

Haemodialysis is the method of choice for renal function replacement therapy during pregnancy and the postpartum period.1 Peritoneal dialysis is an uncommon procedure in this type of patient.2 Placement of a Tenckhoff soft catheter has been described after caesarean section for the immediate start of the dialysis process in selected cases.3 The placement of a rigid catheter is even more restricted because it is a “blind” technique that can be complicated by haemorrhage, laceration or perforation of the intestine, colon, bladder, or of the uterus, which is occupied by the foetus, and its annexes, but in the postpartum period its contraindication is relative.2
We present 4 pregnant patients with pre-eclampsia and complications from acute kidney injury (AKI), who underwent acute peritoneal dialysis in the Intensive Care Unit (ICU) using a rigid abdominal catheter after termination of pregnancy with caesarean section (Fig. 1). The mean age was 30.7±3.4 years and that of pregnancy was 32.0±3.2 weeks. All had a diagnosis of severe pre-eclampsia as well as HELLP syndrome (3 cases) and eclampsia (1 case). The caesarean section was performed after receiving critical care. During surgery no infection (cellulitis, abscesses, chorioamnionitis, peritonitis), “hyperthermic” cavity, haematoma or active bleeding were observed, no packing or drains were placed and there were no potential leakage sites (Penrose, Saratoga, open vaginal vault, wound dehiscence, open abdominal cavity). The hysterorrhaphy and soft-tissue wound were perfectly sealed.

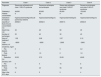
After the surgery, they were admitted again in the ICU. To treat the AKI, a rigid abdominal catheter was placed using the technique previously described.2 The indications were nitrogen retention, oliguria and cardiopulmonary compromise. The method was selected because haemodialysis was not available in the ICU and because their clinical condition did not allow for safe transfer to the nearest haemodialysis unit. When the catheter was placed, average platelet count was 81,750/μl; 8 and 9 platelet concentrates were administered in both cases. All 4 patients received a single peritoneal dialysis session; 2000ml of dialysis fluid were infused manually from the first exchange, with good tolerance to distension, and a dwell time of at least 45min. Between 30 and 40 exchanges were performed, and −4225ml of clear liquid was obtained, on average. The catheter remained for 2.29 days on average. There were no technical complications, and the indications for catheter removal were decreased serum creatinine, recovery of diuresis, and clinical improvement. The average stay in the ICU was 5 days, and the survival rate was 100% (Table 1).
Peritoneal dialysis with rigid catheter.
| Parameter | Case 1 | Case 2 | Case 3 | Case 4 |
|---|---|---|---|---|
| Diagnosis | Severe pre-eclampsia and class 1 HELLP syndrome | Severe pre-eclampsia and eclampsia | Severe pre-eclampsia and class 2 HELLP syndrome | Severe pre-eclampsia and class 3 HELLP syndrome |
| Platelets/μl | 49,000 | 95,000 | 60,000 | 123,000 |
| Platelet concentrates | 8 | No | 9 | No |
| Indications for dialysis | HyperazotaemiaOliguriaAcute pulmonary oedema | HyperazotaemiaOliguria | HyperazotaemiaOliguria | HyperazotaemiaOliguria |
| Quantity of fluid (ml) and concentration (%) | 20002.5 | 20002.5 | 20001.5 | 20002.5 |
| Dwell time, min | 45 | 45 | 60 | 45 |
| Number of exchanges | 30 | 40 | 30 | 40 |
| Days of treatmenta | 1.58 | 2.08 | 3.37 | 2.12 |
| Total balance, ml | −8000 | −3000 | −2000 | −3900 |
| Creatinine, mg/dl | ||||
| Pre-dialysis | 6 | 4 | 6 | 4.2 |
| Post-dialysis | 2 | 1.5 | 2 | 1.8 |
| Reduction (%) | 33.33 | 37.5 | 33.33 | 42.85 |
| Diuresis, ml/h | ||||
| Pre-dialysis | 5 | 5 | 15 | 8 |
| Post-dialysis | 75 | 45 | 55 | 80 |
| Stay in the ICU, days | 6 | 5 | 5 | 4 |
Peritoneal dialysis with rigid catheter is part of the training for nephrologists, internists, emergency physicians and specialists in critical medicine. In Mexico, the technique, indications, complications and their management have been established in paediatric and adult patients.4,5 International literature also offers similar information,6,7 but not for pregnant women.
In 2006, Briones-Garduño et al.3 published the results of acute peritoneal dialysis with a Tenckhoff soft catheter in 6 pre-eclamptic patients with AKI in the postpartum period. They found that the method was safe from the technical point of view, and that it achieved an improvement in renal function. This study describes 4 pre-eclamptic patients undergoing caesarean section, complicated with AKI, whose dialysis indications were well identified.2 The rigid catheter was placed only after clotting abnormalities had been corrected, bleeding had stopped, no signs of infection, and the abdominal cavity had been closed. The placement, permanence and removal of the catheter were uneventful. The infusion of 2000ml from the start of dialysis was well tolerated, and the choice of glucose concentration in the solutions was consistent with the intention to perform ultrafiltration4–6 (Table 1).
There are no reports in the literature on the peritoneal membrane and its dialysance in this type of patient. In the report by Briones-Garduño et al.,3 serum creatinine values were the gold standard, and their reduction was interpreted as recovery of renal function; the same was true in the 4 patients in this study, as predialysis creatinine values fell by 36.75% by the end of the treatment, and diuresis had evidently increased (Table 1). The possibility of considering puerperal status as a relative contraindication for peritoneal dialysis with a rigid catheter is related to the technical aspects, but not the dialysance of the peritoneal membrane. It should be considered as a useful method for obstetric care centres with no access to haemodialysis.
Please cite this article as: Vázquez-Rodríguez JG. Diálisis peritoneal posparto con catéter rígido en pacientes preeclámpsicas intervenidas de cesárea. Reporte de 4 casos. Nefrologia. 2019;39:444–446.



