
Anaphylactic or anaphylactoid reactions during hemodialysis (HD) have been recorded since 1975.1 The bio-incompatibility of the materials may be the cause.2
In the last decade, reactions associated with the use of synthetic membranes, generally polysulfones, have been described as “allergic”, “hypersensitive” or “anaphylactic”.1,3–5
The different forms of presentation, from more to less frequent, are: dyspnea, hypotension, bronchospasm, cough, vomiting and other GI symptoms, precordial pain, pruritus, urticaria, fever, headache and confusion. Eosinophilia, increased serum tryptase or hypocomplementemia help in differential diagnosis.6
Allergic reactions to synthetic hemodialysis membranes have been described with the use of different membranes: polysulfone, polyethersulfone, polynephrone, polyarylethersulfone and polyacrylonitrile.4,7 If changed to cellulose triacetate (CT) membranes, there were no further reactions.5,8
Rodríguez-Sanz et al. conclude that basophil degranulation and elevated tryptase levels, which occurred during the acute reaction in 7 patients, that were allergic to synthetic membranes, demonstrate that there is the activation of mast cells and basophils.9 Years later, the same authors performed a study in 29 patients using polysulfone membranes and found alterations in tryptase levels, complement activation and interleukin-6 (IL-6) levels during acute reactions.10
Our main objective was to measure serum levels of tryptase, IL-6, complement (C3 and C4) in 3 groups of dialyzers: Group 1, synthetic membranes in post-dilution online hemodiafiltration (HDFOL), Group 2 with asymmetric TAC membranes (TACA) in HDFOL and Group 3 with synthetic membranes in extended HD (HDx).
As secondary objectives we observed the association of the presence of lymphopenia, eosinophilia, thrombocytopenia and chronic pruritus among the group of patients with allergies to synthetic membranes (using TACA membranes) vs. patients without allergies to these synthetic membranes.
This is an observational, retrospective, cross-sectional, descriptive-comparative, retrospective study of all patients in the hemodialysis unit of the Hospital Universitario Infanta Sofía older than 18 years of age who have been on HD for more than 3 months and with the same dialysis membrane for more than one month.
Statistical analysis was performed with SPSS® version 25 software.
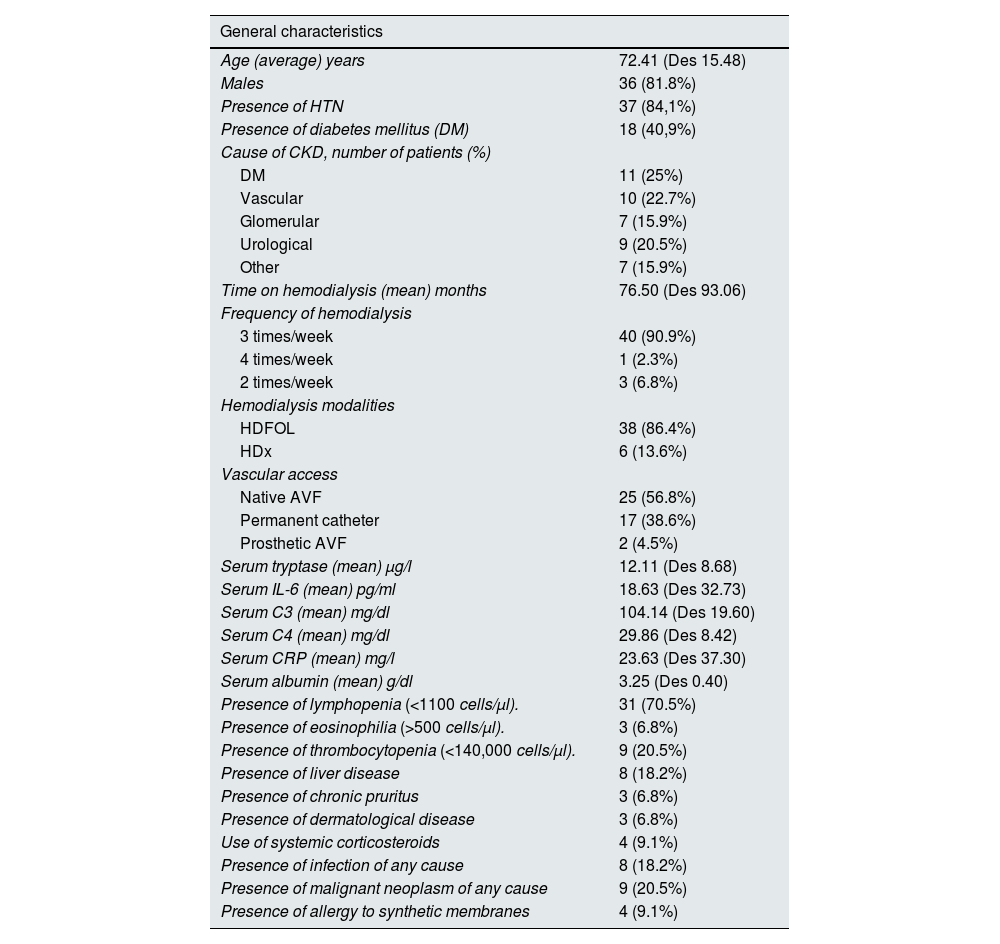
We analyzed 53 patients from the hemodialysis unit of our hospital, and excluded 9 patients (6 due to time on dialysis of less than 3 months, 1 patient in an ultrafiltration program due to severe heart failure and 2 patients due to the use of drugs that bind to the IL-6 receptor). The general data are described in Table 1.
General data of the patients studied.
| General characteristics | |
|---|---|
| Age (average) years | 72.41 (Des 15.48) |
| Males | 36 (81.8%) |
| Presence of HTN | 37 (84,1%) |
| Presence of diabetes mellitus (DM) | 18 (40,9%) |
| Cause of CKD, number of patients (%) | |
| DM | 11 (25%) |
| Vascular | 10 (22.7%) |
| Glomerular | 7 (15.9%) |
| Urological | 9 (20.5%) |
| Other | 7 (15.9%) |
| Time on hemodialysis (mean) months | 76.50 (Des 93.06) |
| Frequency of hemodialysis | |
| 3 times/week | 40 (90.9%) |
| 4 times/week | 1 (2.3%) |
| 2 times/week | 3 (6.8%) |
| Hemodialysis modalities | |
| HDFOL | 38 (86.4%) |
| HDx | 6 (13.6%) |
| Vascular access | |
| Native AVF | 25 (56.8%) |
| Permanent catheter | 17 (38.6%) |
| Prosthetic AVF | 2 (4.5%) |
| Serum tryptase (mean) µg/l | 12.11 (Des 8.68) |
| Serum IL-6 (mean) pg/ml | 18.63 (Des 32.73) |
| Serum C3 (mean) mg/dl | 104.14 (Des 19.60) |
| Serum C4 (mean) mg/dl | 29.86 (Des 8.42) |
| Serum CRP (mean) mg/l | 23.63 (Des 37.30) |
| Serum albumin (mean) g/dl | 3.25 (Des 0.40) |
| Presence of lymphopenia (<1100 cells/µl). | 31 (70.5%) |
| Presence of eosinophilia (>500 cells/µl). | 3 (6.8%) |
| Presence of thrombocytopenia (<140,000 cells/µl). | 9 (20.5%) |
| Presence of liver disease | 8 (18.2%) |
| Presence of chronic pruritus | 3 (6.8%) |
| Presence of dermatological disease | 3 (6.8%) |
| Use of systemic corticosteroids | 4 (9.1%) |
| Presence of infection of any cause | 8 (18.2%) |
| Presence of malignant neoplasm of any cause | 9 (20.5%) |
| Presence of allergy to synthetic membranes | 4 (9.1%) |
The most commonly used dialyzers were Polyflux 210H® and Fx cordiax 1000®. The use of Solacea 21H® was 9.1% and of Theranova 500® was 13.6%.
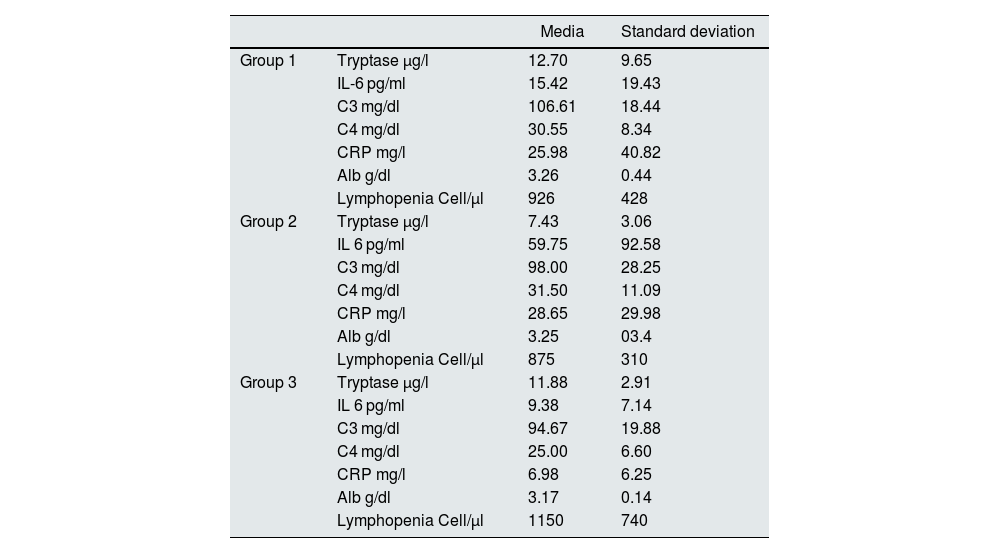
The analysis of tryptase levels, complement C3/C4 and IL-6 are in Table 2. Tryptase levels are lower in the asymmetric cellulose triacetate (TACA) membrane (second group) in HDFOL, however, IL-6 levels are lower in the third synthetic membrane group with MCO in HDx.
Differences in biochemistry in dialyzer membranes.
| Media | Standard deviation | ||
|---|---|---|---|
| Group 1 | Tryptase µg/l | 12.70 | 9.65 |
| IL-6 pg/ml | 15.42 | 19.43 | |
| C3 mg/dl | 106.61 | 18.44 | |
| C4 mg/dl | 30.55 | 8.34 | |
| CRP mg/l | 25.98 | 40.82 | |
| Alb g/dl | 3.26 | 0.44 | |
| Lymphopenia Cell/µl | 926 | 428 | |
| Group 2 | Tryptase µg/l | 7.43 | 3.06 |
| IL 6 pg/ml | 59.75 | 92.58 | |
| C3 mg/dl | 98.00 | 28.25 | |
| C4 mg/dl | 31.50 | 11.09 | |
| CRP mg/l | 28.65 | 29.98 | |
| Alb g/dl | 3.25 | 03.4 | |
| Lymphopenia Cell/µl | 875 | 310 | |
| Group 3 | Tryptase µg/l | 11.88 | 2.91 |
| IL 6 pg/ml | 9.38 | 7.14 | |
| C3 mg/dl | 94.67 | 19.88 | |
| C4 mg/dl | 25.00 | 6.60 | |
| CRP mg/l | 6.98 | 6.25 | |
| Alb g/dl | 3.17 | 0.14 | |
| Lymphopenia Cell/µl | 1150 | 740 |
The statistical analysis of non-parametric tests (Kruskal Wallis test), revealed no significant differences between the levels of the 4 markers (tryptase, IL-6, C3 and C4) in the 3 groups, but analysis of the difference between the TACA membranes in HDFOL (Group 2) vs. the other two groups (Group 1 and 3 together), shows a tendency toward lower tryptase levels, with a p = 0.09 (Mann–Whitney U test).
Regarding the presence of lymphopenia, eosinophilia, thrombocytopenia and chronic pruritus we compared the group of patients with allergy to synthetic membranes (using TACA membranes) with patients without allergy to synthetic membranes and found no significant differences (Fisher’s exact test), with values of p = 0.66 for lymphopenia, p = 0.75 for eosinophilia, p = 0.614 for thrombocytopenia and p = 0.746 for chronic pruritus. But it is worth mentioning that none of the 4 patients with TACA membrane had chronic pruritus or eosinophilia.
The serum levels of IL-6 was associated to pruritus, p = 0.47 (Mann–Whitney U test).
In conclusion we found that tryptase levels are lower in HD patients using TACA membranes, probably indicating a smaller reaction to this membrane.
The study also showed that in the TACA group no patient had eosinophilia or pruritus.
In the present study, tryptase, IL-6, C3 and C4 levels did not change with age, sex, time on HD, presence of DM or hypertension, but an association was found between high IL-6 levels and pruritus.
Financial supportThis work has not received any funding.



