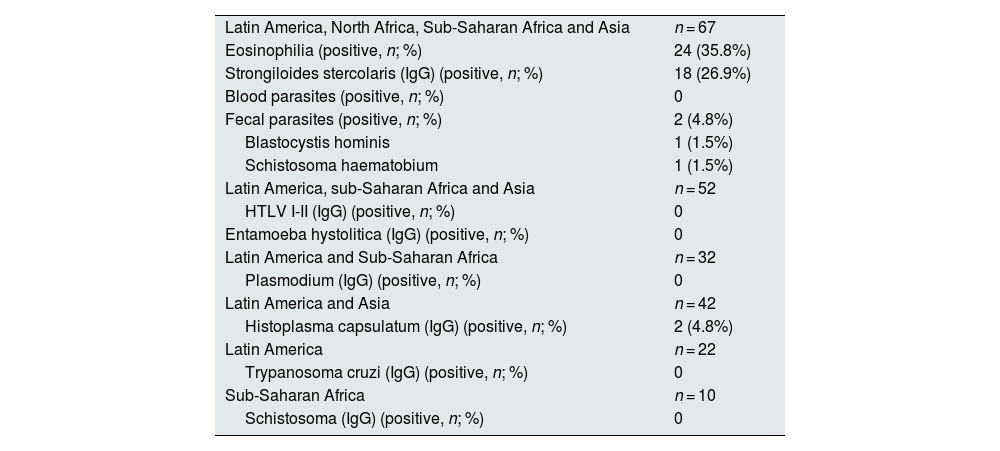
The specific screening for tropical diseases, according to the origin of the individual, is presented in Table 4. 35.8% of the cohort (n = 24) had eosinophilia and required referral to infectious diseases for further study. Of these patients, 2 had a history of previous parasitosis and none of them had symptoms related to parasitic infection at the time of the study. In 4 patients the eosinophilia was due to allergic phenomena not caused by parasite co-infection; in 6 patients the cause of eosinophilia was not found by serological and copro-parasitological study, so triple empirical treatment was administered with ivermectin 200 µg/kg/day/for 2 days, albendazole 400 mg/24 h/for 5 days and praziquantel 40 mg/kg/ in 2 doses, following the recommendations of the Spanish Society of Tropical Medicine and International Health (SEMTSI).22 In 14 patients, eosinophilia was associated with Strongyloides; and in one patient from Senegal, Schistosoma haematobium was detected in feces. In total, 26.9% of the KT candidates had positive serology for strongyloidiasis and received antiparasitic treatment with ivermectin.
Screening for tropical and imported diseases in KT candidates from other geographic areas (n = 67).
| Latin America, North Africa, Sub-Saharan Africa and Asia | n = 67 |
| Eosinophilia (positive, n; %) | 24 (35.8%) |
| Strongiloides stercolaris (IgG) (positive, n; %) | 18 (26.9%) |
| Blood parasites (positive, n; %) | 0 |
| Fecal parasites (positive, n; %) | 2 (4.8%) |
| Blastocystis hominis | 1 (1.5%) |
| Schistosoma haematobium | 1 (1.5%) |
| Latin America, sub-Saharan Africa and Asia | n = 52 |
| HTLV I-II (IgG) (positive, n; %) | 0 |
| Entamoeba hystolitica (IgG) (positive, n; %) | 0 |
| Latin America and Sub-Saharan Africa | n = 32 |
| Plasmodium (IgG) (positive, n; %) | 0 |
| Latin America and Asia | n = 42 |
| Histoplasma capsulatum (IgG) (positive, n; %) | 2 (4.8%) |
| Latin America | n = 22 |
| Trypanosoma cruzi (IgG) (positive, n; %) | 0 |
| Sub-Saharan Africa | n = 10 |
| Schistosoma (IgG) (positive, n; %) | 0 |
HTLV I-II: human T-cell lymphotropic viruses type I and II; IgG: immunoglobulin G.
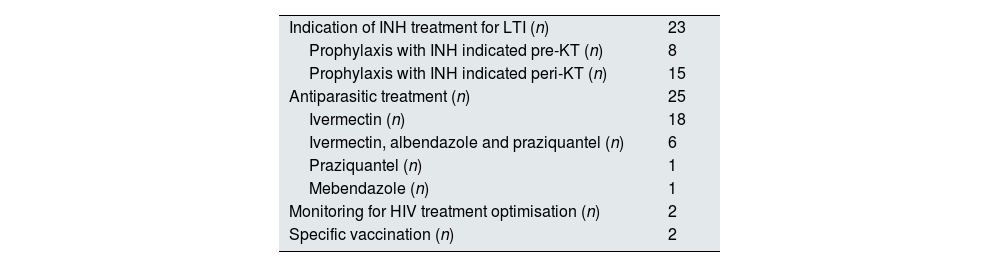
Overall, after the general and specific studies and the clinical assessment by the nephrologist in charge, 62.7% of the KT candidates were referred to the infectious diseases service to extend this study, assess vaccination, indicate pharmacological treatment and/or optimise existing treatment (Table 5). In no case was a re-evaluation of NTD required in the sample included due to the absence of travel to endemic areas.
Specific treatments and actions by the infectious diseases service for referred patients (n = 42).
| Indication of INH treatment for LTI (n) | 23 |
| Prophylaxis with INH indicated pre-KT (n) | 8 |
| Prophylaxis with INH indicated peri-KT (n) | 15 |
| Antiparasitic treatment (n) | 25 |
| Ivermectin (n) | 18 |
| Ivermectin, albendazole and praziquantel (n) | 6 |
| Praziquantel (n) | 1 |
| Mebendazole (n) | 1 |
| Monitoring for HIV treatment optimisation (n) | 2 |
| Specific vaccination (n) | 2 |
IgE: immunoglobulin E; INH: isoniazid; LTI: latent tuberculosis infection.
This study describes the implementation of a screening program for tropical and imported infections in our KT center and the frequency of such infections in a cohort of migrant KT candidates. We found a high prevalence of strongyloidiasis and LTI. The prevalence of all other infections in the study population was very low, however, since the screening was performed using indirect techniques, there was probably a loss of sensitivity in detecting some latent infections.25,26
Given the expected increase in the incidence of tropical and imported infections in non-endemic areas11,16,27,28 and the potential consequences of their under-diagnosis in the transplant candidate population,10–12 specific screening and treatment prior to transplantation is essential. Infections are the leading cause of death in transplant recipients in tropical and subtropical countries and, in so-called "developed settings", they are the second or third leading cause of death in these patients.11,29,30 Furthermore, infectious processes represent 21% of the causes of hospitalization in the population with chronic kidney disease, behind only cardiovascular causes.31 The complications that may arise from the failure to detect and treat these diseases can be fatal for the person having access to KT, the same consequences as a de novo post-TR infection.10–12
Regarding the general infectious screening in foreign-born KT candidates, we found a high percentage with LTI (34.3%). It is also noteworthy that almost half of the patients were no vaccinated against hepatitis B (44.8%), and most of those were non-responders to the vaccine, although we found six patients who had not received vaccination despite its specific indication in the population with advanced CKD. According to the RMRC, of the patients who started renal replacement therapy in Catalonia in 2020, only 60.6% were vaccinated against hepatitis B.
Regarding the specific study of tropical and imported diseases, more than one third of the cohort had eosinophilia at the time of the study, a finding that may be related to an active or latent parasitic form. In one case an active parasitic form was confirmed via stool screening and six patients received empirical treatment with antiparasitic drugs. Eosinophilia in the CKD population may be related to other diagnoses or syndromes32 and therefore its value as a screening for tropical diseases is limited.33 In the cohort studied, most of these eosinophilias corresponded to the finding of a positive Strongyloides serology. It has been reported that only 50% of Strongyloides patients have eosinophilia, although its predictive value in this disease and other helminthiases is high.21
Strongyloides stercoralis is a helminth that affects 10–60% of the population in tropical and subtropical areas.28 In Spain, it is uncertain whether it is already an endemic disease,34 and a prevalence of around 10% has been reported at hospital level in populations from Africa and Latin America.35 In the case of KT candidates who are going to undergo immunosuppression, infection by this parasite can have fatal consequences, as it can become highly replicating and develop the so-called "hyperinfestation syndrome" or spread to other vital organs, causing high mortality via bacteremias caused by gram-negative bacilli, Loeffler's syndrome, secondary bacterial meningitis or severe colitis, among others. This especially affects patients receiving immunosuppressants, including corticosteroids.36 In addition, the parasite's life cycle allows for auto-infection cycles, so infection could have occurred more than 30 years ago.34 Screening and appropriate pre-KT treatment of the population at risk is essential to minimise the negative impact of immunosuppressive treatment.
Conversely, in our cohort, we did not find other parasitic forms such as Plasmodium, Entamoeba or Trypanosoma cruzi. However, Plasmodium is the most prevalent parasitic infection worldwide, affecting more than 228 million people and causing the death of 405,000 people annually in 108 countries around the world.21,37 Cases were probably not detected because malaria was ruled out only with antigen and peripheral blood smear (PBS) which are low-sensitivity tests in patients with subacute/chronic infection, the ideal test for these patients being Plasmodium sp. PCR.26Entamoeba is the second leading cause of death due to protozoan infection worldwide,28 and Chagas disease has a prevalence of 8–10 million people in 21 Latin American countries,38,39 although we also found no cases in the cohort analyzed. We did detect one case of schistosomiasis in a patient from Senegal. The prevalence of this parasite is moderate/high in sub-Saharan Africa, reaching more than 50% of the population in countries such as Sierra Leone, Ghana, Tanzania, Mozambique and Madagascar.28
Although the screening for fungus causing histoplasmosis is not recommended for pre-KT screening due to its low incidence after KT, we identified 2 IgG-positive patients in this study.
It should be kept in mind that the sensitivity of serological techniques in patients with CKD may be compromised by a state of baseline immunosuppression associated with the disease itself. It is therefore essential: (1) to perform early screening in this group of patients (in the advanced CKD phase), before the state of pharmacological immunosuppression further compromises the validity of the available techniques, and (2) to use more sensitive techniques such as PCR or direct stool analysis.26
Patients receiving KT can develop a tropical or imported infection through different pathways: (1) through reactivation of a latent infection acquired prior to KT, (2) through transmission of the infection from the donor carrying the pathogen, or (3) through the development of a de novo infection acquired after KT in an endemic area.27 Before KT, both the recipient and the donor should undergo preventive screening for the described infections. After transplantation, health education for the recipient and prophylaxis to prevent de novo infections will be important.12,27 Some 25–30% of transplant recipients may travel to tropical and subtropical areas without prior knowledge of the healthcare team, and 5–10% may develop a complication derived from an NTD.12,39,40 Correct follow-up, pre- and post-transplant health education on possible risks, and individualization of immunosuppressive treatment are necessary to avoid this type of action due to lack of knowledge.41,42
In this study, an interdisciplinary pre-KT screening program was followed with the main objective of adequately evaluating infectious risks and ensuring suitability for KT. The screening program is initiated at the KT access consultation and, depending on the findings, the candidate is referred or not to the infectious diseases department. Almost two thirds of the patients required this referral and/or consultation. The initiation and coordination of the study by the nephrology department has advantages. In addition, it avoids unnecessary visits for the patient (which in many cases will go to another referral center) and avoids prolonging the screening time for KT. In addition, first-hand knowledge of the patient's risks promotes a state of alertness for early detection of the problem.
Within the framework of the UN Sustainable Development Goals, by 2030 this group of NTDs should be under control and this requires increased recognition of the current situation in order to be able to act accordingly and apply the relevant preventive or curative measures at the appropriate time.4,5 Screening for NTDs in both the general population and in the CKD population awaiting KT is now a real need in all those who may have been in direct contact in endemic areas. Immunosuppressive treatment can cause asymptomatic or unmanifested infections to be exacerbated or reactivated.37–39 Thus, to guarantee the safety of the people treated and the quality of the care provided, it is essential to promote the recognition of these diseases, which are becoming increasingly prevalent in our environment.
The present study is a single-center study with a small sample size that has limitations. The main limitation is that screening for tropical diseases was mainly performed by indirect serological diagnosis and stool concentration (not fresh samples), which in this type of patient could have led to false negatives. Furthermore, the protocol does not cover 100% of the NTDs considered by the WHO, focusing instead on those with the highest prevalence in our setting. Due to the characteristics of the sample and the long time since migration, the prevalence of acute/subacute tropical diseases could not be explored either. However, it is known that chronic tropical diseases can also cause morbidity and mortality in immunocompromised patients.43 Despite these limitations, the reported findings are significant, in line with the reference literature, and set out a clear strategy for action to tailor the proposed interventions to the specific needs of the target population. It will be necessary to increase the prospective sample size and conduct multicenter studies to achieve more relevant evidence.
ConclusionsThe prevalence of strongyloidiasis and LTI in screening for tropical and imported diseases in asymptomatic migrants who were KT candidates was high. Their detection and treatment are essential to avoid serious complications in post-KT. To this end, the implementation of an interdisciplinary screening program, led by the nephrology department, is a feasible healthcare practice, with the potential advantage of streamlining screening and shortening the waiting times involved in inter-specialty consultations.
FundingThe authors declare that they have not received any funding for this work.
AuthorsGPR, ABP and MJPS conceived of and designed the study and conducted data acquisition, analysis and interpretation.
SCN, EP, CAC, DRP, FS, JPH, JP and MC participated in the critical revision of the final manuscript, contributing important intellectual content to the outcome.
All authors have read and approve the final manuscript.
GPR, JVG and MJPS take responsibility for the published document.
Conflict of interestThe authors declare that they have no conflicts of interest.
Judit Boluña and Ariadna Graells for their contribution to the design of the protocol's quality circuit.
Laia Fontdevila-Sans and Yasmin Taouil for arranging the necessary tests for this study.



