


IgA nephropathy (IgAN) is characterized by glomerulonephritis (GN) with predominant IgA immune deposits. Idiopathic IgAN is the most common cause of glomerular IgA deposition and the most common GN worldwide. We have encountered an increase in the frequency of an uncommon secondary form of IgAN in renal biopsies over a recent 7-month period (December 2016 to June 2017), likely related to bacterial infections. All native kidney biopsies received at our laboratory are processed routinely for light, immunofluorescence (IF) and electron microscopy (EM). Of 310 native renal biopsies received over this period, 49 (15.8%) had predominant IgA deposits. Twenty-seven of these had idiopathic IgAN, 5 had incidental minimal mesangial IgA deposits, and 17 biopsies had features of IgA infection-related (IR) GN. On histologic evaluation, 11 of 17 IgA IRGN had proliferative and exudative GN with or without crescents, and 6 had resolving GN with minimal or mild mesangial proliferation. Both IF and EM revealed characteristic coarse granular capillary wall and mesangial deposits of IgA and complement component C3 in a pattern distinct from idiopathic IgAN (Figs. 1 and 2). Subepithelial (100%), subepithelial hump-like (67%), subendothelial (50%) and mesangial (100%) electron dense deposits were identified on EM (Fig. 2). Acute tubular necrosis or interstitial nephritis was present in all 17 biopsies.
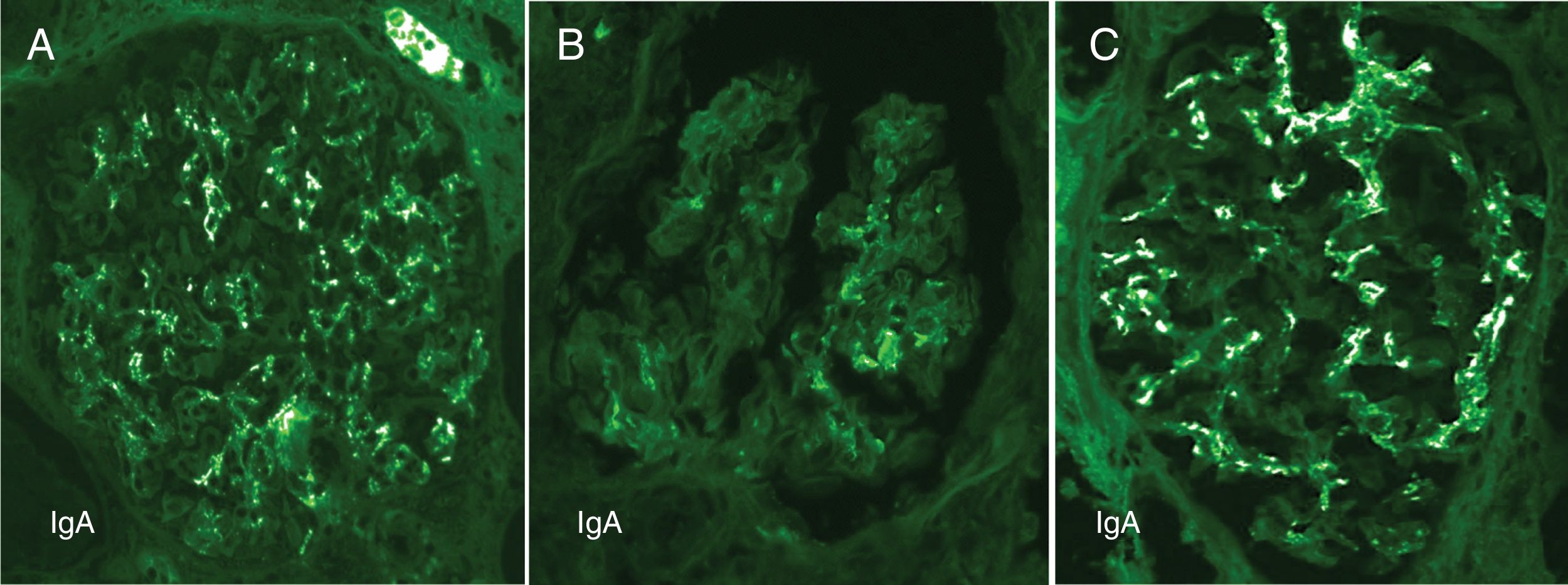
Contrasting features of IgA dominant IRGN and idiopathic IgAN.
Mesangial and capillary wall coarse granular deposits are prominent in exudative IgA IRGN (A) and less so in resolving IgA IRGN (B). These immunofluorescence patterns contrast with the largely mesangial deposits of IgA in idiopathic IgAN (C).
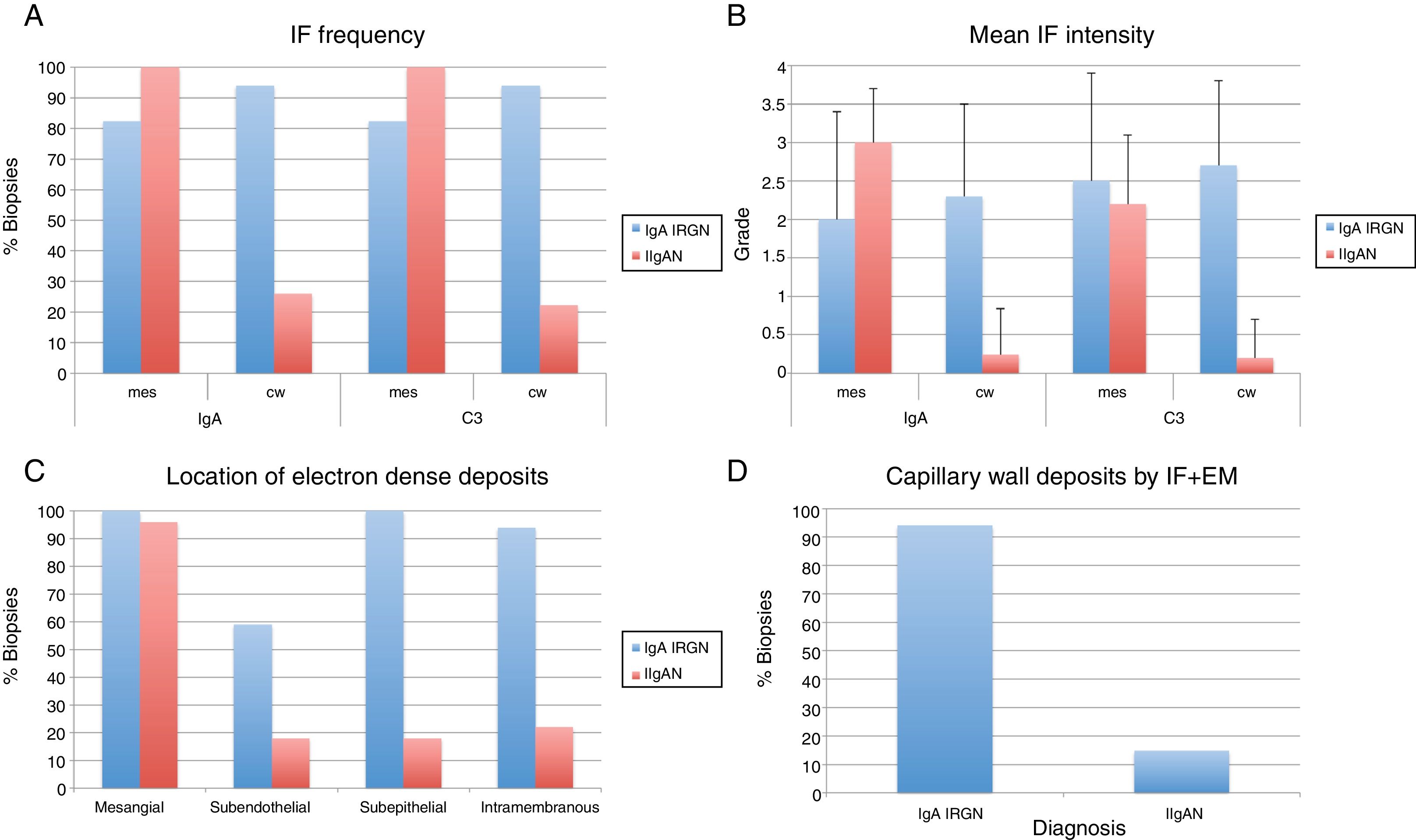
Analysis of immunofluorescence and electron microscopic features of IgA IRGN and idiopathic IgAN.
Mesangial deposits of IgA and C3 were seen with comparable frequency in IgA IRGN and idiopathic IgAN, however, there were more frequent (A) and intense (B) deposits of these reactants in the glomerular capillary walls (p<0.001 by Fisher Exact and Mann–Whitney tests respectively). Capillary wall deposits were more frequently observed by EM in IgA IRGN compared with idiopathic IgAN (C). Ninety-four percent of IgA IRGN had capillary wall deposits detectable by both IF and EM compared with 14.8% of idiopathic IgAN (D).
All patients were adults (mean age 55.5 years (range 30–93)), with acute kidney injury in 16 of 17 (mean serum creatinine 3.9±3mg/dL), proteinuria (4 in the nephrotic range) and hematuria. Seven patients had diabetes mellitus, 4 of whom had diabetic nephropathy. Twelve had known clinical features of recent or concurrent bacterial infection (involving skin 7, joint 1, lung 2, appendix 1, vascular graft 1), 6 of which had culture positive S. aureus. In 6 cases the organism is unknown to us, and 5 patients had limited available clinical data. Of 10 patients with available follow-up data, 6 developed end-stage kidney disease, 3 had partial recovery and 1 had complete recovery of renal function.
Acute or resolving IgA IRGN accounted for nearly 35% of renal biopsies with IgA deposits and 5.5% of all native renal biopsies received over the study period. For perspective, a review of 21 339 native kidney biopsies obtained in the United States and Canada over approximately 20 years, suggests a frequency of about 0.6% for IgA IRGN.1–4 Our observations show a 9-fold increase in frequency of IgA IRGN albeit in a small single practice sample over a short time span. IgA IRGN has distinctive features including strong C3 staining, capillary wall immune deposits and acute tubulointerstitial injury, but may be difficult to distinguish from idiopathic IgAN, a feature noted by others.5 IRGN may be a more significant differential diagnostic consideration in biopsies with predominant glomerular IgA deposition than has been generally recognized.



