

After years with no randomised, controlled clinical trials in the field of acute kidney injury (AKI) in critically ill patients, the results of two important clinical trials have been recently published (AKIKI1 and ELAIN2), aiming to resolve uncertainties about the optimal timing for initiating dialysis in critically ill patients with AKI.
Despite decades of research, the incidence of AKI continues to rise, and the mortality rate remains high.3–5 In the early 2000s, the main study objective was the dialysis dose, based on the hypothesis that a higher dose of dialysis would result in better renal and patient survival outcomes in dialysis-dependent AKI patients. The study by Bouman et al.6 was one of the first to question this hypothesis, and showed that the dialysis dose does not improve survival in these patients; this hypothesis was definitively rejected after publication of the results of the ATN7 and RENAL studies.8 Moreover, Bouman et al. found no differences, in terms of survival, with initiating replacement therapy at an early stage.6
Now the important question is when is the best time to start dialysis in these types of patients, i.e. would early dialysis improve renal and patients survival?
The current evidence comes from observational studies.8–11 Two meta-analyses12,13 suggest a survival benefit associated with early initiation of dialysis. Probably, the benefits may be explained by the better control of fluid therapy and water/electrolyte imbalance and the elimination of toxins, which would all help to prevent complications such as gastrointestinal bleeding and encephalopathy.14
The main limitation of these observational studies is the fact that they had no control group; all patients received renal replacement therapy. However, the possibility of spontaneous renal recovery being facilitated by delayed initiation of therapy has not been evaluated.
As detailed below the results of two studies are contradictory and provide no clear answer. In the Artificial Kidney Initiation in Kidney Injury (AKIKI) study, no benefit was obtained from early initiation of dialysis as compared to delayed initiation in septic patients; however, in the early versus delayed initiation of renal replacement therapy in AKI (ELAIN) study, very early initiation of a renal replacement technique could be beneficial in surgical patients with less severe AKI.
Artificial kidney initiation in kidney injury studyThe first study designed to answer this question was the open-label, randomised, French multicentre study, AKIKI, which compared early versus delayed initiation of dialysis therapy in severely ill patients with AKI. The primary endpoint was patient survival at 60 days. Patients were randomised 1:1 at the time of diagnosis of KDIGO stage 3 AKI to the “early” treatment group (as soon as possible), or “delayed” treatment group (when the patient met one of the criteria considered as signs for urgent dialysis which had been used prior to randomisation as study exclusion criteria).
Exclusion criteria were: oliguria for more than 72h, elevated BUN, hyperkalaemia, major acidosis, acute pulmonary oedema due to volume overload that causes hypoxaemia with oxygen flow requirements despite diuretic treatment.
The choice of haemodialysis technique (continuous or intermittent), its duration and interval between sessions was at the discretion of each centre. The subjects were adult patients in intensive care units (ICU) diagnosed with AKI secondary to ischaemic acute tubular necrosis or KDIGO stage 3 nephrotoxicity. All patients were intubated or on treatment with vasopressor drugs.
A total of 620 patients were randomised: 312 to the early group and 308 to the delayed group. Of the overall cohort, 80% of patients were diagnosed with sepsis and 63% were diagnosed with AKI secondary to nephrotoxicity; 80% were on vasoactive drugs and a similar percentage required ventilatory support by way of orotracheal intubation. In the early group, patients started haemodialysis a mean of 4.3h after diagnosis of KDIGO stage 3 AKI. Of the patients in the delayed group, only 50% received dialysis, starting after an average of 57h after diagnosis and randomisation. Intermittent haemodialysis techniques were used in 50% of the patients and continuous therapies in 30%. With respect to the primary endpoint, the mortality rate at 60 days after randomisation was 50%, being similar in both groups. No differences were found in complications potentially related to the dialysis technique, with the exception of catheter-associated infections, which were more common in the early group, and hypophosphataemia, more common in the delayed group. Although survival curves were similar in both groups, recovery of renal function, defined as recovery of diuresis, was faster in the delayed group. In this study, the strategy of delaying the initiation of dialysis in seriously ill AKI patients made the dialysis procedure unnecessary in 50% of the patients.
Early versus delayed initiation of renal replacement therapy in AKI studyThe second study was a clinical trial conducted at a German centre that compared early versus delayed initiation of dialysis therapy in seriously ill patients with AKI; the primary endpoint was patient survival at 90 days. Inclusion criteria were: age 18–90 years, diagnosis of KDIGO stage 2 AKI, plasma neutrophil gelatinase-associated lipocin (NGAL) levels >150ng/mL and one of the following conditions: severe sepsis, need for catecholamines, pulmonary oedema refractory to diuretic treatment or progression on the SOFA score.
Exclusion criteria were prior grade 4 or 5 chronic kidney disease or AKI resulting from causes other than acute tubular necrosis (thrombotic, interstitial, glomerular or obstructive). Patients were randomised to the early haemodialysis group, in which treatment was initiated within 8h after randomisation or to the delayed group, with initiation of dialysis within 12h after progression to KDIGO stage 3 or when one of the absolute criteria for initiation of dialysis occurred (elevated urea, hyperkalaemia, hypermagnesaemia, diuresis <200mL/12h or anuria, or diuretic-resistant oedema). Patients were predominantly surgical, 47% having a history of heart surgery and a high percentage on mechanical ventilation and requiring vasoactive drugs. All were treated by continuous dialysis techniques using the same protocol to ensure uniformity in treatment.
A total of 231 patients were randomised, 112 patients to the early group and 119 patients to the delayed group; all those in the early group received dialysis, compared to only 89% (n=108) in the delayed group. The mean time from meeting all inclusion criteria to the initiation of dialysis was 6h in the early group and 25.5h in the delayed group. At the time of randomisation, there were no differences between the two groups in terms of renal function. Mortality at 90 days was lower in the early group (44/112) than in the delayed group (65/119), HR 0.66 (CI 0.045–0.97, p=0.03). The early dialysis group was found to have greater renal recovery at 90 days, reduced mechanical ventilation time, and decreased hospital admission time, compared to the delayed initiation group.
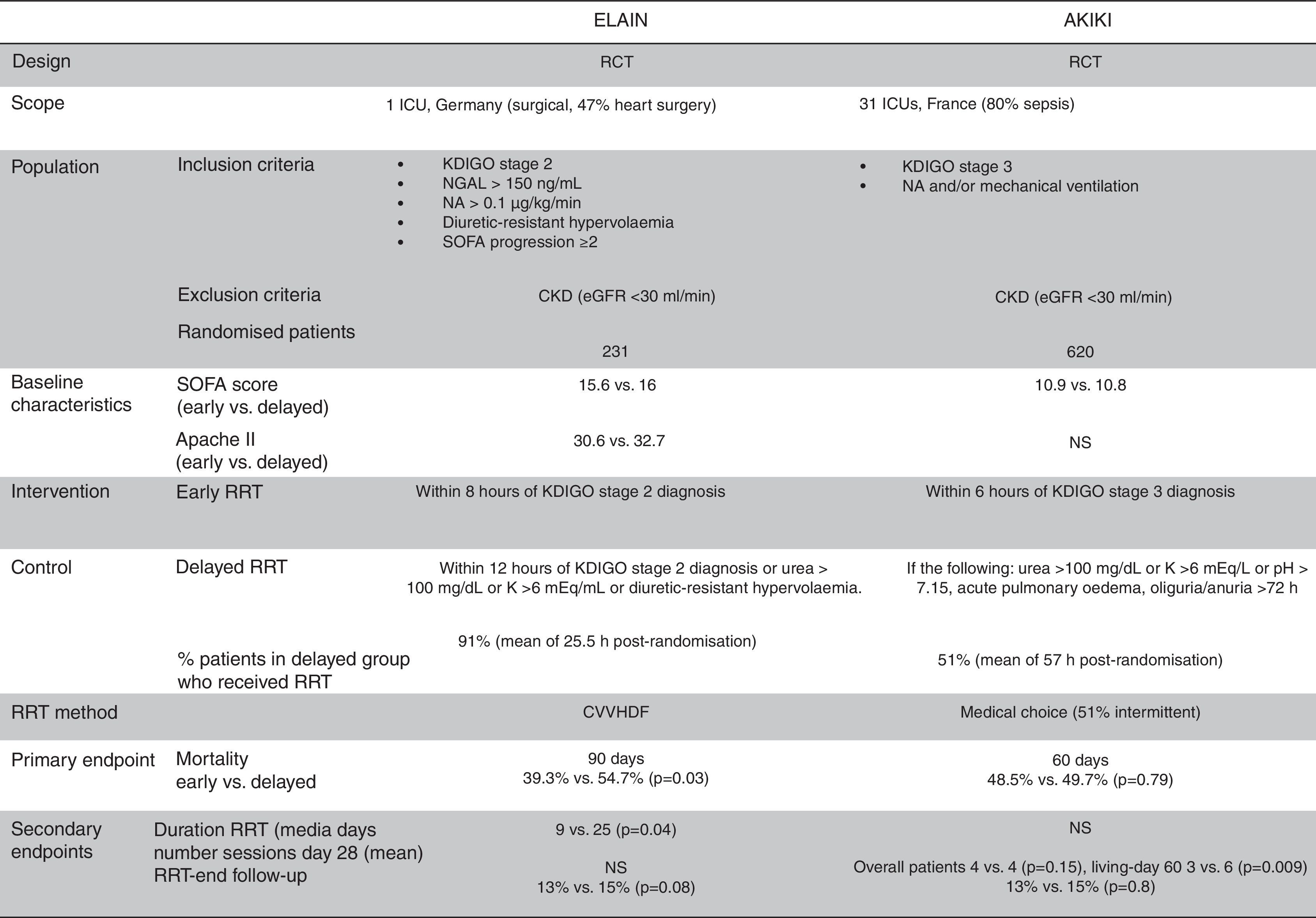
Contradictory resultsWhen analysing the contradictory results between the two studies, it is essential to analyse the differences carefully (Table 1). In addition to the obvious differences in the number of patients included and the number of participating centres in each study, there is a major difference in the type of patients in each study: AKIKI included serious ill patients due to medical causes, predominantly septic patients, although with a lower incidence of multiple organ failure (SOFA∼11) than in the ELAIN cohort; ELAIN included surgical patients with a higher incidence of multiple organ failure (SOFA∼16) and greater severity as measured by the APACHE scale (∼30). There are also differences in the indication for dialysis: in the AKIKI study, it is indicated “early” in KDIGO stage 3, whereas in ELAIN, it is indicated “very early” in KDIGO stage 2. There are also subtle differences between the delayed indication groups in the two studies: the ELAIN study consists of KDIGO stage 3 patients (85%) or patients with certain metabolic abnormalities (15%), meaning that in practice, the ELAIN delayed indication group is practically the same as the early indication group in the AKIKI study. The dialysis groups should therefore be renamed as follows: in ELAIN “very early indication” versus “early indication”; and in AKIKI “early indication” versus “conventional indication”. Moreover, we are unable to explain why a short delay in the initiation of therapy in the ELAIN study could result in a significant decrease in both the duration of therapy and the number of hospital admission days. There are also differences regarding the type and dose of dialysis: in the AKIKI study, the individual doctors decided, and exact modalities and dosages were not detailed in the published text. In the ELAIN study, both modality and dose were defined (continuous veno-venous haemodiafiltration, 30mL/kg/h with 100% predilution) but, unlike the AKIKI study, the criteria for maintaining or withdrawing therapy are not specified.
In terms of the validity of the data provided by the two studies, the authors of the AKIKI study formulated the following hypothesis: delayed renal replacement therapy may provide an absolute survival benefit of at least 15%, with a statistical power of 90% and a significance level of 5%. The authors of the ELAIN study had almost the opposite hypothesis: early renal replacement therapy may provide an absolute survival rate of 18% with a statistical power of 80% and the same level of significance.
In conclusion, in the AKIKI study, early initiation of a dialysis technique in septic patients with severe AKI provided no benefit over the more conventional delayed initiation. The ELAIN study, although with fewer patients, less importance and quality, and conducted in surgical patients with less severe AKI, suggests that very early initiation of renal replacement may be beneficial.
A meta-analysis of 9 randomised clinical trials comparing the early initiation of dialysis versus standard practice in critically ill patients admitted to the ICU with AKI confirmed that there were no differences in mortality rates between the two groups.15 Despite the significant efforts, the uncertainty about the optimal timing for initiating dialysis in patients with AKI persists. A search with the terms “acute kidney injury” AND “renal replacement therapy” at ClinicalTrials.gov produces a total of 208 projects focusing on multiple aspects such as technical modality, biomarkers, etc.; only two express interest in the optimal timing for initiating dialysis in these patients. One of these was from a randomised pilot study in Canada,16 which provided key points for the design of a large-scale trial that is now fully underway (NCT02568722). The other, limited to patients with septic shock, is a French multicentre trial that is still in the patient inclusion phase (NCT01682590).17 A large sample, a certain degree of uniformity in baseline diagnoses, with validation of the classification systems,18,19 very controlled randomisation and the application of biomarkers as surrogate variables20,21 are essential requirements for generating high-quality responses.
Please cite this article as: Rodríguez García E, Pascual Santos J. ¿Cuándo iniciar diálisis en la insuficiencia renal aguda en pacientes críticos?. Nefrologia. 2017;37:563–566.



