

dRTA is a genetic or acquired rare disease, characterized by an unability to excrete hydrogens (H+) into urine, hypobicarbonatemia, hyperchloremia, and frequently hypercalciuria and hypokalaemia. Genetic forms are usually diagnosed during the first months of life and its treatment is based on providing alkali supplements in order to prevent long term clinical consequences, particularly chronic kidney disease (described in some cohorts up to 82% of dRTA patients) and the associated bone disease. A 10 queries multi choice closed response survey was designed to know more about epidemiological, diagnostics, clinical management and therapeutical issues of this disease among Spanish nephrologists.
Methods and materialsThis survey was delivered to the attendees to a scientific meeting on dRTA at the Spanish Nephrology Society congress in 2019. Surveys were collected at the end of this dRTA event. Results were analyzed by using a parametric statistical test, obtaining the percentage of each response for the 10 questions. Results. Among the survey responders, 44.4% and 37.7% did not visit any dRTA patient during the 1st and 3rd last year respectively. When having a suspicious diagnose, confirming genetic diagnostic test is only performed on the 13.3% of cases and pedigree studies only on 11.1%. Only a 26.6% confirms that metabolic control is excellent, good or very good. 69% of the responders believe that treatment compliance is not bad, bad or very bad.
ConclusionsThis survey enhances the fact that dRTA is not a well known entity, satisfaction with metabolic control is poor and compliance is low. All these factors can lead to a higher severity of renal and bone diseases associated to dRTA.
La ATRd es una enfermedad minoritaria de origen genético o adquirido, caracterizada por una incapacidad de excreción urinaria de hidrogeniones (H+), hipobicarbonatemia, hipercloremia, hipocitraturia y habitualmente hipokaliemia e hipercalciuria. Las formas genéticas suelen diagnosticarse en los primeros meses de vida y su tratamiento consiste en suplementos de álcali encaminados a evitar las consecuencias clínicas a largo plazo, sobre todo la enfermedad renal crónica (presente en algunas series hasta en el 82% de los pacientes) y la enfermedad ósea asociada. Se desarrolló una encuesta multirrespuesta cerrada de 10 preguntas encaminada a conocer aspectos epidemiológicos, diagnósticos, del manejo clínico y terapéutico, dentro del colectivo de nefrólogos españoles.
Materiales y métodosEncuesta distribuida a los asistentes a un foro científico sobre ATRd durante el congreso de 2019 de la Sociedad Española de Nefrología (SEN), se recogieron las respuestas a la salida del mismo. Los resultados se analizaron con un test estadístico paramétrico estableciéndose el porcentaje de cada respuesta las 10 preguntas. Resultados. De entre los que respondieron a la encuesta, un 44,4% y un 37,7% no atendió ningún paciente con ATRd en el último año ni en los 3 anteriores, respectivamente. Cuando se sospecha la patología, el diagnóstico genético confirmatorio se realiza solo en un 13,3% de los casos y el estudio familiar solo en un 11,1%. Solo un 26,6% afirma que el control metabólico es excelente, bueno o muy bueno, y el 69% piensa que el cumplimiento terapéutico es regular, malo o muy malo.
ConclusionesLa encuesta ha puesto de manifiesto el relativo desconocimiento de esta patología, así como la baja satisfacción con el control metabólico y el pobre cumplimiento terapéutico, lo cual puede conllevar a una mayor severidad en la enfermedad renal y ósea asociadas a la ATRd.
Distal renal tubular acidosis (dRTA) is one of the most prevalent renal tubular disorders within a group of diseases considered rare or minority. dRTA can be inherited or acquired, with a reported estimated prevalence of 0.46/10,000 inhabitants.1 However, the prevalence of primary or hereditary dRTA is less than one case per 100,000 inhabitants, meaning that in Spain the total number of patients diagnosed with primary dRTA would be between 300 and 400.2 This disease is diagnosed in the first months, or even days, of life and should be suspected in children with nausea, vomiting, a certain degree of dehydration, polydipsia and polyuria, as well as poor weight gain or growth, who also present with hypobicarbonataemia, hyperchloraemia and anion GAP in normal blood. Additionally, it usually manifests with hypokalaemia. In urine it is characteristic to find hypercalciuria, hypocitraturia, pH>5.5 and positive anion GAP in coexistence with metabolic acidosis.
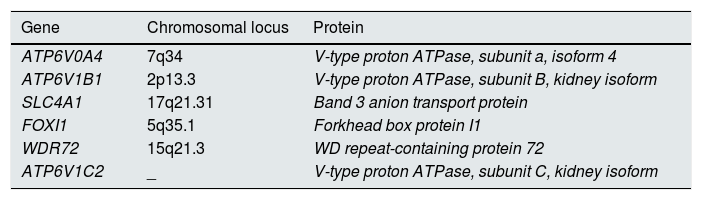
Primary dRTA presents an autosomal recessive inheritance pattern in most cases, six genes have been described to be involved in this disease (Table 1). The most common in our setting (more than 80%) are those that encode for the V1B1 and V0A4 subunits of the H+ATPase pump; more specifically, the genes ATP6V1B1 and ATPV0A4. The pathophysiological consequence of the alteration of the H+ATPase pump is the inability to excrete hydrogen ions into the lumen of the tubule, generating urine with a more alkaline pH (and an inability to acidify the urine in the event of excess acid in the blood). In total, 15% of the mutations are attributable to the SLC4A1gene, which will affect the normal configuration of the chloride/bicarbonate anion exchanger located in the membrane of the alpha intercalated cell, on the face closest to the blood capillary. Alterations in the chloride/bicarbonate exchanger will result in hyperchloraemia (as the chloride does not fully enter the alpha intercalated cell) and hypobicarbonataemia (the normal functioning of the exchanger is impaired). Moreover, it is interesting to note that the SLC4A1 gene can present autosomal recessive or dominant inheritance, giving rise in the latter case to less severe clinical symptoms that usually results in a later diagnosis and added difficulty. Other responsible genes described in isolated cases are FOXI1, WDR72 and ATP6V1C2, the latter recently reported in October 2019.3
Genes identified in the pathogenesis of distal renal tubular acidosis and the protein they encode.
| Gene | Chromosomal locus | Protein |
|---|---|---|
| ATP6V0A4 | 7q34 | V-type proton ATPase, subunit a, isoform 4 |
| ATP6V1B1 | 2p13.3 | V-type proton ATPase, subunit B, kidney isoform |
| SLC4A1 | 17q21.31 | Band 3 anion transport protein |
| FOXI1 | 5q35.1 | Forkhead box protein I1 |
| WDR72 | 15q21.3 | WD repeat-containing protein 72 |
| ATP6V1C2 | _ | V-type proton ATPase, subunit C, kidney isoform |
The most prevalent forms of the disease are non-genetic, secondary to autoimmune diseases (including Sjögren's syndrome, systemic lupus erythematosus, rheumatoid arthritis), administration of drugs (especially cytotoxic drugs) or ingestion of toxins.2 It is estimated that secondary forms could be around four times more common than genetic forms, although this assumption has not been corroborated, and they will generally be diagnosed from the second decade of life onwards.
Regardless of its origin, 25% of patients with dRTA may experience a metabolic emergency at some point in their life4, the majority caused by a hypokalaemic crisis, with the consequent onset of muscle weakness, muscle paralysis, risk of respiratory distress, shock, coma and death. Patient series have been published with a mortality rate of 11% attributed to this cause.5
Poorly-corrected metabolic acidosis, as well as the presence of hypokalaemia, hypercalciuria, and hypocitraturia, are risk factors for associated kidney diseases: nephrocalcinosis (88-94% of patients)6,7; renal lithiasis (12–24%)7,8; chronic kidney disease, since 82% of patients between the ages of 20 and 60 years will have stage 2 or higher chronic kidney disease (CKD)7; and chronic kidney disease stage 5, reported in 2.1–5% of patients.9,10 Metabolic acidosis will be responsible for associated bone disease in these patients: osteoporosis, reported in 43% of children and 90% of adults9,11; osteomalacia, reported in 9.6% to 23.3% of adult patients12,13; bone deformities, reported in 25% of children11; pathological fractures reported in 6.3% of these patients9 and growth retardation and short stature in 50% to 79.1% of children.6Fig. 1 illustrates how metabolic acidosis, hypercalciuria, hypocitraturia, and hypokalaemia will condition the progression of the clinical manifestations of dRTA.

Additionally, in primary forms, sensorineural hearing loss has been reported in up to 92% of patients with the ATP6V1B1mutation.6 It has not been definitively established whether there could be some type of associated hearing loss in the secondary forms of the disease, although it is believed that this should not be the case, since the reason for hearing loss seems to be the alteration of the proton pump dependent on an ATPase located in the inner ear.
A direct relationship has been established between adequate metabolic control of the disease and better bone health and better preservation of kidney function.7,9
As we have already mentioned, dRTA is a rare entity and the primary forms are mostly diagnosed by paediatric nephrologists. However, the diagnosis is sometimes made by adult nephrologists in patients with recurrent lithiasis, especially if the kidney stones are fully or partially composed of calcium phosphate (CaP), the urine has a persistent pH>5.5 and they present with hypocitraturia. In many cases, blood bicarbonate levels are normal, which explains why these entities were not diagnosed in childhood. This is an attenuated form of dRTA called incomplete dRTA. However, for a definitive diagnosis, unlike complete dRTA, it is mandatory to perform urinary acidification tests (urinary acidification tests with ammonium chloride, urinary acidification test with furosemide or furosemide-fludrocortisone, determination of maximum urinary pCO2, stimulation with sodium bicarbonate and/or acetazolamide). It is important to note that urinary acidification capacity is not a dichotomous trait but rather a continuous one, which means that incomplete dRTA is not a distinct entity, but can be one end of a spectrum. Recent findings suggest that incomplete dRTA may be attributed to heterozygous carriers of hypofunctional V-ATPase. Treatment also consists of receiving alkaline therapy, preferably in the form of potassium citrate, administered prudently so as to treat chronic acid retention that favours both stone formation and bone disease but without excessively raising the urine pH level, which would further promote the formation of CaP in urine.14
In light of the reasonable doubts about the established follow-up of these patients in adulthood, a group of experts designed a brief survey, distributed to a cohort of Spanish nephrologists, to assess epidemiological, diagnostic and clinical and therapeutic follow-up aspects of dRTA.
Material and methodsIn January 2019, a group of five experts interested in dRTA, made up of three paediatric nephrologists and two adult nephrologists, developed a questionnaire with 10 multiple-choice questions that aimed to evaluate epidemiological aspects (number of patients seen in consultations in the last year and last three years), diagnostic aspects (conducting a confirmatory genetic test of the disease and drawing up a genealogical tree), clinical follow-up aspects (age of transfer of these patients to the hospital nephrology department, frequency of follow-up of these patients) and therapeutic management aspects (assessment of bicarbonataemia and calciuria control, degree of treatment compliance, drugs used and their dosage).
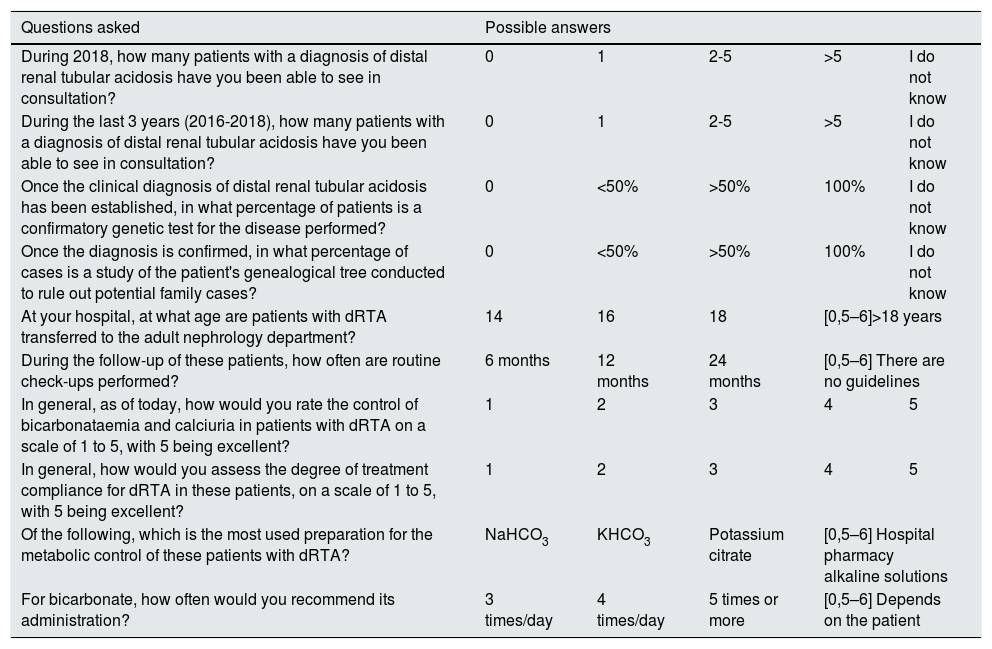
The complete survey is shown in Table 2. This survey was distributed on paper to those attending a forum on dRTA during the last congress of the Spanish Society of Nephrology [Sociedad Española de Nefrología (SEN)] held in October 2019. The SEN was informed in advance of the intention to conduct this project. For greater flexibility in obtaining the results of this survey, and given the degree of saturation to which clinical nephrologists are subjected regarding this type of exercise using online surveys, it was decided to opt for a more pragmatic and streamlined approach. The results were analysed using simple parametric statistical tests, expressing the answers in the analysis in percentage terms compared to the total number of surveys received. For questions which not all respondents answered, the total number of surveys received was also considered to be 100%.
Questions included in the survey with their possible answers.
| Questions asked | Possible answers | ||||
|---|---|---|---|---|---|
| During 2018, how many patients with a diagnosis of distal renal tubular acidosis have you been able to see in consultation? | 0 | 1 | 2-5 | >5 | I do not know |
| During the last 3 years (2016-2018), how many patients with a diagnosis of distal renal tubular acidosis have you been able to see in consultation? | 0 | 1 | 2-5 | >5 | I do not know |
| Once the clinical diagnosis of distal renal tubular acidosis has been established, in what percentage of patients is a confirmatory genetic test for the disease performed? | 0 | <50% | >50% | 100% | I do not know |
| Once the diagnosis is confirmed, in what percentage of cases is a study of the patient's genealogical tree conducted to rule out potential family cases? | 0 | <50% | >50% | 100% | I do not know |
| At your hospital, at what age are patients with dRTA transferred to the adult nephrology department? | 14 | 16 | 18 | [0,5–6]>18 years | |
| During the follow-up of these patients, how often are routine check-ups performed? | 6 months | 12 months | 24 months | [0,5–6] There are no guidelines | |
| In general, as of today, how would you rate the control of bicarbonataemia and calciuria in patients with dRTA on a scale of 1 to 5, with 5 being excellent? | 1 | 2 | 3 | 4 | 5 |
| In general, how would you assess the degree of treatment compliance for dRTA in these patients, on a scale of 1 to 5, with 5 being excellent? | 1 | 2 | 3 | 4 | 5 |
| Of the following, which is the most used preparation for the metabolic control of these patients with dRTA? | NaHCO3 | KHCO3 | Potassium citrate | [0,5–6] Hospital pharmacy alkaline solutions | |
| For bicarbonate, how often would you recommend its administration? | 3 times/day | 4 times/day | 5 times or more | [0,5–6] Depends on the patient | |
dRTA: distal renal tubular acidosis.
In total, 83 surveys were handed out, one for each of the dRTA forum attendees. 45 partially or fully completed copies were collected: 40 of them contained all 10 questions answered. 44.4% reported that they had not treated any patient with dRTA during the last year and 37.7% had not done so in the previous three years. However, 17.7% were able to see one patient, and 33.3% were able to see between two and five patients during the last year. Regarding genetic aspects, 28.8% stated that confirmatory genetic diagnosis is not performed in their hospital, while 20% were not sure. In contrast, only 13.3% affirmed that a confirmatory genetic diagnosis is performed in all patients with clinical suspicion of dRTA. No type of family study is performed according to 31% of those surveyed, and 17.7% stated that they were not sure. Only 11.1% stated that a family study is always carried out in their hospital when a new patient is diagnosed.
Patients are transferred to the adult nephrology department at the age of 14 years according to 20% of those surveyed, and another 20% report that they are transferred at age 16, while the rest are transferred at 18 years of age. Follow-up of these patients is most typically carried out every six months or less, with 68.8% of the respondents agreeing on this point. 13.3% stated that the follow-up is annual, and 11.1% maintained that there are no established reviews for these patients.
Those that participated in the survey were asked to assess the metabolic control of these patients, expressed through the two parameters that have best demonstrated their correlation with the long-term clinical sequelae of the disease, bicarbonataemia and calciuria. Only 6.6% rated it as excellent, and 20% as good or very good. 44.4% stated that it was acceptable, and the rest rated it as bad or very bad.
Their opinion was also requested on the degree of treatment compliance with acidosis medication in these patients. Only 4.4% rated treatment compliance as excellent, 26.6% as good or very good, while the rest (69%) assessed treatment compliance as fair, poor or very poor.
Sodium bicarbonate and potassium citrate are the two most used treatments, as attested to by 37.7% of those surveyed for both active substances. 40% of respondents stated that the prescribed treatment is to be taken three times a day, 17.7% four times a day and 8.8% five times or more. 17.7% stated that the dosage will depend on the type of patient, without having a preconceived dosage.
DiscussionThe dRTA is a rare disease with a poor clinical outcome if metabolic control is inadequate. Given its low prevalence, the follow-up of these patients, particularly adults, is not as exhaustive as it should be. The need for appropriate transfer from the paediatric nephrology department to the adult nephrology department must be emphasised, seeking a follow-up schedule that allows for periodic evaluation of kidney function. In addition, it is essential to pay adequate attention to the treatment, which must be maintained for life and, therefore, must have the simplest dosage regimen possible, as well as a very good safety profile to facilitate its chronic administration. Treatment is imposed as mandatory to avoid the long-term consequences of the disease, such as loss of kidney function. In this regard, a recent cross-sectional study on 340 patients from 29 countries found that only 18% of these patients between 20 and 60 years of age had normal renal function.7 In patients between two and eighteen years of age, kidney function was normal in 65.3%. Furthermore, the bone involvement that accompanies poorly controlled metabolic acidosis translates into an increase in osteoporosis, osteomalacia and pathological fractures. Kidney stones have been reported in 12% to 24% of these patients, which, compared to the prevalence of lithiasis in Europe (5% to 9%)15, means dRTA might increase the risk of kidney stones up to fivefold. Moreover, it has been published that life-threatening episodes of hypokalaemia can occur in 25% of patients. Because of all these clinical sequelae, we believe that it is important to assess the degree of familiarity with this rare disease among Spanish nephrologists, exploring epidemiological, diagnostic, patient management and therapeutic aspects.
A 54% of the nephrologists who received the survey returned it completed, and the vast majority answered all the questions, although five of the 45 surveys did not fully answer all the questions. This can perhaps be explained by the fact that the respondents were not particularly familiar with this rare disease at the time of completing the survey. In our experience, the fact that more than half of those attending a scientific forum participated in this exercise exceeds all expectations, since the use of other channels that are more in line with current technology (e-mails, website links or survey monkey-like tools) yields a percentage of spontaneous participants that barely exceeds 20%.
The fact that they voluntarily attended a training session on dRTA can be interpreted that the attendees also had a priori a greater interest in this disease compared to the nephrologist community as a whole, which may also explain the high percentage of responses obtained. This circumstance must be taken into account when analysing the responses, since there may be a bias in the sample population compared to the nephrologist community as a whole. As such, given that 44.4% and 37.7% of those surveyed had not seen a single patient with dRTA in the previous year and the previous three, respectively, it is logical to assume that this percentage, along with the low level of familiarity with the disease, would be even greater among nephrologists as a whole.
It is striking that only 13.3% of those surveyed stated that a genetic confirmation of the result is performed in 100% of newly diagnosed cases. 20% of the sample stated that they did not know the percentage of genetic confirmations performed in their hospital. Similarly, a family study is only conducted in 11.1% of the surveyed hospitals. These figures should make us reflect on the need for a greater focus on renal tubular disorders and specifically dRTA, since, compared to other genetic diseases with kidney involvement, the percentage of cases where there is genetic confirmation and a family study is extremely low. The actual figure could be even lower due to the sample selection bias already discussed.
The age at which paediatric patients are referred to the adult nephrology department is usually 18 years. At least 51% of paediatric patients are transferred to adult nephrology at 18 years of age or older. In chronic multisystemic diseases, transfers from paediatric departments tend to be delayed, while for more trivial or milder conditions they are either not transferred to an adult department or they are transferred at an earlier age. According to 68.8% of the respondents, these patients are most commonly followed up every six months or less. To date, there are no guidelines or recommendations that address how often these patients should be assessed, meaning that no type of assessment or comparison can be established.
Only 26.6% of those surveyed stated that the metabolic control of these patients is excellent or good or very good, revealing an urgent need to improve metabolic control. In a cross-sectional study of 340 patients, only 51% of them had adequate metabolic control, understood as adequate bicarbonataemia and calciuria.
Only 4.4% believed that treatment compliance is excellent and 26.6% good or very good. In the opinion of those surveyed, adherence to treatment is fair, poor or very poor in 69% of patients. The figure for adequate treatment compliance (31%) may be overestimated, meaning that the actual figure may be much lower. In any case, adherence to treatment in this disease is far below the estimated 50% adherence reported in other chronic conditions.16
Regarding the most commonly used treatment, sodium bicarbonate and potassium citrate are the two most used agents: 37.7% each according to the respondents. These drugs are prescribed to be taken three times a day according to 40% of those surveyed. 17.7% recommend an administration of four times a day and 8.8% recommend five times a day. This variable posology throughout the day, together with the fact that it is a chronic disease, are two circumstances that lead to poor treatment compliance, which will lead to further deterioration of kidney function and bone disease. This reality should undoubtedly motivate us to pay more active attention as to whether or not these patients have adequate metabolic control.
ConclusionsPrimary dRTA is a rare disease with significant clinical sequelae. In Spain, the low percentage of confirmatory genetic diagnosis and the small number of family genealogical studies conducted is surprising. The manifestly low degree of metabolic control, together with poor treatment compliance, should alert us to the potential risk of chronic kidney disease progression and the clinical sequelae of bone disease. As a result, actions are necessary that provide greater awareness of the disease in the Spanish nephrological community, as well as future treatment alternatives that improve its metabolic control, in terms of efficacy, tolerability and treatment compliance.
Conflicts of interestVíctor M. Navas is a consultant for Advicenne Pharma Iberia. The other authors have no conflicts of interest to declare.
Please cite this article as: Torregrosa Prats JV, Rodríguez FS, Parra EG, Román LE, Buades Fuster JM, Monteagud-Marrahí E, et al. Acidosis tubular renal distal (ATRd): aspectos epidemiológicos, diagnósticos, de seguimiento clínico y terapéuticos. Resultados de una encuesta a un colectivo de nefrólogos. Nefrologia. 2021;41:62–68.



