




Recently, the Advanced Chronic Kidney Disease Units (UERCA) have been developed in Spain to offer a better quality of life to patients with ACKD, improving their survival and reducing morbidity in this phase of the disease. Nowadays, there is not much evidence in the Spanish and international literature regarding the structure and how to achieve these objectives in the UERCA. From the ERCA working group of the Spanish Society of Nephrology (S.E.N.), this project is promoted to improve care for ERCA patients through the definition of quality standards for the operation of the UERCA.
Material and MethodsAn initial proposal for quality standards concerning the operation of the UERCA was configured through consultation with the main sources of references and the advice of an expert working group through face-to-face and telematic meetings. Base on this initial proposal of standards, a survey was conducted and sent it via email to 121 nephrology specialist and nursing professionals with experience in Spanish UERCA to find out, among others, the suitability of each standards, that is, its mandatory nature or recommendation as standards. The access to the survey was allowed between July 16, 2018, until September 26, 2018.
ResultsA total of 95 (78,5%) professionals participated out of the 121 who were invited to participate. Of these, 80 of the participants were nephrology specialists and 15 nursing professionals, obtaining a varied representation of professionals from the Spanish geography. After analyzing the opinions of these participants, the standards were defined to a total of 68, 37 of them (54,4%) mandatory and 31 of them (45,5%) recommended. Besides, it was observed that the volume of patients attended in the UERCA is usually above 100 patients, and the referral criteria is generally below 25–29 ml/min/ 1.73 m2 of glomerular filtration.
ConclusionsThis work constitutes a first proposal of quality standards for the operation of UERCA in Spain. The definition of these standards has made it possible to establish the bases for the standardization of the organization of UERCAs, and to subsequently work on the configuration of a standards manual for the accreditation of ERCA Units.
Recientemente, se han desarrollado en España las Unidades de Enfermedad Renal Crónica Avanzada (UERCA) con el objetivo de ofrecer una mayor calidad de vida a los pacientes con ERCA, mejorar su supervivencia y disminuir la morbilidad en esta fase de la enfermedad. A día de hoy, hay poca evidencia en la literatura española e internacional con respecto a la estructura y cómo conseguir estos objetivos en las Unidades ERCA. Desde el grupo de trabajo ERCA de la Sociedad Española de Nefrología (S.E.N.), se impulsa este proyecto para mejorar la atención a los pacientes ERCA a través de la definición de estándares de calidad para el funcionamiento de las UERCA.
Material y MétodosSe conformó una propuesta inicial de estándares de calidad sobre el funcionamiento de las UERCA a través de la consulta de principales fuentes de referencias y el asesoramiento de un grupo de trabajo de expertos a través de reuniones presenciales y no presenciales. A partir de esta propuesta inicial de estándares, se diseñó y envío una encuesta vía correo electrónico a 121 especialistas de nefrología y profesionales de enfermería con experiencia en UERCA españolas para conocer entre otros, la idoneidad de cada estándar, es decir, su obligatoriedad o recomendación como estándar. Se permitió acceso a la encuesta entre el 16 de julio de 2018, hasta el 26 de septiembre de 2018.
ResultadosParticiparon un total de 95 (78,5%) profesionales de los 121 que fueron invitados a participar. De éstos, 80 de los participantes fueron especialistas en nefrología y 15 profesionales de enfermería, obteniéndose una variada representación de profesionales de la geografía española. Tras analizar las opiniones de estos participantes, los estándares quedaron definidos a un total de 68, 37 de ellos (54,4%) obligatorios y 31 de ellos (45,5%) recomendables. Además, se observó que el volumen de pacientes atendidos en las UERCA se sitúa usualmente por encima de los 100 pacientes, y que el criterio de derivación por regla general está por debajo de 25−29 ml/min/1,73 m2 de filtración glomerular.
ConclusionesEste trabajo constituye una primera propuesta de estándares de calidad para el funcionamiento de una UERCA en España. La definición de estos estándares ha permitido establecer las bases para la estandarización de la organización de las UERCA, y trabajar posteriormente en la configuración de un manual de estándares para la acreditación de Unidades ERCA.
Advanced chronic kidney disease (ACKD) is considered to be the stages 4 and 5 of chronic kidney disease (CKD). It is therefore defined as CKD with a severe decrease in glomerular filtration rate (GFR ) (<30 mL/min).1 ACKD is a public health problem due to its high prevalence and cost of care, and which is conditioned by high cardiovascular morbidity.2,3 With data obtained from the latest estimates of the prevalence of CKD in Spain, there could be around 100,000 people in the ACKD phase.4
In this context, in recent times the ACKD units (ERCAU) have been developed in our country, they are multidisciplinary care units for patients with ACKD with aiming to offer comprehensive care, higher quality of life, improving survival and reducing morbidity in this phase of the disease. In fact, in the Framework Document on Chronic Kidney Disease (CKD) within the Strategy for Addressing Chronicity in the National Health System of 2015, it is highlighted among its specific objectives to guarantee good care to the patient with CKD, offer support to the ACKD patient in all hospitals with Nephrology consultation, and to the extent possible, establish an ACKD consultation with a specific structure.5 Among the specific objectives of these clinics or ERCAU are identified the following items6–10: early detection of progressive kidney disease, prevent and treat ACKD complications (anemia, mineral metabolism abnormalities, malnutrition, acidosis, etc.), treat associated comorbidity (hypertension, dyslipidemia, smoking, etc…), delay the progression of ACKD until the need for renal replacement therapy (RRT), inform the patient of the possibilities of RRT or conservative therapy, prepare the patient in a prearranged manner to receive the most appropriate therapeutic option for their needs, whether it is conservative treatment or RRT, or establish measures to analyze the quality of care of these patients.
In “Nefrologia”, the Journal of the Spanish Society of Nephrology (SEN), in a publication in 2008, the integral care of the patient with ACKD is recognized as the main objective of the UERCA and as priority, the following objectives : 1) Healthcare objectives (early referral, delay progression, etc. ); 2) Programs directed to the patient, with training or progressive education in self-care, and 3) Analysis of quality of care with the monitoring of biological indicators, the planning for scheduled initiation of dialysis, quality of life and user satisfaction.10 In other national and international documents can be identified the definition of standards on the structure and organization of the ERCAU.11–13 In various publications, it is observed the great variability in the organization of the ERCA processes14,15 and indicate that there is room from improvement on areas such designation of resources, processes and results of the ERCAU.16
To improve the care of the patient with ERCA, it is required to evaluate carefully, with evidence-based methodology, the achievement of predetermined standards.17 Some scientific societies, both in the national and European environment, have developed accreditation programs in their own body of knowledge. Examples of these initiatives are those of the Spanish Society of Internal Medicine (“SEMI”),18 European Clinical Research Infrastructure Network (ECRIN),19 Spanish Society of Coloproctology (“AECP”),20 Spanish Society of Neurology (SEN),21 accreditation criteria for hospital emergency services,22 etc. Accreditation is a method to improve the organization and results of a service with the help of an accrediting body that evaluates the activity, comparing them with predetermined standards.23 A general example of an accreditation process is illustrated in Fig. 1. The purpose of measuring and monitoring the standards is to document the quality of healthcare, establish comparisons (benchmarking), support accreditation, allow the improvement of healthcare, and provide support to healthcare professionals, managers and decision-makers. Standards can be derived from the literature and based on evidence or, if there is not scientific evidence, they can be determined by a panel of experts and/or healthcare professionals through a consensus process based on their own experience. In this sense, various quality initiatives have been developed over time by SEM in other aspects of the specialty.24–27

Regarding the care of the patient with ACKD, the working group of ACKD from the SEN has worked on publications on the structure and operation of ERCAUs. However until now, a systematic attempt to develop quality standards and indicators for ACKD patient care, as well as an accreditation process, has not been carried out.
In this context, the SEN's ACKD working group carries out this work aiming to improve the care of ACKD patients through the definition of quality standards for the operation of the ERCAU. Such standards are based on the literature, on the consensus of working group of experts and through a survey of a large number of nephrology specialists and nursing professionals with experience in Spanish ERCAU.
MethodologyInitially, with the objective of providing advice and guiding the work to be carried out during the project, a working group was formed made up of nine members of the ERCA working group of the SEN. All members of the working group are nephrologists and have experience in management of ACKD patient in the ERCAU. Likewise, several of the members of this group also have experience in the accreditation of renal replacement treatment units, as well as specific knowledge in the different renal replacement treatment options (hemodialysis, peritoneal dialysis and kidney transplantation). The entire working group collaborated, participated and guaranteed the correct execution of all phases of the project.
In the first phase, it was generated a proposal of quality standards on the operation of the ERCAU; this was created by consulting the main sources of references: documentation corresponding to the ERCAU of the different Nephrology Services that are part of the working group, scientific guides of the SEN,2,26–30 Framework Document of the Ministry of health on Chronic Kidney Disease,5 and international guidelines.31 This proposed standards was reviewed and adjusted by the working group through face-to-face and non-face-to-face meetings. Through telematic interviews it was obtained and taken into consideration the opinion of representatives from the National Transplant Organization (ONT), the Spanish Society of Nephrological Nursing (SEDEN) and from patients through the Association for the Fight against Kidney Diseases (ALCER). In this way, an initial proposal of quality standards for the operation of a ERCAU was put together. The standards were grouped into five blocks (Fig. 2): (1) General requirements of the ERCAU; (2) Material and human resources; (3) Processes; (4) Rights and safety of patients; (5) Results. The working group validated this initial proposal of standards and assessed each of them as mandatory or recommended. A proposed standard was determined to be mandatory if more than 50% of the working group members considered it mandatory, and a standard was determined to be recommended when less than 50% of the working group members considered it mandatory.

In a second phase, based on the initial proposal of standards, a survey was designed to determine the suitability of each standard by collecting the opinion of nephrology specialists and nursing personnel. The objective of this survey was to obtain a broad external evaluation by experts to determine the value of the initial proposal of standards designed by the working group. A total of 121 nephrologists and nursing personnel from the national territory with work experience in ERCAU and part of the SEN and SEDEN were invited to participate via email. The selection of these experts was made based on the recommendations of the members of the working group. All invited professionals received the same standard email in which they were informed about the project, the objective of the survey was indicated and a link to access the survey was provided with the corresponding instructions. Access to the survey was allowed from the same day of the invitation, July 16, 2018, until September 26, 2018. During this time, reminders to complete the survey were sent periodically via email.
The survey included two parts. In one part, there were questions aiming to identify each professional (professional profile, hospital, Autonomous Community, email) and to know the degree of activity in the ERCAU consulted (number of patients treated at ERCAU / year, and criteria for referral to ERCAU according to GFR ( mL/min/1.73 m2 ). Four categories were established according to the volume of patients seen (0–99, 100–200, 201–300, 301–500) and referral criteria by GFR used in the center (15–19, 20–24, 25−29, >30). A second part was dedicated to obtain information on the relevance, nature and possible modifications of each of the standards of the initial proposal agreed upon by the working group were consulted. Therefore, for each of the 82 standards, three questions were asked: (1) Do you consider appropriate to include this standard in the manual? (relevance). The response was requested was limited to two options: "Yes" and "No". (2) Do you consider that it should be "mandatory" to obtain quality accreditation or should be just "recommended" (nature). A closed response was requested to two options: "mandatory" and "recommended". (3) Do you want to add any additional comments about this? (modifications). A response was requested in an open text field. The entire survey was developed on the 123FormBuilder® platform.
After finishing the deadline to respond to the survey, in a third phase, the results of the responses obtained were analyzed. On the one hand, the response rate of the participants and the results were analyzed in relation to the number of patients seen at the ERCAU/year and the criteria for referral to ERCAU according to GFR, with the aim of knowing the burden of care activity. On the other hand, an analysis of the suitability of each standard was carried out in order to adjust the proposed standards. For this analysis, the evaluation criteria for each of these aspects were decided in consensus with working group. Regarding the relevance of the standard, it was determined that a standard was included in the manual if at least 80% of the participants considered it appropriate to include it; if this assessment was less than 80%, it was determined that the standard was not included. Regarding the category of the standard, it was determined that a standard was mandatory if at least 50% of the participants considered it mandatory, and it was determined that a standard was recommended when less than 50% of the participants considered it mandatory. Regarding the possible modifications, comments were registered for most of the standards, and they were analyzed with the aim of improving the definition of each standard.
Finally, after obtaining the results of the analysis, the conclusions were presented to the working group in a meeting with the aim of reaching a consensus on a final proposal of quality standards for the operation of ERCAU, that was based on their experience and results of the analysis of the survey. This final proposal served as the basis and was later added to a final document that was approved by representatives of SEN, SEDEN, ONT and ALCER for publication.
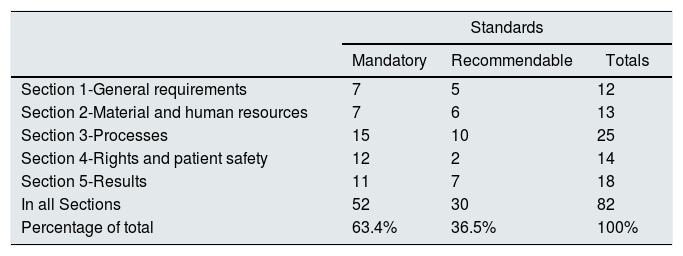
ResultsAfter completion of the work of the first phase through the review of the references, the contributions of representatives of scientific societies (SEN, SEDEN, ONT) and patients association (ALCER) and, the adjustment made by the work group there were identified a total of 82 quality standards for the operation of a ERCAU. Of these standards, 12 (14.6%) refer to general requirements of the ERCAU, 13 (15.8%) are related to material and human resources, 25 (30.4%) are directly linked to the processes of ERCAU, 14 (17%) are associated with the rights and safety of the patient and 18 (21.9%) with results. In addition, the working group classified 52 (63.4%) standards as mandatory and 30 (36.5%) standards as recommended (Table 1).
Initial proposal made by the working group.
| Standards | |||
|---|---|---|---|
| Mandatory | Recommendable | Totals | |
| Section 1-General requirements | 7 | 5 | 12 |
| Section 2-Material and human resources | 7 | 6 | 13 |
| Section 3-Processes | 15 | 10 | 25 |
| Section 4-Rights and patient safety | 12 | 2 | 14 |
| Section 5-Results | 11 | 7 | 18 |
| In all Sections | 52 | 30 | 82 |
| Percentage of total | 63.4% | 36.5% | 100% |
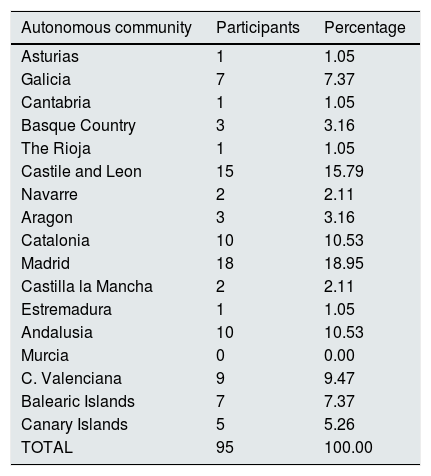
Regarding the results of the survey, of the 121 health professionals invited to participate (nephrology specialists and nursing staff), a total of 95 (78.5%) accepted and completed the entire survey; of these, 80 were nephrology specialists and 15 nursing professionals, obtaining a varied representation of professionals from the Spanish geography as it is shown in Table 2. Given a total of 121 invited professionals, it is considered that with a confidence level of 95%, with a precision of 5%, and assuming an expected proportion of 50%, with a sample size of 93 participants the results are representative. Regarding the number of patients seen in the ERCAU/year and the criterion for referral to the ERCAU according to GFR, the participants indicated that the volume of patients seen in the UERCA is usually above 100 patients (Fig. 3) and that the referral criterion is a GFR generally below 25−29 mL/min/1.73 m2 (Fig. 4).
Participants in the survey by Autonomous Community. Total number of participants by Autonomous Communities and percentage of the total.
| Autonomous community | Participants | Percentage |
|---|---|---|
| Asturias | 1 | 1.05 |
| Galicia | 7 | 7.37 |
| Cantabria | 1 | 1.05 |
| Basque Country | 3 | 3.16 |
| The Rioja | 1 | 1.05 |
| Castile and Leon | 15 | 15.79 |
| Navarre | 2 | 2.11 |
| Aragon | 3 | 3.16 |
| Catalonia | 10 | 10.53 |
| Madrid | 18 | 18.95 |
| Castilla la Mancha | 2 | 2.11 |
| Estremadura | 1 | 1.05 |
| Andalusia | 10 | 10.53 |
| Murcia | 0 | 0.00 |
| C. Valenciana | 9 | 9.47 |
| Balearic Islands | 7 | 7.37 |
| Canary Islands | 5 | 5.26 |
| TOTAL | 95 | 100.00 |
.")
.")
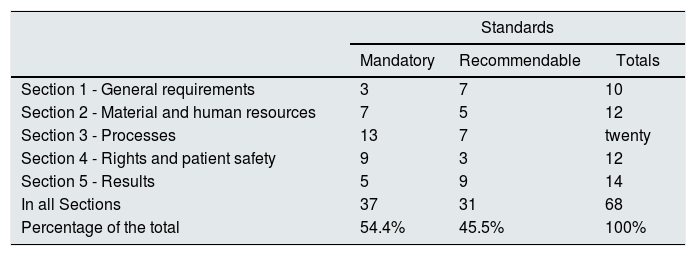
Regarding the assessment of the 82 standards proposed by the working group, the survey participants rated 68 (82.9%) as appropriate to include in a manual of standards and 14 (17.07%) as not relevant to include in a standards manual. Of these 68 standards, 37 (54.4%) were rated as mandatory and 31 (45.5%) as recommended (Table 3). Table 4 shows the definition of each standard with details of its assessment of its relevance for inclusion in a manual and its nature, mandatory or recommended. For the drafting of the standards, it begins with "must" when it was considered mandatory and begins with "recommended" when it is recommended. In addition, there were proposed modifications and improvements in the wording of the definition of the standards. These considerations were assessed to subsequently adjust the wording in the development of the standards manual.
Results obtained from the survey.
| Standards | |||
|---|---|---|---|
| Mandatory | Recommendable | Totals | |
| Section 1 - General requirements | 3 | 7 | 10 |
| Section 2 - Material and human resources | 7 | 5 | 12 |
| Section 3 - Processes | 13 | 7 | twenty |
| Section 4 - Rights and patient safety | 9 | 3 | 12 |
| Section 5 - Results | 5 | 9 | 14 |
| In all Sections | 37 | 31 | 68 |
| Percentage of the total | 54.4% | 45.5% | 100% |
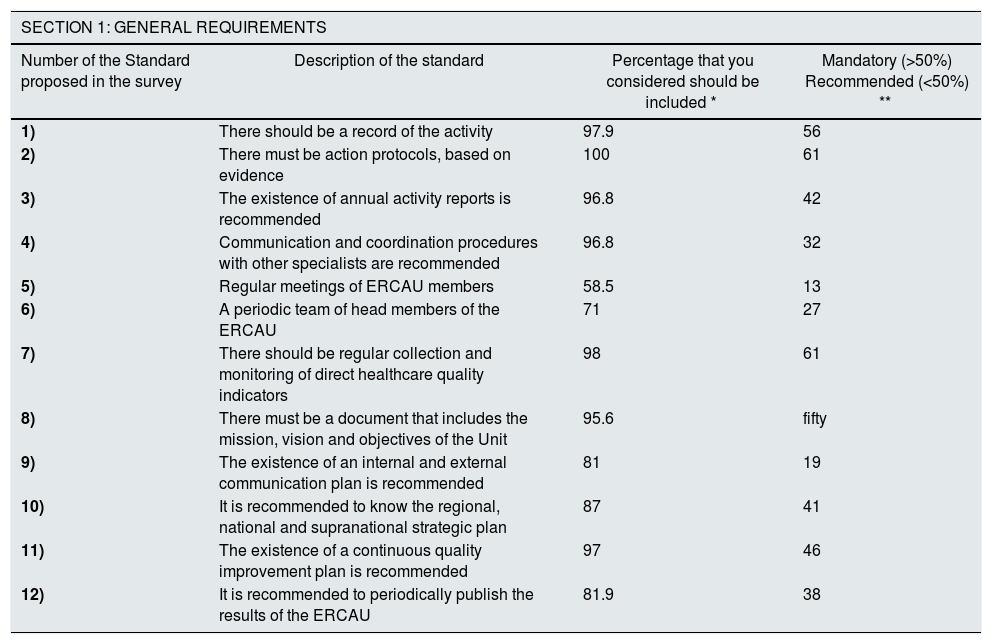
Standards accepted and eliminated from each of the survey sections.
| SECTION 1: GENERAL REQUIREMENTS | |||
|---|---|---|---|
| Number of the Standard proposed in the survey | Description of the standard | Percentage that you considered should be included * | Mandatory (>50%) Recommended (<50%) ** |
| 1) | There should be a record of the activity | 97.9 | 56 |
| 2) | There must be action protocols, based on evidence | 100 | 61 |
| 3) | The existence of annual activity reports is recommended | 96.8 | 42 |
| 4) | Communication and coordination procedures with other specialists are recommended | 96.8 | 32 |
| 5) | Regular meetings of ERCAU members | 58.5 | 13 |
| 6) | A periodic team of head members of the ERCAU | 71 | 27 |
| 7) | There should be regular collection and monitoring of direct healthcare quality indicators | 98 | 61 |
| 8) | There must be a document that includes the mission, vision and objectives of the Unit | 95.6 | fifty |
| 9) | The existence of an internal and external communication plan is recommended | 81 | 19 |
| 10) | It is recommended to know the regional, national and supranational strategic plan | 87 | 41 |
| 11) | The existence of a continuous quality improvement plan is recommended | 97 | 46 |
| 12) | It is recommended to periodically publish the results of the ERCAU | 81.9 | 38 |
| SECTION 2: MATERIAL AND HUMAN RESOURCES | |||
|---|---|---|---|
| Number of the Standard proposed in the survey | Description of the standard | Percentage who considered that it should be included * | Mandatory (>50%)/Recommended (<50%) ** |
| 1) | The ERCAU should have a multidisciplinary nature | 98.9 | 94 |
| 2) | Validated scales should be used for comprehensive assessment of the patient | 98.9 | 57 |
| 3) | Patient education materials must be available | 100 | 82 |
| 4) | Tools to aid shared decision making should be used | 96.8 | 67 |
| 5) | A nephrologist is recommended for 250−300 patients and a nurse for 125−250 patients | 94.6 | 49 |
| 6) | You must have access to various professional profiles, as well as diagnostic tests, and other services | 96.7 | 55 |
| 7) | The design and evaluation of the competences of the members of the ERCA unit in the care, teaching and research fields is recommended. | 85.1 | 47 |
| 8) | It is recommended that the ERCAU have a physical space (own or shared) to hold clinical sessions and teaching of the health team | 89.4 | 2. 3 |
| 9) | Ways and / or resources must be available for the study of the living kidney donor for the anticipated transplant | 96.8 | 67 |
| 10) | Access to other profiles associated with the management of ACKD is recommended: dietitian / nutritionist; physiotherapist; psychologist; pharmacist and social worker | 87.1 | 16 |
| 11) | A referral doctor and nurse must be available for each ERCAU patient | 94.7 | 71 |
| 12) | A reception plan is recommended for professionals who join ERCAU (medical and nursing staff) | 81.9 | 29 |
| 13) | The ERCAU has telecommunication applications to provide healthcare activity to patients | 72.3 | 9 |
| SECTION 3: PROCESSES | |||
|---|---|---|---|
| Number of the Standard proposed in the survey | Description of the standard | Percentage who considered that it should be included * | Mandatory (>50%)/Recommended (<50%) ** |
| 1) | The criteria for referring the patient from the outpatient clinic of the Nephrology Service to the ERCAU must be defined. | 100 | 79 |
| 2) | The patient should be referred to the ERCAU stage 4 (glomerular filtration < 30 mL / min / 1.73 m 2 ) with progression criteria, and at least 12 months before starting RRT | 90.3 | 62 |
| 3) | There must be a protocol for referral to the UERCA of patients with kidney transplant failure to ensure their continuity of care and their access to the process of deliberation-selection-preparation for RRT | 82.8 | 58 |
| 4) | Information must be provided to patients orally and in writing about: the objectives and operation of the ERCAU, the contact details of the ERCAU (telephone number and hours of operation ) and the unambiguous identification of referent professionals in the ERCAU | 95.7 | 63 |
| 5) | The ERCAU, prior to the start of the decision-making process, conducts eligibility tests for the different RRTs, so that it can start the information process of the different RRT techniques without delay. | 72 | 46 |
| 6) | The educational process of the RRT of the patient and / or family must be planned, establishing a minimum of two visits, in person or online, which are scheduled according to their needs | 94.6 | 74 |
| 7) | There must be specific protocols and materials to inform patients, in a staggered manner and adjusted to their cognitive capacity and other needs, about: basic notions of ACKD, objectives to be achieved, healthy lifestyle habits, indications for self-care, types of RRT and possible complications | 98.9 | 69 |
| 8) | It is recommended to have tools to evaluate the knowledge acquired by the patient about the information provided, aimed at identifying informational needs and resolving doubts. | 89.2 | 3. 4 |
| 9) | There must be a protocol for shared decision making that facilitates planning of the sequential use of the different techniques throughout the evolution of the disease: HD, PD, transplantation, conservative treatment | 93.5 | 55 |
| 10) | It is recommended to provide the patient with information about patient associations and the encounters with "expert patients" they can access. | 95.7 | 19 |
| 11) | There must be procedures in place and applied for completing the informed consent document after the patient's choice of RRT technique or conservative treatment. After its proper completion, a copy of it will be incorporated to the medical record and another will be delivered to the patient | 94.6 | 80 |
| 12) | It is recommended that coordination protocols are in place with the PC and other specialists in charge of palliative care to plan conservative treatment activities for ACKD. | 97.8 | 38 |
| 13) | There should be a specific protocol for patients entering conservative treatment, which includes aspects such as conservative renal management and pain control. | 94.5 | 56 |
| 14) | There must be a protocol for the early identification and assessment of candidates for kidney transplantation that is carried out during the first consultations, and inclusion on the waiting list for kidney transplantation and anticipated kidney transplantation before starting RRT, where the documentation necessary for its inclusion, the information that must be provided to the patient, and the coordination required between the kidney transplant center and the person in charge of the ERCAU | 94.6 | 65 |
| 15) | It is recommended that, after the patient's discharge, the ERCAU exchange information with the professionals involved in the following stages of the patient's care process | 82.6 | 39 |
| 16) | Protocols must be available for the evaluation of the patient in his first and subsequent visits, the compilation of his medical history, and the preparation of a summary of the main diagnoses and problems that presented over the years, including clinical judgments and updated treatments in the electronic prescription | 92.4 | 59 |
| 17) | There should be a specific protocol for information, deliberation and preparation for RRT aimed at patients who start it in an unscheduled manner. | 90.2 | 56 |
| 18) | The ERCAU provides the patient with documentation of anticipated wills | 79.1 | 29 |
| 19) | An individualized care plan should be defined for patients with vascular or peritoneal access. | 91.3 | 68 |
| 20) | It is recommended that the patient be approached holistically, taking into account his bio - psycho- socio-spiritual dimension | 87.1 | 32 |
| 21) | It is recommended that the ERCAU be involved in the development of research projects, individual and / or in collaboration with other agents, whose contents are aligned with the strategic lines of health research plans in different areas (hospital, regional, national, and European) | 90.3 | 7 |
| 22) | The ERCAU has mechanisms to identify competitive funding calls for research projects | 63 | 3 |
| 23) | ERCAU carries out a periodic evaluation of the skills of the professionals that make up its team to identify their training and professional development needs | 79.3 | twenty-one |
| 24) | The ERCAU has a methodology for evaluating the degree of improvement in the results of its professionals after carrying out continuous training activities | 68.8 | fifteen |
| 25) | It is recommended that the UERCA have a training program that includes the minimum requirements requested to the house staffs. | 89.2 | 43 |
| SECTION 4: RIGHTS AND SAFETY OF THE PATIENT | |||
|---|---|---|---|
| Number of the standard proposed in the survey | Description of the standard | Percentage who considered that it should be included* | Mandatory (>50%)/Recommended (<50%)** |
| 1) | The right to intimacy and privacy of patients must be guaranteed during healthcare | 96.8 | 100 |
| 2) | The right of patients, after receiving adequate information, to make decisions about their own healthcare process (information process, education, preparation and selection of the different RRT) must be ensured. | 97.8 | 95 |
| 3) | The patient must receive the necessary documentation in order to record the informed consent of the diagnostic and / or therapeutic actions required. A copy signed by the patient will be stored in the electronic medical record or similar record system | 100 | 90 |
| 4) | There must be a procedure for "substitution in decision-making" (family member, guardian or legal representative), in conditions of incapacity or when the patient is not capable, intellectually or emotionally, of understanding the scope of the intervention, in case of doubts the Hospital Ethics Committee will be consulted. | 92.4 | 78 |
| 5) | The recommendations of the reference Ethics Committee should be consulted and taken into account for carrying out R & D & i activities | 84.6 | 44 |
| 6) | When the health care required does not conform to the organization's portfolio of services, it is necessary to give the patient information about t referral to other centers, and this communication will be recorded in the electronic medical record | 95.7 | 62 |
| 7) | If the patient wants to know, will receive information on their situation in the transplant waiting list. | 80.4 | 62 |
| 8) | It is recommended that access to the necessary resources be facilitated to receive professional support with the objective of promoting the integration at different levels, social, labor, educational and family. | 88.2 | 25 |
| 9) | ERCAU patients participating in research projects are required to give their informed consent, having been previously informed of: the objectives, the methodology, the potential risks and benefits, and the alternatives to their non-participation in the project | 91.3 | 85 |
| 10) | The ERCAU has an integrated security plan that specifies the use of alarms and monitors, the elimination of dangerous elements, and the elaboration of a registry of error detected in healthcare practice, among others. | 75.3 | 35 |
| 11) | There should be conciliation of the medication prescribed and taken by the patient seen in the regular visit to the clinic | 86.7 | 59 |
| 12) | Participation in the notification of adverse events according to the established hospital protocol, analyze sentinel events and implement improvements in the procedures involved | 90.2 | 57 |
| 13) | Patients have access to the documents that guarantee their rights, such as the portfolio of services and their relationship with other levels of care, the reception plan, the code of ethics, the protocols that guarantee security, confidentiality and legal access to their data and the complaints and suggestions book, as well as access to documents that informabout their obligations, such as respect for health personnel | 74.2 | 30 |
| 14) | It is recommended the participation of patients in the school patient and/or as patient mentors, as well as contact with the local patient association | 89.2 | 10 |
| BLOCK 5: RESULTS | |||
|---|---|---|---|
| Number of the standard proposed in the survey | Description of the standard | Percentage who considered that it should be included* | Mandatory (>50%)/Recommended (<50%)** |
| 1) | It is recommended to perform and analyze an annual satisfaction survey of all patients and establish improvement plans based on the results obtained | 86 | 28 |
| 2) | The written complaints received from patients and relatives must be collected, analyzed and answered, establishing an improvement plan based on these responses. | 94.6 | 52 |
| 3) | It is recommended that more than 90% of patients that leave the ERCAU have eligibility test performed. | 81.7 | 44 |
| 4) | More than 90% of the patients from the ERCAU with a follow-up time of at least six months should start the RRT with a signed protocol of information-choice of RRT | 96.7 | 51 |
| 5) | It should be accomplished that 100% of the patients (both those with “optimal programmed initiation” and those with “non-optimal programmed initiation” of RRT ) have gone through information, deliberation and preparation process of RRT | 95.7 | 52 |
| 6) | It is recommended that among the patients eligible for transplantation, the ERCAU initiate the procedure for the inclusion of the patient on the waiting list in a percentage higher than 80% | 88.2 | 44 |
| 7) | It is recommended that the percentage of incident patients on peritoneal dialysis be equal to or greater than 20% of the total and equal to or greater than 30% of those from ERCAU with more than six months of follow-up | 85.9 | 21 |
| 8) | It is recommended that the referral of patients for the creation of an arteriovenous fistula (AVF) be 90% of the eligible patients, and be performed when the glomerular filtration rate is < 15 mL / min / 1.73 m2 | 94.6 | 40 |
| 9) | It should be achieved that 100% of adult ERCAU patients who are detected anemia with Hb levels < 10 g/dL are given treatment for it (erythropoiesis stimulating agents +/- iron) | 95.6 | 67 |
| 10) | 100% of patients must have complete viral serology data before reaching the chosen RRT technique, and the information on transmission risks | 96.8 | 81 |
| 11) | The percentage of attendance at the training activities given to professionals who are part of the UERCA is> 80% | 71 | 31 |
| 12) | It is recommended that the percentage of patients from the UERCA with more than six months of follow-up who start RRT on a scheduled basis be > 75% (percentage of the total number of patients excluding deaths ). | 94.6 | 35 |
| 13) | It is recommended that the percentage of patients who attend the ERCAU consultation with the record of blood pressure and the medication they are taking be> 90%. | 83.9 | 37 |
| 14) | The percentage of patients of the total eligible who after receiving the educational process choose home technique is equal to or greater than 50% | 64.1 | 20 |
| 15) | It is recommended that the percentage of patients who start the modality of RRT that they had chosen be> 70% | 89 | 21 |
| 16) | It is recommended that the percentage of patients from RECAU who start hemodialysis with a mature arteriovenous fistula with a previous follow up of at least six months be equal to or greater than 75% | 90.2 | 37 |
| 17) | The ERCAU team carries out annually: at least one publication in indexed scientific journals and / or an individual research project or in collaboration with other institutions and at least one participation in a scientific congress | 64 | 6 |
| 18) | The ERCAU assesses and analyzes the satisfaction of professionals in certain aspects, such as workload, participation in defining objectives, continuing training, etc. | 78.5 | 19 |
TSR:
With these results, the working group, based on its experience, adjusted the final proposal for the operation of an ERCAU to 70 quality standards. This final result has been added and included in the Manual of Standards Accreditation Project ERCA Units.32
DiscussionThe Spanish Society of Nephrology (SEN), for years, given the health priority posed by CKD, has worked to improve care for the ACKD patient through the development of multidisciplinary care units, UERCA.1 The implementation of these units has also been promoted at international level.14 However, both in the Spanish and international literature, there is variability in the organization and operation of these units.14–16
Therefore, this work constitutes the first attempt to describe ERCAU operating standards in Spain in relation to general aspects of organization, resources (material and human), processes, patient safety and results. The contributions of the project's working group, representatives of scientific societies and the evaluations by a wide panel of experts from the national level allow establishing a series of criteria for the configuration and optimal development of an ERCA Unit.
General requirementsIn relation to the general requirements that a ERCAU must have, the experts point out the need and responsibility to document the mission, vision and objectives of the Unit, as well as a map of processes (attendance, teaching and i + D + i) that simplify its organization. In this sense, it is considered advisable to previously identify the Strategic Plan on ERCA of its autonomous, national or supranational scope in order to define the objectives of each ERCAU.
In addition, the ERCAU must have a record of healthcare, teaching, research activity and available resources (material and human) that allow and facilitate the organization and planning of resources. Along these lines, there is also evidence of the suitability of recording relevant data of the patient's information in order to facilitate its monitoring. Some of the relevant data are identified by the working group: GFR level, rate of CKD progression, eligibility test, dates related to decision-making, selected technique, inclusion in the transplant waiting list (living or cadaveric), hospital admissions, death in the ERCA stage or within the first three months of TRS, events that affect their safety.
With regard to healthcare activity, the definition of updated protocols of main clinical processes (entry of the patient into the ERCAU, process to help decision-making, risk assessment, conservative treatment, patient withdrawal) should be considered as mandatory in all ERCAU. For the definition of these protocols, as well as the rest of the healthcare activity of the ERCAU, it is recommended according to what is reported,10,33 to define coordination and communication mechanisms within the same Unit, with the rest of the nephrology department and with other healthcare units involved in the care of patients with ACKD (transplant unit, radiology and angio radiology, vascular/general surgery, palliative care, cardiology, preventive medicine, emergencies, social work, psychology, etc.).
On the other hand, a ERCAU must establish the collection and periodic monitoring of healthcare quality indicators, and it would be advisable to publish its results periodically, both internally and externally, together with other information of interest on teaching or research activities.34 Along these lines, it would be recommended that the ERCAU had a quality plan to promote improvement through the definition and evaluation of these indicators in order to implement corrective and preventive actions.10 Also, the experts point out that it would be advisable to prepare an annual report that contains information on resources, activity and results.21
Human and material resourcesIt is clear that the ERCAU must have the appropriate team to carry out the activities, as well as have a multidisciplinary team that allows a comprehensive approach to the patient.10 Thus, it is recommended to have a nephrology specialist for every 250−300 patients and a professional nurse for every 125−250 patients, establishing a reference doctor and nurse for each patient. According to the opinion of experts and references in clinical guidelines, these ratios are estimated to guarantee continuity in work and excellence in care at ERCAU.34 Thus, the team made by nephrologist and nursing constitutes the nucleus of health professionals that conform the ERCAU.10 According to the experts, it is advisable to strengthen their professional skills, both healthcare, teaching and research, through plans of up-to-date training, reception plans and an adequate description of functions, roles and responsibilities.34,35
In addition, communication circuits should be established with other professionals involved in the care of the ACKD patient (vascular / general surgery, interventional nephrology, palliative care, cardiology, preventive medicine, emergencies, transplant unit).10,34 It is also recommended to facilitate access to other profiles associated with ACKD management to guarantee holistic patient care10: nutrition, physiotherapy, psychology, psychiatry, pharmacy or social work.
The UERCA must have the necessary material to support healthcare activity.10 Among these materials, the experts indicate, according to their experience and the bibliography,10,33 that the material should include: tools to aid shared decision-making, education and training materials for patients on the management of ACKD and the techniques of RRT (brochures, audiovisual media, app, etc.), or scales for the comprehensive assessment of the patient (frailty, dependence, comorbidity, functionality, socio-family situation, emotional state, nutritional status and patient progression). The use of these materials must be validated and supported by scientific evidence.
In relation to structural resources, an ERCAU must include a medical and a nursing clinic for consultation, with own physical space and agenda to carry out patient education and training activities.10,33 Furthermore, as indicated in the bibliography,10 it is recommended that the ERCAU have a physical space (own or shared) to hold clinical sessions and teaching of the health team.
ProcessesThe ERCAU should have defined the criteria for referring the patient from the outpatient clinic of the nephrology service to the ERCAU.10 The referral to ERCAU should be established in stage 4 of ACKD (glomerular filtration rate <30 mL/min/1.73 m2 with criteria of disease progression, and at least 12 months before starting RRT.10,36
As previously mentioned, there should be stablished protocols with primary care, palliative care and other professionals involved in the management of patients with ACKD to reinforce communication and coordination of health care.10,36 There should be protocols related to the early identification and evaluation of candidates for kidney transplantation and inclusion in the waiting list for kidney transplantation and anticipated kidney transplantation, individualized care plan for patients with vascular or peritoneal access, and a referral protocol to the ACKD Unit of patients with kidney transplant failure to ensure their continuity of care.36
In cases where the patient is discharged, it is recommended to generate protocols to guarantee the adequate exchange of information with the professionals involved in the patient's transition after discharge.33
With respect to the relationship with the patient, there must be established and identified the processes or procedures necessary to guarantee adequate patient care: protocols for the evaluation of the patient in their visits to the ERCAU, shared decision-making, completion of informed consent, information to patients about how the ERCAU function, education on ACKD and comorbidities, training and deliberation about the RRT techniques.10,33,34,36 Along these lines, experts recommend having tools to assess the knowledge acquired by the patient about the information provided, aimed at identifying information needs and resolving doubts, and providing the patient with information about patient associations and meetings with expert patients that they may have access.
Patient rights and safetyAnother fundamental aspet to guarantee the optimal functioning of a ERCAU is the incorporation of measures and standards on the rights and safety of the patient. This work highlights that in the ERCAU, the patient must come first, and, consequently, the fulfillment of their rights and safety throughout the entire care process.
It is considered that a ERCAU should guarantee the right to intimacy and privacy of patients during health care with adequate physical spaces that limit to a maximum of one patient per clinical visit.34,37
The ERCAU must also provide adequate information to patients and guarantee its own decision-making about the healthcare process (process of information, education, preparation and selection of the different RRT, situation on the waiting list).10,27,34 In this line, the necessary documentation for the registration of informed consent must be provided for all activities that require it (diagnosis, therapy, research or substitution of decision-making, among others).35,37
In cases which the health care required by the patient does not fit within the organization's portfolio of services, the patient must be provided with the corresponding information for referral to other centers, and this communication must be registered in the medical record.35
Regarding safety, the experts add that a process must be established in the ERCAU to notify adverse events and other incidents, with the purpose being analyzed t and implement improvements in the procedures involved. In this regard, the need to establish measures to guarantee the conciliation of medication is also pointed out.
It is considered as good and advisable practice to promote the participation of patients in the patient school, contact with the local patient association, as well as facilitate access to the necessary resources to receive professional support aimed at promoting social, labor, educational and family inclusion of the patient.37
ResultsThe definition of standards in the section of results allows for a systematic measurement and analysis of quality indicators that provide key information to objectively monitor healthcare activity at ERCAU and identify the improvements made in service management. The aim is to promote the achievement of the objectives of a ERCAU in accordance with the definition of standards according to the consensus of experts and the available scientific evidence.
Therefore, an ERCAU must, among other things, promote that all patients receive adequate information prior to choosing RRT, and that the indication of their RRT will take place on a scheduled basis. Also, it is recommended that patients starting hemodialysis have a mature arteriovenous fistula performed and that the percentage of patients electing peritoneal dialysis be encouraged.
The ERCAU should collect, analyze and respond to the written complaints received from patients and relatives, establishing an improvement plan based on these responses.21 Along these lines, it is also recommended to carry out and analyze an annual satisfaction survey of all patients and establish improvement plans based on the results obtained.21,35
Like in all studies, the present work has strengths and limitations. Despite the intention and interest ofcontacting all the nephrologists who work on ACKD, this has not been possible and consequently there is the possibility of some bias. This survey is based on the perception/opinion of nephrology specialists and nursing staff about how the structure, resources, processes, safety and patient outcomes should be, therefore, its results are probably closely connected with the daily practice of the ERCAU in Spain, and in some cases it may be distant from formal aspects of more structured documents and/or sources of knowledge. Another possible weakness is that at some point the formulation of the indicator has not been understood and there is a misinterpretation, as in the case of establishing the eligibility of the treatments that has not been deemed mandatory. In addition, we recognize the need to work in future studies on the definition of standards focused on the evaluation of clinical aspects, in addition to those more related to the optimization of the healthcare process. In addition, it is urgent to evaluate the feasibility of achieving the standards in subsequent works. Certainly, the evaluations reported will allow to establish a first balance of mandatory and recommended standards as an initial starting point to carry out the development of actions in relation to the operation of a ERCAU. In addition, in this evaluation the representation of patients through the Association for the Fight against Kidney Diseases (ALCER) and the National Transplant Organization (ONT) must be highlighted, parties clearly interested in patient-centered care and clarity and lack of bias in the inflows to the various RRT options.
In conclusion, this work has allowed the configuration of a first proposal of standards for the operation of a ERCAU. After a subsequent work and review of these standards by the working group, 70 quality standards were defined, collected in the first version of the document, Manual of Standards Project Accreditation Units ERCA.33 The first version of this manual is a first approach to advance towards improving the quality of ERCAU, establishing a starting framework that reduces the variability between the different centers in the development of ERCAU and offers CKD patients the same opportunities care, regardless of where they are cared for. The definition of the standards in this manual is understood as an open process, that recognizes the possibility of requiring a reduction, an increase or a redefinition of standards according to new evidences or needs of clinical practice.
SponsorThe company Baxter SL® has financed the work required to carry out the opinion survey analyzed in this study.
Conflict of interestsThe authors declare that they have no conflicts of interest.
To all members of the ERCA working group, as authors, for their dedication, disposition and contributions throughout the development of the work. Special thanks to the Association for the Fight Against Kidney Diseases (ALCER), the National Transplant Organization (ONT) and all the professionals (nephrologists and nurses) who have collaborated in the project. Finally, we would like to thank Ascendo Consulting Sanidad & Farma ® for its participation as technical office and Baxter SL® for their collaboration to make the project possible.
Please cite this article as: Prieto-Velasco M, Pino MDDP, Buades Fuster JM, et al. Unidades de Enfermedad Renal Crónica Avanzada en España: una encuesta nacional sobre los estándares de estructura, recursos, resultados y seguridad del paciente. Nefrologia. 2020;40:608–622.



