


A multidisciplinary approach and Doppler ultrasound (DU) assessment for the creation and maintenance of arteriovenous fistulas (AVF) for haemodialysis can improve prevalence and patency. The aim of this study was to analyze the impact of a new multidisciplinary vascular access (VA) clinic with routine DU.
Material and methodsWe analyzed the VA clinic results from 2014 and 2015, before and after the implementation of a multidisciplinary team protocol (vascular surgeon/nephrologist) with routine DU in preoperative mapping and prevalent AVF.
ResultsWe analyzed 345 and 364 patients from 2014 and 2015 respectively. The number of surgical interventions was similar in both periods (p=.289), with a trend toward an increase in preventive surgical repair of AVF in 2015 (17 vs. 29, p=.098). 155 vs. 169 new AVF were performed in 2014 and 2015, with a significantly lower primary failure rate in 2015 (26.4 vs. 15.3%, p=.015), and a non-significant increase in radiocephalic AVF, 25.8 vs. 33.2% (n=40 vs. 56), p=.159. The concordance between the indication at the clinic and the surgery performed also increased (81.3 vs. 93.5%, p=.001). Throughout 2015 fewer complementary imaging test were requested from the clinic (78 vs. 35, p<.001), with a corresponding reduction in costs (€ 87,716 vs. € 59,445).
ConclusionsMultidisciplinary approach with routine DU can improve VA results, with a decrease in primary failure rate, higher likelihood of radiocephalic AVF, better management of dis-functioning AVF and lower radiological test costs.
El abordaje multidisciplinar y el uso de ecografía doppler (ED) en la creación y vigilancia del acceso vascular (AV) puede mejorar la prevalencia y permeabilidad de las fístulas arteriovenosas (FAV) para hemodiálisis. El objetivo de este estudio es analizar el impacto de una nueva consulta multidisciplinar (CMD) de AV con ED de rutina.
Material y métodosEvaluamos los resultados de la consulta de AV en 2014 (pre-CMD) y 2015 (CMD), antes y después de la implantación de un equipo multidisciplinar (cirujano vascular/nefrólogo) con ED de rutina en mapeo prequirúrgico y FAV prevalente.
ResultadosSe evaluaron 345 pacientes en 2014 (pre-CMD) y 364 pacientes en 2015 (CMD). En ambos periodos se realizó un número similar de cirugías, 172 vs. 198, p=0,289, con tendencia a aumentar las cirugías preventivas de reparación de FAV en el periodo CMD, 17 vs. 29 (p=0,098). En FAV de nueva creación (155 vs. 169), disminuyó la tasa de fallo primario en el periodo CMD, 26,4 vs. 15,3%, p=0,015 y aumentó de forma no significativa la realización de FAV radiocefálicas distales, 25,8 vs. 33,2% (n=40 vs. 56), p=0,159. También aumentó la concordancia entre la indicación quirúrgica en la consulta y la cirugía realizada (81,3 vs. 93,5%, p=0,001). En el periodo CMD se solicitaron menos exploraciones radiológicas desde la consulta, 78 vs. 35 (p<0,001), con una reducción del gasto sanitario (81.716€ vs. 59.445€).
ConclusionesEl manejo multidisciplinar y la utilización del ED de rutina permiten mejorar los resultados de AV, con disminución de la tasa de fallo primario de FAV, más opciones de FAV distal nativa, mejor manejo de la FAV prevalente disfuncionante y menor coste en exploraciones radiológicas.
Autologous arteriovenous fistula (AVF) is the vascular access (VA) of choice in hemodialysis (HD) patients. As compared with central venous catheters (CVC) and prosthetic fistulas (PTFE), AVF is associated with a lower rate of infection, complications and less health cost, and it has greater long-term patency.1–3 However, in recent decades, due to the increase in age and comorbidity of HD patients, achieving a functioning and long-lasting AVF is increasingly complex.4–8 It is estimated that the rate of early primary failure of the AVF, according to the definition of the North American consortium of vascular access (NAVAC),5 is between 23 and 37% and the primary unassisted permeability at one year is between 40% and 64%.4,6,7 Between 21% and 50% of the AVFs performed never mature enough to be used in HD.4,6,7
Multidisciplinary programs for creation and follow-up of VA recommended in clinical guidelines1–3 may help to reduce the rate of primary failure and maintain the medium and long-term permeability of the AVF.8–11 The use of Doppler ultrasound (DU), both in the preoperative evaluation and in the subsequent surveillance of the AVF, has also shown important benefits in the primary, assisted and secondary survival of the AVF.12–14
Aiming to improve the results of VA in our center, we generated the multidisciplinary clinic consultation (MDC) of VA in the Hospital Gregorio Marañón at the beginning of the year 2015. Patients were conjointly evaluated by the services of Peripheral Vascular Surgery (PVS), Nephrology and we incorporated the use of routine of DU.
The objective of the present study, observational and retrospective, is to analyze the results of the VA after the first year of implementation of the MDC as compared with the previous year without MDC.
MethodsThe VA clinic of the University General Hospital Gregorio Marañón currently covers a health area of approximately 800,000 inhabitants, receiving patients from the Infanta Leonor Hospital in Madrid, the University Hospital of the Southeast and two external dialysis centers (FMC-Dialcentro and FMC-Los Junipers). Until the end of 2014 it was organized as a monographic consultation clinic of the PVS service. The surgeon based the indication of new VA or repair of AVF on the patient's medical history and physical examination of the upper extremities.
The MDC of VA was started at the beginning of 2015 and it includes the following characteristics:
- –
Joint assessment of the patient by PVS and Nephrology Service.
- –
Incorporation of a Doppler ultrasound (DU) device (Logic e-GE) for routine ultrasound examination of all patients assessed in the clinic.
- –
Generation of a group of 5 subspecialized vascular surgeons to perform, repair and creation of AVF.
- –
Intensive coordination with each of the patient referral centers, ensuring bidirectional flow of information and consensus of the actions decided.
In pre-surgical mapping performed with DU it has been considered that to indicate a radiocephalic AVF (RC), the radial artery should have a recommended minimum caliber of 1.7mm and a systolic peak velocity (SPV) greater than 35cm/s and the cephalic vein should have a caliber of at least 1.8mm. measured with a compressor.2,3,15,16 In each of the indications of AVF, it was specified the most appropriate location for the anastomosis, specifying the distance between the artery and the vein and the individual anatomical characteristics in each case (collaterals vessels, trayectory, depth, etc.).
In the assessment of prevalent AVFs, the criteria for intervention of stenosis have been based on the fulfillment of two main criteria (reduction of vessel size greater than 50% and a ratio SPV in the stenotic region/SPV pre-stenotic region>2) plus an additional finding (drop of the access flow [QA] below 500ml/min, drop of QA>25% as compared to the previous measurements in FAV with QA<1000ml/min or residual diameter <2mm). These criteria have been proposed by the Spanish multidisciplinary VA guidelines (GEMAV).3
After the first year of implementation of MDC, we retrospectively evaluated the characteristics of the patients attended, the surgical interventions performed and the results obtained in terms of the type of AVF performed and primary AVF failure. The primary failure has been defined as an AVF unable to provide adequate dialysis within three months of its creation.5
The statistical analysis was carried out using the SPSS V.21.0 computer system. The qualitative variables are expressed as a percentage and the quantitative variables as mean and standard deviation or median and interquartile range according to the characteristics of the variable. The comparison between groups was performed using the chi-square test or Fisher's test for qualitative variables and Student's t test for quantitative variables.
ResultsPatients evaluated and reasons for consultationDuring the year 2014 (pre-MDC) and 2015 (MDC) there were 345 and 364 patients evaluated in each respective year. The cause of consultation was different in each period (Figs. 1 and 2). In the MDC period, a higher percentage of patients consulted for dysfunctional AVF and to assess QA after surgery or interventional procedure, and there was a decrease in the percentage of patients coming to be evaluated after complementary tests, infection of a prosthetic fistula or for an unknown reason.
Request for complementary tests (CE) from MDC

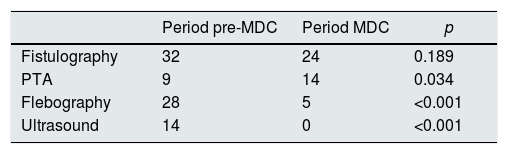
During the pre-CMD period, there were 78 complementary examinations requested (22.6% of the total number of consultations) as compared with 35 during the MDC period (9.6% of the total), p<.0.001. There were no significant differences in the number of fistulograms performed, but the percent of angioplasties was increased in the MDC period, p=0.034 (Table 1). The cost of complementary explorations requested was reduced from € 81,716 (pre-MDC) to € 59,445 (MDC).
Complementary tests requested from the vascular access clinic to the Radiology Service in both periods.
| Period pre-MDC | Period MDC | p | |
|---|---|---|---|
| Fistulography | 32 | 24 | 0.189 |
| PTA | 9 | 14 | 0.034 |
| Flebography | 28 | 5 | <0.001 |
| Ultrasound | 14 | 0 | <0.001 |
PTA: percutaneous transluminal angioplasty.
MDC: multidisciplinary clinic.
There were no significant differences in the total number of surgical interventions performed in the two periods: 172 versus 198 (p=0.289). But in relation to AVF repair surgeries, we found that during MDC period there was tendency to have a greater number of preventive surgeries aiming to repair AVF with high risk of thrombosis, 17 pre-MDC vs 29 MDC (p=0.098).
There were also differences in the period of time consumed in surgical waiting list (SWL) that was longer in the MDC period; 27 (16–41) days in the pre-MDC period as compared to 48 (27–83) days in the MDC period (p<0.001).
There were 155 new AVF performed in the pre-MDC period (25.8% RC, 58.7% autologous AVF in elbow and 15.5% prosthetic) and 169 new AVF in the MDC period (33.2% RC, 56.2% autologous FAV in elbow and 10.6% prosthetic). Therefore, in the MDC period, there was an increase in the percentage and total number of RC AVF performed (n=40 vs. 56) with a decrease in the percentage and number of prosthetic AVFs (n=24 vs. 18) However the differences did not reach statistical significance (p=0.159).
The primary failure rate of the newly created AVFs was reduced from 26.4% in the pre- MDC period to 15.3% in the MDC period (p=0.015). In the MDC period, there was an increase in the agreement between the surgery indicated from the VA consultation and the surgery actually performed, being 81.3% in the pre- MDC period compared to 93.5% in the MDC period, p=0.001.
Conservative managementThe percent of dysfunctional AVF in which a conservative management was decided, with no need for complementary examinations or not inclusion in SWL, was similar in both periods, 28.6% (n=18) pre-MDC vs. 23% (n=23) MDC, p=0.425. However, during the MDC period, the cause of the AVF dysfunction was identified in all 23 patients affected (9 non-significant stenosis, 6 thrombosed or partially thrombosed pseudoaneurysms and 8 patients with anatomical features of depth or collaterally that made punctures difficult). In all of them, a scheme was added to facilitate punctures to the nursing team of the corresponding center and the AVF with non-significant stenosis were followed quarterly with periodic evaluation of the QA. In the pre-CMD period, this was not possible because the portable DU device was not available in the consultation.
DiscussionThe creation of a multidisciplinary VA clinic with the use of Doppler ultrasound has improved the results of VA in our center, both, with a significant decrease in the rate of primary failure in the newly created AVF and in non-significant increase in the execution of distal AVFs. The management of dysfunctional prevalent AVF was improved also, with a significant increase in the number of AVF repaired endovascularly and a tendency to increase surgical repair of AVF with a high risk of thrombosis. All this was associated with a reduction of the complementary tests requested which resulted in economic savings.
Multidisciplinary VA clinics are of recent creation and the information provided in the literature still limited. In a recent survey of 47 experts from 37 European countries, only 16% of the cases had a multidisciplinary team taking care of the monitoring and evaluation of prevalent vascular access and a 62% had some form of centralization of care and planning of the VA.17
There is evidence that a multidisciplinary VA team or the figure of an VA coordinator can improve the percentage of autologous AVF performed, decreasing the number of prosthetic AVF and the prevalence of central venous catheter (CVC).18–20,11 In addition, the multidisciplinary approach to VA may improve patient satisfaction, costs and mid-term results of access functionality.21,22 However, not all studies find benefits from multidisciplinary teams. Recently, it has been published an important series of incident patients where the creation of a multidisciplinary team in the creation and surveillance of the new AVF increased the number of interventions during the first year of dialysis without achieving a decrease in CVC free time.23
The Doppler ultrasound (DU) has gained an important role in recent years. It is the first diagnostic test to be performed in case of FAV dysfunction and leaving the fistulogram relegated to those cases in which the result of DU is not conclusive.3
The use of DU in the clinic explains why there is an increase in the number of patients with the diagnosis of dysfunctional AVF. The information obtained with the DU has allowed to select more effectively those patients who needed percutaneous transluminal angioplasty or surgical repair to avoid thrombosis; also, it has allowed to elucidate the cause of the dysfunction in those AVF without significant stenosis, and some of the problems with the AVF have been solved easily by modifying the puncture sites or providing information on the depth of the vein or the presence and characteristics of collateral veins.
The DU has allowed the periodic monitoring of the QA in AVF with stenosis without criteria for intervention and AVF repaired surgically or endovascularly, since it is known that the periodic measurement of the QA may improve the secondary survival of the AVF and reduce the risk of thrombosis.13,14
The DU has also managed to minimize the need for additional test, limiting them to those patients in whom the DU was inconclusive, such as a suspicion of central stenosis, or to patients in whom a stenosis was detected with criteria of intervention. In experienced hands, DU has an excellent correlation with fistulogram and allows to provide very useful information on the location and characteristics of the stenosis, facilitating the work by the interventional radiology team.24
Regarding newly created AVFs, systematic mapping by DU is now recommended in all patients.3,12 Still there is no consensus about the minimum sizes of artery and vein to establish the indication of a distal AVF with guarantees; certainly, there are numerous factors that influence the risk of primary failure.2,3,15,25 Therefore, the main risk of increasing the percentage of RC AVF with limited vessel diameter is to increase the risk of primary failure, especially taking into account the advanced age, the suboptimal vascular bed and the important comorbidity of our incident and prevalent hemodialysis patients.5 However, thanks, to a large extent, to the information provided by the UD and the PVS team subspecialized in the creation of AVF, we have managed to reduce the primary failure rate and at the same time perform more distal FAVs, with a percentage of primary failure lower than most published series.4,6,7 The DU has been fundamental, not only to obtain information about the artery and vein sizes, the calcification and SPV of the artery, but also to define the exact location of the most favorable anastomosis, with the distance between the artery and the vein, the presence of collaterals or areas where the vein is less compressible, informing the surgeon about possible problems that may be encountered during the intervention. All this has allowed to drastically reduce the cases of discordance between the indicated AVF and the AVF performed.
The number of consultations due to prosthetic fistula infection decreased in the MDC period, probably due to the lower number of prostheses performed and the subspecialization of the surgical team. The specialization and experience of the surgical team has been shown to be one of the key factors to reduce the primary failure rate and decrease the number of surgical complications.15
Thanks to the intensive coordination between centers, decisions could be agreed upon with the nephrologists responsible for each patient. The number of patients who attended the clinic for an unknown reason was minimized. In addition, although it is difficult to quantify, the constant communication between PVS and nephrology has allowed the integration of clinical and surgical information, in such a way that the decisions made in the MDC (patient candidate or not to AVF, most adequate AVF in each patient, priority of each case in the SWL, etc.), have been carried out after agreement upon the specific case.
Among the limitations of this study it should be noted that this is a single center experience and the data collection has been retrospective.
Based on our experience, we can conclude that the multidisciplinary approach in the consultation of VA with routine DU involves important benefits for the patient with lower risk of primary failure of newly created AVF, more options for performing native distal AVF and greater efficacy in the management of the prevailing dysfunctional AVF. In addition, it allows both minimizing and optimizing complementary examinations, with a reduction in health costs in fistulogram and phlebography. Although the data is encouraging and coincides with the majority of published series, still there is little information and more studies are needed to know the real impact that multidisciplinary teams can have on the creation and functional of AVF, quality of life of our patients and health care cost.
Financial statementIsciii Retic Redinren Rd016/009 Funds Feder.
Conflict of interestsThe authors declare that they have no conflicts of interest.
Please cite this article as: Aragoncillo Sauco I, Ligero Ramos JM, Vega Martínez A, Morales Muñoz ÁL, Abad Estébanez S, Macías Carmona N. Consulta de acceso vascular: resultados antes y después de la instauración de un programa multidisciplinar con realización de ecografía doppler de rutina. Nefrologia. 2018;38:616–621.



