







Instrumental Activities of Daily Life (IADL) requires a higher level of personal autonomy and interaction with the environment than the basic activities of daily life (BADL). Few studies analyze the deficit on IADL. Early detection is important because an early action can delay the evolution of the dependency process.
AimTo know the prevalence of functional deficit in IADL of hemodialysis patients, its relationship with the functional deficit in the BADL and its influence on the health related quality of life (HRQoL).
MethodsCross-sectional study in 66 patients on HD. Different scales were used: Lawton and Brody (AIVD dependency), Delta (BADL dependency), and Coop-Wonca (HRQOL). Clinical data were collected (age, sex, CKD etiology, months in HD, marital status, employment situation).
Results80.3% of the patients had some degree of dependence for the IADL (57.5% in moderate / severe degree) and 40.8% for the BADL (9% in moderate / severe degree). There was a correlation between dependence to the BADL and AIVD. Age and employment status influence the dependence on IADL and BADL. Patients with greater dependence on IADL had worse HRQoL (p < 0.000). The dimensions in which they showed greater differences were "Daily activities", "Social activities" and "Social support".
ConclusionsHD patients are more dependent on IADL than on ADL and with a higher degree of severity and the level of dependence in both types of activities has important influence on HRQoL. Early detection of the occurrence of disability in the realization of IADL can be used to initiate intervention programs that help to prevent, reverse or delay the progression.
Las actividades instrumentales de la vida diaria (AIVD) requieren un mayor nivel de autonomía personal e interacción con el entorno que las actividades básicas de la vida diaria (ABVD). Pocos estudios analizan el déficit funcional en AIVD. La detección temprana del déficit es importante, pues una acción temprana puede retrasar la evolución del proceso de dependencia. El objetivo de este estudio fue conocer la prevalencia de déficit funcional en AIVD de pacientes en hemodiálisis, su relación con el déficit funcional en la ABVD y su influencia en la calidad de vida relacionada con la salud (CVRS).
MétodosEstudio transversal en 66 pacientes en HD. Se utilizaron diferentes escalas: Lawton y Brody (dependencia AIVD), Delta (dependencia ABVD), y Coop-Wonca (CVRS). Se recogieron datos clínicos (edad, sexo, etiología de la ERC, meses en HD, estado civil, situación laboral).
ResultadosEl 80,3% de los pacientes estudiados tenían algún grado de dependencia para el AIVD (57.5% en grado moderado / severo) y 40.8% para el ABVD (9% en grado moderado / severo). Ambos tipos de dependencia mostraron correlación (R: - 0.583, p: 0.000). La edad y la situación laboral influyen en la dependencia de las AIVD y las ABVD. Los pacientes con mayor dependencia de la AIVD tuvieron una peor CVRS (p < 0.000) con mayores diferencias en las dimensiones: "Actividades diarias", "Actividades sociales" y "Apoyo social".
ConclusionesLos pacientes de HD presentan más dependencia a las AIVD que a las ABVD y con mayor severidad y ambos tipos de dependencia influye sobre la CVRS. Detectar precozmente la discapacidad en las AIVD puede servir para iniciar programas de intervención y prevenir, revertir o retrasar la progresión.
The characteristics of the hemodialysis population has changed with respect to two decades ago. With the aging of the population and the technical aspects of renal replacement therapy, dialysis facilities face, the challenge of caring for patients with a progressive increase in the degree of functional dependence.1
This has implications for the structure, organization and operation of the dialysis units.2,3 Also there is an impact on patients, being a risk factor for mortality4–6 and influence decisively on issues such as interaction with the environment and the health-related quality of life (HRQL).7
Most of the studies that analyze the level of dependence of dialysis patients have focused on the basic activities of daily living (BADL),2,8–10 and only analyze the functional deficit in instrumental activities of daily life (IADL). The latter are more complex activities, with a greater requirement of personal autonomy and interaction with the environment. Deficits in IADL are observed earlier than the deficits in the BADL.4,5,9,11 The IADL include activities such as: the use the telephone, preparation of food, basic household chores (washing dishes, beds …), shopping, laundry, use of medication, use of transport and use of money.
The disability in the IADL could precede the appearance of a more important functional deficit affecting the BADL. It has been proposed that an early action aimed at helping the patient to improve their autonomy may delay the progression of the dependency.12
The objective of this study has been to determine in hemodialysis patients the prevalence of functional deficit in IADL, its relationship with functional deficit in BADL and the influence on health-related quality of life (HRQL).
MethodsPatientsCross-sectional study in 97 hemodialysis patients from a single hospital that receives patients with high complexity. The study included the 66 patients (68%) that agreed to be assessed by the occupational therapists with all available tests and that were able to understand the questions. Thirty-one patients were excluded (32%) from the study (3 blindness, 4 deafness, 5 dementia, 10 refused to participate in the study and 9 were not clinically stable due to acute concomitant diseases, recent admissions, active cancer or hepatic cirrhosis…). There were no significant differences between patients included and excluded in age (66.3 ± 12.9 vs. 67.2 ± 13.1 years; p = NS), months on hemodialysis (114 ± 119.3 vs. 112 ± 114.5; p = NS) or gender distribution (71.2% vs. 67.7% male).
Data collection procedureAll participants were informed of the nature and objectives of the study and signed the informed consent. All scales were completed during one of the hemodialysis (HD) sessions, while the patient was in a stable clinical situation, and were administered by experts occupational therapists. Other variables such as age (years), sex, etiology of CKD and time on hemodialysis (months), marital status, employment status were obtained from the patients' medical records. The collection of these data was performed over a period of one month.
Measuring instrumentsThe scales Lawton and Brody were used to measure dependence on IADL; the dependence on BADL was assessed with the Delta test and COOP-WONCA sheets were used to measure HRQL.
Dependence on instrumental daily life activity: Lawton and Brody scaleThe Lawton and Brody13 scale explores independence in the use of telephone, shopping activity, food preparation, cleaning, washing, travel, taking medication and managing finances. It assigns a value of 1 (independent) or 0 (dependent). The final score is the sum of the values of all answers. It ranges from 0 (maximum dependence) to8 (total independence). This information is obtained by directly asking the individual or their primary caregiver.
Dependence on the basic activities of daily life: Delta testThe "Delta test"14 has been used as a method of assessing the level of dependency on BADL in hemodialysis patients.2 A person is considered to be "valid" if according to the "Delta test" is "valid or requires only a mild assistance", and it is considered "assisted person" if the results of the test indicates that such a patient is "moderate assisted or decidedly assisted". The Delta test is a scale consisting of 3 independent subscales, whose different items score from 0 to 3 (from least affected to most severe): 1) degree of dependence, as an indication of the need for care of the person (0: autonomy of function, 1: occasional help, 2: frequent help and 3: permanent help); 2) physical deficiency; and 3) psychic deficiency. The total scores are obtained by adding the corresponding values to each item, obtaining 3 different values that correspond to: dependence (maximum score 30), physical deficiency (maximum score 15) and psychic deficiency (maximum score 15). Higher score means higher dependence. Assessing the score corresponding to the dependency questionnaire the following classification is made: valid from 0 to 1 point, mild assisted from 2 to 9 points, moderate assisted from 10 to 19 points, to markedly assisted from 20 to 30 points.
Health-related quality of life: COOP-WONCA sheetsHRQL has been estimated using the Spanish version of COOP-WONCA sheets.15,16 The choice of these sheets instead of other questionnaires, such as the Nottingham Health Profile, Sickness Impact Profile, Kidney Disease Quality of Life or SF-36 has been based on the fact that, having similar validity, they are easier to answer and have been used previously in dialysis patients.17,18 There are 9 sheets and each of them explores an aspect of the patient's quality of life in a global manner. Each aspect has a title and answers the question in relation to what happened in the last 2 weeks: 1) physical form; 2) feelings; 3) daily activities; 4 ) social activity; 5) change of health status; 6) health status; 7) pain; 8) social support; and 9) quality of life in general. The possible answers follow an ordinal scale from 1 to 5, and higher scores indicates worse HRQoL.
Statistical analysisThe statistical analysis was performed using the SPSS 12.1 program. The Student's "t" test has been used for comparison of independent samples if the data followed a normal distribution, and the Wilcoxon test in cases where the samples did not follow a normal distribution. Qualitative variables were compared using the Chi-square test and the magnitude of the association has been quantified by the odds ratio with the 95% confidence interval. The magnitude of the correlation between the results obtained through the different scales was evaluated by Pearson's linear correlation coefficient. The level of statistical significance was defined as p < 0.05.
ResultsThe demographics of the patient population are shown in Table 1.
Sample description.
| Average (SD) | ||
|---|---|---|
| Age (years) | 66.3 (12.9) | |
| Time in HD (months) | 114 (119.3) | |
| N | % | |
| Gender | ||
| Men | 47 | 71.2 |
| Women | 19 | 28.8 |
| Marital status | ||
| Single | 3 | 4,5 |
| Married | 44 | 66.7 |
| Divorced | 6 | 9.1 |
| Widower | 13 | 19.1 |
| Employment status | ||
| Employment status | 32 | 48.5 |
| Employment status | 29 | 43.9 |
| Employment status | 5 | 7.6 |
| Etiology of CKD | ||
| Unknown | 14 | 21.2 |
| PKD | 8 | 12.1 |
| Diabetes | fifteen | 22.7 |
| Glomerular | 8 | 12.1 |
| Vascular | 7 | 10.6 |
| Interstitial | 8 | 12.1 |
| Other | 6 | 9.1 |
Eighty point three percent of the patients studied had some degree of dependence for IADL (57.5% in moderate/severe degree) (Fig. 1) and 40.8% had dependence for BADL (9% in grade moderate/severe). The IADL in which the patients showed more dependence were activities related to the house (shopping, taking care of the house, cooking, washing clothes) (Fig. 2). There was a correlation between the dependence on the BADL (the higher score the greater the dependence) at the global level (R: –0.583; p = 0.000); physical (R: –0.389; p = 0.001) and psychological (R: –0.271; p = 0.028) and the AIVD (lower score the means greater dependence) (Table 2).
.")
.")
Comparative cross table between BADL and IADL for the cut-off points (X 2 20.7; p < 0.002).
| BADL | IADL | |||
|---|---|---|---|---|
| Independent (0–1 points) | Mild-Moderate Dependent (2–6 points) | Dependent severe (7–8) | Total | |
| Valid (0–1 points) | 20 | 20 | 2 | 42 |
| Slight Assisted (2–9 points) | 3 | 13 | 2 | 18 |
| Moderate Assisted (10–19 points) | 0 | 3 | 2 | 5 |
| Severe dependent (20–30 points) | 0 | 0 | 1 | 1 |
| Total | 23 | 36 | 7 | 66 |
The time on HD, gender, the etiology of CKD and marital status do not influence the performance of the IADL or the dependence on the BADL, however age and employment status had an effect on IADL and BADL (Table 3). There were no gender differences in the dependence of the different activities except laundry (X2 : 9.4; p = 0.003) where men were more dependent.
Factors related to functional deficit for BADL and IADL.
| ABVD | p | AIVD | p | ||||
|---|---|---|---|---|---|---|---|
| Valid | Slight Assisted | Moderate Severe Assisted | Independent mild Dependent | Dependent moderate severe | |||
| Age (years) | 63.6 (12.6) | 68.3 (12.3) | 77.3 (10.8) | 0.034 | 57.2 (9.1) | 72.6 (11.2) | 0.000 |
| Months on HD | 112.4 (122.7) | 106.7 (93.4) | 164.8 (187.6) | 0.621 | 141.5 (141.5) | 95.2 (97.3) | 0.136 |
| Gender (%) | 0.584 | 0.557 | |||||
| Males(n: 47) | 55.3 | 34 | 10.6 | 40.4 | 59.6 | ||
| Females (n: 19) | 68.4 | 26.3 | 5.3 | 42.1 | 57.9 | ||
| Marital status (%) | 0.992 | 0.673 | |||||
| Married (n: 44) | 59.1 | 31.8 | 9.1 | 40.9 | 59.1 | ||
| Single (n: 3) | 66.7 | 33.3 | 0 | 66.7 | 33.3 | ||
| Divorced (n: 6) | 50 | 33.3 | 16.7 | 50 | 50 | ||
| Widower (n: 13) | 61.5 | 30.8 | 7.7 | 30.8 | 69.2 | ||
| Employment status | 0.003 | 0.000 | |||||
| Active (n: 32) | 75 | 21.9 | 3.1 | 53.1 | 46.9 | ||
| Unemployed (n: 5) | 80 | 20 | 0 | 100 | 0 | ||
| Retired (n: 29) | 59.1 | 31.8 | 9.1 | 17.2 | 82.8 | ||
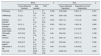
Patients with greater dependence on IADL showed worse perception of health status HRQoL (moderate-severe dependent: 23.8 [6.5], independent or mildly dependent: 19.2 [5.4]; p = 0.004) (Fig. 3 and Table 4). The areas "daily activities" and "social activities" were the ones that showed worse scores in moderate-severe dependent patients compared to the rest.
 charts according to the degree of dependence on the instrumental activities of daily life (Lawton and Brody scale).")
Health-related quality of life scores (HRQoL) in COOP-WONCA charts (mean [SD]) according to the degree of dependence on IADL (Lawton and Brody scale) and BADL (Delta test): means and SD.
| BADL | p | IADL | p | ||||
|---|---|---|---|---|---|---|---|
| Severe Moderate Assisted | Mild assisted | Valid | Severe Moderate Dependent | Dependent and mild independent | |||
| CW fitness | 5 (0.1) | 4 (1.0) | 3.7 (1.0) | 0.042 | 4.23 (0.86) | 3.59 (1.1) | 0.001 |
| CWfeelings | 3 (1,2) | 1.9 (1.1) | 1.9 (1.1) | 0.06 | 2.38 (1.30) | 1.62 (0.9) | 0.003 |
| CW daily activities | 4 (1) | 3.1 (1.4) | 1.9 (0.8) | 0.001 | 3.05 (1.4) | 1.74 (1.2) | 0.000 |
| CW social activities | 3.6 (1.1) | 3.7 (1.0) | 2.1 (0.7) | 0.001 | 3.35 (1.4) | 1.88 (1.4) | 0.000 |
| CW change health status | 3.33 (0.8) | 3.7 (0.7) | 2.7 (1.1) | 0.12 | 2.87 (0.6) | 2.77 (0.9) | 0.405 |
| CW health status | 3.67 (0.5) | 3.6 (1.0) | 2.5 (1.1) | 0.46 | 3.54 (0.9) | 3.14 (1.1) | 0.128 |
| CW pain | 3.17 (1.6) | 2 (1,3) | 2.2 (1.0) | 0.12 | 2.55 (1.3) | 2.05 (1.4) | 0.166 |
| CW social support | 2.83 (0.7) | 3.4 (1.0) | 2.3 (1.1) | 0.001 | 3.03 (0.8) | 2.33 (1.1) | 0.006 |
| CW quality of life | 3.17 (0.7) | 2.73 (0.7) | 2.4 (0.7) | 0.06 | 2.71 (0.8) | 2.44 (0.6) | 0.127 |
| Total CW | 27.8 ( 2.9) | 24.62 (5.8) | 19.3 (5.2) | 0.01 | 24.62 (5.2) | 19.21 (5.3) | 0.000 |
Significance value of p for ABVD comparative between valid and moderate-severe assisted.
The patients with a greater degree of dependence on the BADL (Fig. 4 and Table 4) had significantly higher scores on the COOP-WONCA sheets than the valid patients, equivalent to a worse perception of their HRQL. The areas in which they showed the greatest differences were "daily activities", " social activities" and "social support".
Discussion according to the degree of dependence on basic activities of daily living (Delta test).")
The results of the present study indicate that disability in the activities required for independent living (BADL and IADL) is a highly prevalent condition in patients on hemodialysis and is associated with a reduced HRQL.
In the present study 40.8% of patients had some degree of dependence for the BADL (9% in a severe degree), a similar result to that obtained in a multicenter study conducted in our community in a larger group of patients.2 The dependence on IADL showed a higher prevalence (80%), and more than half were moderate-severe. Functional dependence for IADL has not been sufficiently evaluated in hemodialysis patients, and the few publication that have included this parameter estimate global prevalence between 19% and 59%,4,6,9,11 which is lower than reported by this study. This prevalence vary depending on the parameter analyzed and the countries, as demonstrated in the DOPPS6 study, in which the prevalence of dependent patients for some IADL in the United Kingdom was 81% and in Spain it was 62%. In our study the prevalence is higher than other studies, which may be due to several factors: 1) the specific characteristics of the population in our unit as it is a single center of a specific geographical area; 2) the collection of information was not obtained by the unit staff (nurses, nephrologists …), but by experienced personnel (occupational therapists), with greater knowledge in the area and with the ability to identify this type of deficiencies; or 3) high number, about a third, of patients were excluded, because the high complexity and time invested in completing the questionnaires, which also implies a limitation of this study when determining prevalence, since a high number of patients could not be studied.
Dependency is part of a process that begins with the initiation of a deficit in body function that, if not corrected adequately and on time, ends up in a limitation for the individual who needs the help of other people to carry out the everyday life activities. The IADL present greater complexity than BADL and require more personal autonomy and interaction with the environment, which justify its earlier appearance and the higher prevalence and severity found in our study. The detection of functional deficits in IADL with an impact on medical hygiene, nutrition, economic activity or taking medication may be important in the overall assessment for inclusion in the waiting list for renal transplantation, especially in those patients who do not have family support, and the lack of personal autonomy in these areas could even affect the viability of the graft if preventive measures are not taken.
Both types of functional dependence, IADL and BADL, showed a statistically significant association. It is possible that we are facing different gradations of the same problem. Some studies12 show that rehabilitation through education, cognitive, physical and psychosocial may prevent, reverse or delay the progression of functional impairment of IADL to BADL, so early detection of the deficit is important and its evaluation should be incorporated into the routine of standard dialysis care.
The IADL in which the patients showed more dependence were those related to home care (shopping, food preparation, household chores and laundry). This affected more than 50% of the patients (Fig. 2).
In our study, only age and labor status showed significant association with functional disability for IADL (patients with a moderate / severe degree of dependence on IADL were older and a high proportion were retired). The time in HD, gender and the etiology of CKD was not significantly associated with dependence on IADL (Table 2). It was know the association between age and disability as observed in other studies that have analyzed the problem.4,6,9,11
One could speculate that the high prevalence of disability in IADL in our population could be due to the high prevalence of men (71%), however we did not observed an association between males and functional disability. In the general population, a higher incidence of disability in IADL has been described in women with chronic diseases and greater social vulnerability, which is maintained even after controlling adverse social and clinical conditions.19 In our study the only differences in dependence between males and females was in the activity of washing clothes in which men were more dependent, and this may be related to sociocultural factors.
Although dialysis has immediate benefits, it also add stress to the patient. The onset of dialysis has been associated with a significant and sustained decrease in the functional status of patients 1 and has a strong impact on HRQL.20 In hemodialysis patient over 75 of age the HRQL has been linked to factors such as gender (worse HRQL in women), depression, cognitive impairment and the level of self — sufficiency measured by the Karnofsky scale.18,21 In the present study, HRQL is also influenced by the degree of dependence, both for BADL and for IADL, so that greater dependence is associated with worse HRQoL (Figs. 3 and 4 and Table 3).
HRQL has been defined as the subjective perception, influenced by the current state of health, of the ability to perform activities important to the individual.22 It measures how the value assigned to the duration of life is modified based on the perception of limited physical, psychological, social activities and the reduction of opportunities due to the disease, its sequelae, treatment and / or health policies.23 Therefore it is not strange to observe the great impact that functional disability has on HRQL. In this study, the areas that showed the greatest differences between dependent and non-dependent patients were "daily activities","social activities" and "social support."
The strategies to cope with the various situations and social support are aspects of maximum importance and with significant influence in the evaluation of HRQL. There is numerous evidence showing that, as the disease progresses, internal adjustments occur that preserve the person's satisfaction with life, so there are people with significant degrees of physical limitation who consider that their quality of life to be good.24
From the clinical point of view it is then possible to improve the process of adaptation to the disease, teaching strategies to handle the disease. Occupational therapists may help to plan and reinvent structures for life that were lost due to illness, disability or pain. It is important to provide the patient with the necessary tools so that with a new behavior and attitude they can restructure and regain control over their life and restore hope, competence, confidence and success as part of daily activities.25 Occupational therapy has been widely applied as a complementary intervention in different areas of medicine, especially in chronic diseases such as mental illnesses and neurological disorders. However, there is very little research aimed at assessing its effectiveness in dialysis patients. Some studies show a positive impact of occupational therapy programs on HRQL in dialysis patients, especially in the control of pain.26 The longer term benefits should be investigated in large number of patients.
The limitations of the study include the small number of patients evaluated. The study did not include all patients of our dialysis unit. It was a cross-sectional design and in a single center. But, we consider that these limitation are somewhat compensated by the strength of being the first study in our country studying the dependence on IADL in hemodialysis patients and the fact that the tests have been performed by occupational therapists skilled in the field. Also, our study was performed using the Lawton and Brody scale, which is widely used and it had to be validated for this purpose; though this scale is based on patient responses and not on objective tests and, the items measured may have cultural, environmental or gender influences that may affect the result.
In conclusion, hemodialysis patients have more dependence and with a greater degree of severity to the IADL than to BADL. The level of dependence in both types of activities has an important influence on HRQOL. Early detection of disability to perform IADL should be followed by implementation of programs that help to prevent, reverse or delay the progression of such functional impairment. This strategy may avoid that other spheres of the individual's life became affected.
Conflict of interestsThe authors declare that they have no conflicts of interest for this article.
ThanksOur thanks to all the patients who have collaborated in the study.
Please cite this article as: Arenas MD, Navarro M; Serrano E, Alvarez-Ude F. Dependencia para las actividades instrumentales de la vida diaria en pacientes en hemodiálisis: influencia sobre la calidad de vida relacionada con la salud. Nefrologia. 2019;39:531–538.



