
After the rapid spread of the COVID-19 pandemic, different reports have been written with contradictory results about the presence of the SARS-CoV-2 virus in peritoneal fluid, as Vischini et al.1 and Coccolini et al.2 report in favour, while Candellier et al. and other authors state the opposed.3–5 For nephrologists it is important to know about the possible presence of the SARS-CoV-2 virus in the dialysis effluent in patients on peritoneal dialysis. Some pathophysiological mechanisms have been mentioned related to the characteristics of the peritoneal membrane and that of the virion itself. The pores of the peritoneal membrane have a maximum diameter of 20−40 nm, while the SARS-CoV-2 virion diameter measures between 60 and 140 nanometres. In theory the virion could enter the peritoneal cavity via haematogenous diffusion or via the peritoneal dialysis catheter after contact contamination.3
Specifically, in Latin America, including Mexico, ambulatory peritoneal dialysis predominates as renal replacement therapy.6 In our experience, we found four patients, two women and two men from the ambulatory peritoneal dialysis programme, three of whom were in continuous ambulatory peritoneal dialysis and one in automated peritoneal dialysis, with an age ranging from 35 to 64 years and with different comorbidities, including diabetes mellitus, hypertension, rheumatoid arthritis, and obesity (Table 1). All cases were diagnosed with COVID-19 by real-time inverse polymerase chain reaction (RT-PCR) test targeting SARS-CoV-2 from samples obtained from the nasopharynx or by CT findings. Samples for RT-PCR were obtained from the peritoneal effluent with a dwell time in the cavity of six hours and the following findings were obtained: three patients were positive for the presence of SARS-CoV-2 in the nasopharynx and in the dialysis effluent, while the fourth patient was negative for the presence of the virus in both samples, despite having CT scan findings highly compatible with the disease. It should be mentioned that in the three patients with positive SARS-CoV-2 RT-PCR tests in the nasopharynx and dialysis effluent, the samples were performed within the first seven days of the onset of COVID-19-related symptoms, and in the fourth patient, the sample was obtained from the peritoneal effluent after more than seven days of the onset of symptoms. All four patients had transparent and colourless peritoneal dialysis effluents. None of the cases reported localised symptoms in the abdominal region. Three of the four patients died during their hospital stay.
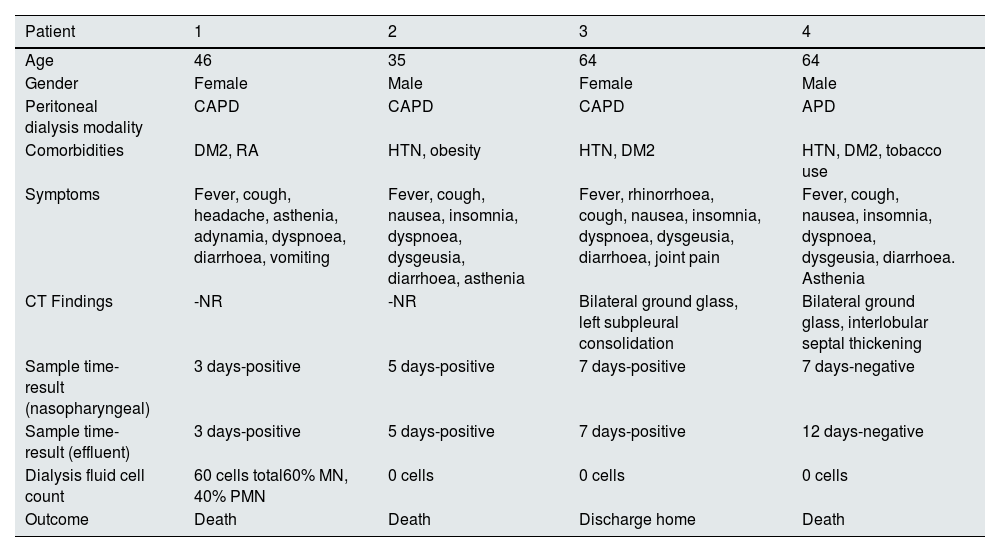
Characteristics and comorbidities of patients in the ambulatory peritoneal dialysis programme.
| Patient | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| Age | 46 | 35 | 64 | 64 |
| Gender | Female | Male | Female | Male |
| Peritoneal dialysis modality | CAPD | CAPD | CAPD | APD |
| Comorbidities | DM2, RA | HTN, obesity | HTN, DM2 | HTN, DM2, tobacco use |
| Symptoms | Fever, cough, headache, asthenia, adynamia, dyspnoea, diarrhoea, vomiting | Fever, cough, nausea, insomnia, dyspnoea, dysgeusia, diarrhoea, asthenia | Fever, rhinorrhoea, cough, nausea, insomnia, dyspnoea, dysgeusia, diarrhoea, joint pain | Fever, cough, nausea, insomnia, dyspnoea, dysgeusia, diarrhoea. Asthenia |
| CT Findings | -NR | -NR | Bilateral ground glass, left subpleural consolidation | Bilateral ground glass, interlobular septal thickening |
| Sample time-result (nasopharyngeal) | 3 days-positive | 5 days-positive | 7 days-positive | 7 days-negative |
| Sample time-result (effluent) | 3 days-positive | 5 days-positive | 7 days-positive | 12 days-negative |
| Dialysis fluid cell count | 60 cells total60% MN, 40% PMN | 0 cells | 0 cells | 0 cells |
| Outcome | Death | Death | Discharge home | Death |
APD, automated peritoneal dialysis; CAPD, continuous ambulatory peritoneal dialysis; DM2, type 2 diabetes mellitus; HTN, arterial hypertension; RA, rheumatoid arthritis.
The presence of SARS-CoV-2 in the peritoneal fluid continues to be a topic of lively debate in the literature on COVID-19. Positive RT-PCR for SARS-CoV-2 should be confirmed or ruled out using subsequent studies with greater statistical power.
Different authors have reported that, to date, the procedure for obtaining peritoneal effluent samples has certainly not yet been standardised, which could explain the discordant and inconsistent results in the bodily secretions and excretions, specifically from peritoneal fluid. Based on our experience, we advocate implementing SARS-CoV-2 RT-PCR detection in peritoneal effluent with a three to seven day margin of time after the onset of clinical symptoms suggestive of COVID-19, and in addition, that the effluent should have a dwell time in the peritoneal cavity of six hours, without centrifuging the sample. We join the observations that suggest culturing for SARS-CoV-2 to confirm the presence of the virus in the abdominal fluid before performing specific procedures when managing peritoneal dialysis effluent.



