The COVID-19 epidemic represents a special risk for kidney patients due to their comorbidities and advanced age, and the need for hemodialysis treatment in group rooms. It also represents a risk for professionals responsible for their attention. This manuscript contains a proposal for action to prevent infection of professionals in the Nephrology Services, one of the most valuable assets at the present time.
La epidemia de COVID-19 representa un riesgo especial para los pacientes renales por sus comorbilidades y edad avanzada, y por la realización del tratamiento de hemodiálisis en salas colectivas, pero también supone un riesgo para los profesionales responsables de su atención. El presente manuscrito recoge una propuesta de actuación para prevenir la infección entre los profesionales en los Servicios de Nefrología.
In addition to the obvious need to protect patients, it is no less important to guarantee the protection of the healthcare professionals who have to treat them. There are a number of reasons why the protection of healthcare professionals has to be one of the main objectives in the SARS-CoV-2 pandemic: 1) They are necessary to guarantee the continuity of care; 2) They have a high risk of contagion due to their front-line exposure to infected patients; and 3) They may act as transmission vehicles in their day-to-day work to patients, other colleagues, and members of their families and the community.
Up to 25 February 2020, China had reported 3387 infected healthcare workers in Hubei alone, at least 18 of whom died as a result of the infection.1 In Spain, according to the most recent official data made public by the Ministry of Health, on 7 May there were 35,548 healthcare professionals infected by COVID-19.2 Spain has one of the highest figures in the world for healthcare workers infected by COVID-19. In a recent study in a hospital in Madrid, 20% of the healthcare staff in the Nephrology department were diagnosed with COVID-19.3
Like other viruses of the same family, SARS-CoV-2 spreads mainly through droplets and direct contact with the secretions of infected people.4 However, it also has several distinguishing features which make it necessary to increase precautions against contagion, including the high rate of infected individuals who remain asymptomatic with an incubation period which can be as long as 24 days5, the hyper-affinity to the receptors of angiotensin-converting enzyme 2 (ACE2), which makes it highly transmissible6,7, and the 20–30% false-negative rate in PCR detection.8
Every hospital, nephrology department and haemodialysis centre has implemented its own action protocol, the majority aimed at preventing transmission to patients.9–11 There has also been special emphasis on preventing transmission from patients to healthcare professionals.12–15 However, less attention has been paid to preventing contagion among healthcare professionals within the hospital setting, particularly when, as already mentioned, the infection can be asymptomatic for a prolonged period, and the available detection tools fail to detect all cases.
In the present manuscript we present a set of strategies designed to prevent contagion among healthcare professionals in a nephrology department through patients and the co-workers themselves.
Type of exposure of healthcare professionals and the consequences thereofHealthcare professionals are at risk due to the activities they perform. This exposure can result from contact with other patients or with co-workers. There are different types of exposure to SARS-CoV-2, and each type can have different consequences13:
- a)
Low-risk exposure without the appropriate protective equipment: isolated episodes of exposure of < 15 min with minimal physical contact; for example, delivering medication or a food tray, taking vital signs, procedures that do not generate aerosols, contact with cases of healthcare professionals in the work environment.
- b)
High-risk exposure without the appropriate protective equipment: contact with a household member or contact with an exposure time of more than 15 min at a distance of less than 2 m, contact with a patient at high risk of exposure to respiratory secretions without protection or procedures that generate aerosols.
In the first case, if they are asymptomatic, the healthcare professional can continue working with a surgical mask throughout their working day, although they should monitor their temperature and be alert to symptoms. Should they develop symptoms, they should self-isolate immediately (separate themselves from other individuals) and notify Occupational Health without delay.
In the second case, the healthcare professional should be sent home with axillary temperature monitoring twice a day, and withdrawn from healthcare activity for seven days. They may return to work on day eight if they are still asymptomatic. They will need to wear a surgical mask throughout their working day until day 14 after the contact (in addition to the usual basic self-protection measures).
The department designated as responsible by the hospital (Occupational Health, Occupational Risk Prevention or Preventive Medicine) will carry out a personalised risk assessment, taking into account the type of exposure and the department in which the member of staff works, and may give instructions adapted to the specific case.
Measures to be taken by healthcare professionals in the hospital and care setting to prevent the spread of COVID-19Healthcare workers are forced to accept the possibility of being exposed to and infected by SARS-CoV-215,16 as they have to work in close proximity to suspected patients or cases and, additionally, have to cope with an exceptional workload. In these conditions, it is particularly important for all workers to know what personal protective equipment should be used for each activity, and to be conversant with the procedure for putting on and removing said equipment.17 Adherence to these measures should be promoted and supervised by teamwork among the medical-nursing-auxiliary staff, reinforcing both actions.3,18
Individual measures in the hospital and care settingLike any healthcare professional in any healthcare facility, Nephrology staff should adhere to the following17,18:
- none-
compulsory wearing of masks in common spaces (stairs, hallways, elevators, lifts, corridors, terraces, toilets and reception areas);
- none-
use the stairs instead of the lift, whenever possible;
- none-
in corridors and stairs, always keep to the right;
- none-
systematically wash hands with soap and water or apply alcohol solutions to hands;
- none-
keep a safe distance (at least 2 m);
- none-
avoid touching their eyes, nose and mouth with unwashed hands;
- none-
cover their nose and mouth with their sleeve or a tissue and then dispose of it if they cough or sneeze;
- none-
avoid sharing personal equipment and devices with other workers;
- none-
avoid face-to-face meetings, preferably using videoconferences or other non-face-to-face systems;
- none-
clean and disinfect workspaces and frequently touched surfaces, such as keyboards, dictation devices or land-line telephones, and personal items, such as stethoscopes or mobile phones. SARS-CoV-2 is capable of living on surfaces for hours or days19,20, but it is easily eliminated with common disinfectants such as sodium hypochlorite at 1000 ppm or products proven to be virucidal (H100, H200, etc.);
- none-
facilitate the tasks of cleaning and disinfection staff, leaving the workspace as free as possible. A frequent cleaning and disinfection strategy is necessary for common areas: light switches, countertops, chair arms, stair railings, lift buttons, door knobs, etc.21;
- none-
immediately report any respiratory symptoms or low-grade fever if they have had close contact (less than 2 m) with a probable or confirmed case;
- none-
stay home when they are unwell, notifying the centre by telephone and following the protocol indicated by their centre.
One of the first measures taken by the Spanish Ministry of Health, before decreeing the state of national alarm and the confinement of the entire population22, was to recommend that the autonomous regions not organise congresses, workshops, seminars or training courses for healthcare professionals, other than routine events within their own services, in order to guarantee the availability of this group in their usual care-provision services and prevent them from acting as transmitters of the disease to the most vulnerable population groups23. High-risk contacts (close contact with a probable/confirmed case without personal protective equipment) among healthcare professionals can also occur during normal activity in the workplace, between individuals from the same team, who are apparently healthy and asymptomatic24 and are not aware of having been exposed to the virus. In a hospital in Taipei, 17 healthcare professionals were infected by SARS despite not coming into direct contact with infected patients, and virus RNA was detected on surfaces in "clean" areas.25 The consequences of this type of transmission are a large number of people from the same department being on sick leave, and the ensuing problems in guaranteeing healthcare provision.
The restrictions regarding gatherings of people that apply to the general population must also be applied at the hospital/service/centre level, especially when they are dealing with an at-risk population, as mentioned above. The measures to be adopted entail a change in customs adapted to the situation, and a high degree of commitment from the centre. Strategies aimed at protecting healthcare professionals include12,25:
- none-
restricting the number of healthcare professionals who access the facilities and limiting the total number of staff dedicated to patient care;
- none-
encouraging healthcare personnel to remain within the hospital only the time essential for carrying out their care provision tasks;
- none-
promoting teleworking by facilitating remote access to the hospital’s medical records, which will avoid putting patients and healthcare professionals at risk, and allow them to work from home;
- none-
suspending department clinical sessions and face-to-face hand-over sessions for shift changes for which modern communication tools can be used, such as free videoconferences that enable several people to connect from different places (Zoom, Skype, Microsoft Teams, etc.);
- none-
in areas where the work is carried out by several people (residents and assistants), distributing the patients to avoid more than one person attending to each patient, and having discussions and information sharing via WhatsApp or by telephone;
- none-
if possible, working in separate offices. If more than one person share an office, they should be more than 2 m apart; whenever possible, the space should be kept well ventilated;
- none-
avoiding busy places in the hospital (cafeteria) and not having meals or breaks together or using the lifts if safe distancing cannot be maintained.
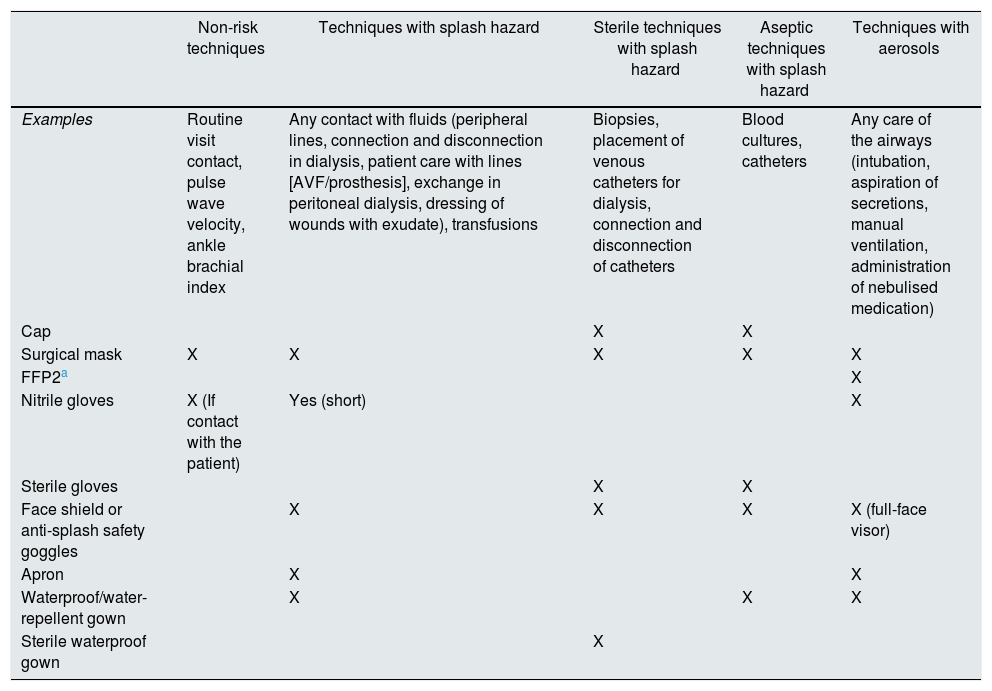
Healthcare personnel who treat kidney patients carry out specific activities with varying degrees of complexity which require different protective measures, depending on the need for asepsis or the risk of splashing and presence of aerosols. These measures and the protective equipment necessary in each case are summarised in Table 1.26–31
Protective measures for carrying out testing and activities related to nephrology in the current context of the COVID-19 pandemic.
| Non-risk techniques | Techniques with splash hazard | Sterile techniques with splash hazard | Aseptic techniques with splash hazard | Techniques with aerosols | |
|---|---|---|---|---|---|
| Examples | Routine visit contact, pulse wave velocity, ankle brachial index | Any contact with fluids (peripheral lines, connection and disconnection in dialysis, patient care with lines [AVF/prosthesis], exchange in peritoneal dialysis, dressing of wounds with exudate), transfusions | Biopsies, placement of venous catheters for dialysis, connection and disconnection of catheters | Blood cultures, catheters | Any care of the airways (intubation, aspiration of secretions, manual ventilation, administration of nebulised medication) |
| Cap | X | X | |||
| Surgical mask | X | X | X | X | X |
| FFP2a | X | ||||
| Nitrile gloves | X (If contact with the patient) | Yes (short) | X | ||
| Sterile gloves | X | X | |||
| Face shield or anti-splash safety goggles | X | X | X | X (full-face visor) | |
| Apron | X | X | |||
| Waterproof/water-repellent gown | X | X | X | ||
| Sterile waterproof gown | X |
- a
Special care or protective measures for medical, nursing and auxiliary staff who work daily with haemodialysis patients
As has previously been described in other publications3,10, the main protection measures for healthcare professionals and patients in haemodialysis units are: 1) adequate information for patients attending the centre in terms of maintaining a safe distance from fellow patients in waiting rooms and ambulances, and in the use of surgical masks and frequent hand washing; 2) early detection of patients suspected to be infected on arrival at the unit (questionnaires about symptoms or close contacts, taking temperature), and if highly suspect, taking a nasopharyngeal swab for PCR testing.
Protective equipment varies depending on the unit’s policy regarding patient screening for COVID-19:
- none-
In units seeing patients who have COVID-19 or units where no general SARS-CoV-2 PCR and/or serology screening is performed, the protective equipment should include all the elements recommended for COVID-19 units, due to the high proportion of infected patients who are asymptomatic; in some Spanish dialysis units, this figure is as high as 40%.3 This equipment includes a heavy-duty surgical gown, waterproof apron, cap, FFP2 mask with a surgical mask over it to protect it from external contamination and prevent droplet transmission by the healthcare professional if the FFP2 has a filter3,10, double gloves (one long pair over the gown and other short), and googles or face shield, with a protocol for putting on and taking off the PPE to avoid contamination which includes changing gloves between patients, with alcohol-solution hygiene before and after the change3,18.
- none-
In units where the population cared for is screened and patients are known to be negative, the use of a surgical mask and gloves is sufficient, but with the addition of a waterproof gown or a heavy-duty surgical gown with a waterproof apron and protective screen for the connection and disconnection of, and care of patients with lines. Gowns and gloves should be changed between patients. The same isolation gown should not be used for the care of more than one patient, except if they are isolated together (isolation of cohorts) with adequate hand washing after removal of both and before attending to the next patient (Table 1).
Bedside visits to the haemodialysis patient, whether in the hospital or a peripheral centre, should only be made by one doctor at a time. Each doctor should always see the same patients, unless they require help from another colleague for the assessment, in which case they should see the patient separately.
Nursing staff should also always attend to the same patients, to make it easier to trace exposed workers. It is important that staffing levels be adjusted to cover the added difficulty of caring for patients infected with COVID-19. One direct care nurse has been recommended for every 3–4 patients, and one nurse for every 7–8 patients, who acts as a "mirror" helping with medication, preparation of material, management of medical records, etc., and one nursing assistant every 5–7 patients who also acts as a "mirror".3
At the end of the shift, deep cleaning of surfaces, monitors, floors and walls should be carried out in the unit. Devices such as pulse oximeters, thermometers and sphygmomanometers should be cleaned between patients with virucidal substances or sodium hypochlorite, with this measure being applied in all work areas.19,20
Of particular interest in the prevention of transmission to patients and healthcare workers is the reincorporation into the units of patients who have been infected by COVID in isolation areas. After seven days free of symptoms, the recommendation is to repeat the PCR test with an interval of 48 h and, if both are negative, incorporate them normally with the rest of the patients.32
- b
Special care or protection measures for staff working in peritoneal dialysis (training, etc.)
Specialised diagnosis and treatment related to peritoneal dialysis and its complications should be provided by the nephrologist via phone, WhatsApp or the Internet.
Assessments should be carried out to exclude the presence of suspected or probable COVID-19 among patients and caregivers.
During admission, to minimise the risk of infection, the recommendation is to substitute automated peritoneal dialysis (APD) for continuous ambulatory peritoneal dialysis (CAPD), reducing the number of connections and exchanges, and thus reducing the possibility of contact infection. If the patient’s medical condition is such that they cannot self-administer the dialysis, they will be put on haemodialysis while in hospital.33
Any surfaces, supplies or equipment located in rooms where suspect patients have been dialysed should be disinfected or discarded.
For training, the nurse should use the individual protection equipment described in Table 1 (surgical mask with a face shield on top, gloves and a waterproof gown or a heavy-duty surgical gown with a waterproof apron). The patient should wear a surgical mask and gloves and their companion should also wear personal protective equipment similar to that of the nursing staff. The same precautions already described should be taken after removal of the protective equipment, with suitable hand hygiene before and after.
Measures and recommendations for staff working in hospitalisation areas or in acute nephrology unitsBefore admission to hospital, patients will be examined to assess their risk of exposure to COVID-19 and the presence of symptoms, including a nasopharyngeal swab and PCR test, so that they can be appropriately placed within the assigned admission areas (COVID ward, suspect ward or negative ward).
As long as the number of patients with COVID-19 is high, it is advisable to group them together in confined wards to limit the number of exposed healthcare staff and conserve supplies. In these COVID-19 wards, the staff should wear individual protective equipment and will not need to change it between patients (isolation of cohorts).
On negative hospital wards (negative PCR on admission), although the risk is low, as preventive measures during the COVID-19 epidemic, gloves and a surgical mask should be worn to enter the room, unless there is a risk of aerosols, when a FFP2 mask should be worn covered with a disposable surgical mask and, provided there is no risk of splashing, a disposable conventional gown. If there is a risk of splashing, a face shield or goggles should be worn and a waterproof apron should be placed over the gown, which should be discarded at the end of the visit. Hand hygiene should be performed before and after the provision of care to each of the patients. The protective measures should be adapted to the type of activity to be carried out (Table 1).
Before leaving the room, the PPE (gloves, screen and gown) should be removed, taking special care to avoid touching the outer surfaces of the gloves and gown. These items should be left inside the room in a place specifically provided for that purpose; staff should never go out into the corridor with gloves or a gown. After removing the protective equipment, they should wash their hands.
In the case of hospitalised patients, healthcare staff should spend the minimum time possible in the room. Only those who need attention and require an examination should be approached, and this should be done with the PPE described. Bedside visits to hospitalised patients should only be performed by one doctor at a time. Each doctor should always see the same patients, unless they require help from another colleague for the assessment, in which case they should see the patient separately.
Measures and recommendations for the staff of the nephrology and kidney transplant clinicsWhile the pandemic continues, face-to-face patient consultations in nephrology clinics, whatever the type (transplant, waiting list, clinical nephrology, CKD), should as far as possible be kept to a minimum. It is imperative for telemedicine to help close the gap created by the pandemic and extend our reach in the future, and for that reason it is already being widely applied, including in a number of surgical specialities.34,35
For patients with stable kidney function, lengthening the interval between outpatient visits is recommended to avoid patient visits to the hospital. In addition to giving preference to telephone and telematic care, strategies for coordination with primary care should be developed, promoting health centres having their healthcare staff carry out analyses at home.
As in all areas, measures will be carried out aimed at the early identification of suspected infection among patients (questionnaires about symptoms or close contacts, taking temperature) and, if suspected, a PCR nasopharyngeal swab test will be carried out.
If there is no alternative to a face-to-face consultation in the outpatient clinic, the visit should be held as quickly as possible and, if necessary, continued by telephone. Patients to be seen in the clinic should arrive at staggered times with minimum waiting time, ensuring that there is only one doctor and one patient in each consultation, maintaining a distance of more than 2 m between them. A family member should only enter if absolutely necessary. Face-to-face consultation in the clinic is considered a low-risk activity, so the use of a surgical mask is sufficient, both by the patient and the healthcare professional. If contact with the patient is necessary, gloves should be worn, with suitable hand hygiene both before and after.
Similarly, strict measures for cleaning and disinfection of the consulting room and surfaces must be applied, the central air conditioning should be turned off and good ventilation maintained.36
Measures and recommendations aimed at staff who perform invasive procedures (kidney biopsy, placement of tenckhoff catheters for peritoneal dialysis or catheters for haemodialysis, etc.)In patients who require invasive procedures, such as kidney biopsy or catheter placement, a SARS-CoV-2 PCR test should be determined 24 h before the procedure, in order to appropriately allocate positive patients to a specially dedicated operating theatre. As shown in Table 1, biopsies and catheter placement are considered activities requiring sterile conditions where there is a risk of splashing, so the equipment to be used should include sterile gloves and gown, in addition to the other protection already mentioned.
Psychological protection for healthcare professionalsHealthcare workers’ need for protection in this pandemic is not limited exclusively to their exposure to transmission. In a study of 994 healthcare professionals in the province of Wuhan, almost 40% developed psychological disorders immediately after the epidemic. These disorders mainly involved anxiety, which required different types of psychological support and mainly affected young women.37
Although the fear of self-infection is accepted by most healthcare professionals, many express concern about being vehicles of transmission to their own families, especially to family members who are older, immunocompromised or have chronic diseases.18
Moreover, carrying out haemodialysis on infected patients involves added factors, such as prolonged exposure for a number of hours, alone and wearing protective equipment, all elements which can increase the state of anxiety. These findings highlight the importance of being prepared to support frontline workers through mental health interventions in times of widespread crisis.38
Key points- •
Self-protection is the responsibility of all staff providing care for people with kidney disease.
- •
Contact between healthcare professionals is a risk factor for nosocomial transmission in hospitals and health centres. Modifying the way we interrelate with each other is a priority if we are to stop the spread of the virus and guarantee healthcare to all those who need it, not only in our speciality but in the hospital as a whole.
- •
Strict compliance with standard, droplet and contact precautions with adequate protection is the responsibility of healthcare personnel providing care for suspected or diagnosed cases of COVID-19.
- •
Meeting the emotional and psychological needs of healthcare personnel is essential in crisis situations such as the current pandemic.
The authors declare that they have no conflicts of interest.
Please cite this article as: Arenas MD, Villar J, González C, Cao H, Collado S, Barbosa F, et al. Protección de los profesionales sanitarios en nefrología ante la pandemia por COVID-19. Nefrologia. 2020;40:395–401.



