
On the occasion of the publication in your journal of the excellent review by Montero N. et al. of GEENDIAB (Spanish Study Group on Diabetic Nephropathy)1 entitled “Clinical Practice Guideline for detection and management of diabetic kidney disease: A consensus report by the Spanish Society of Nephrology” as family physicians who treat these patients we wanted to contribute an aspect not present in the aforementioned review.
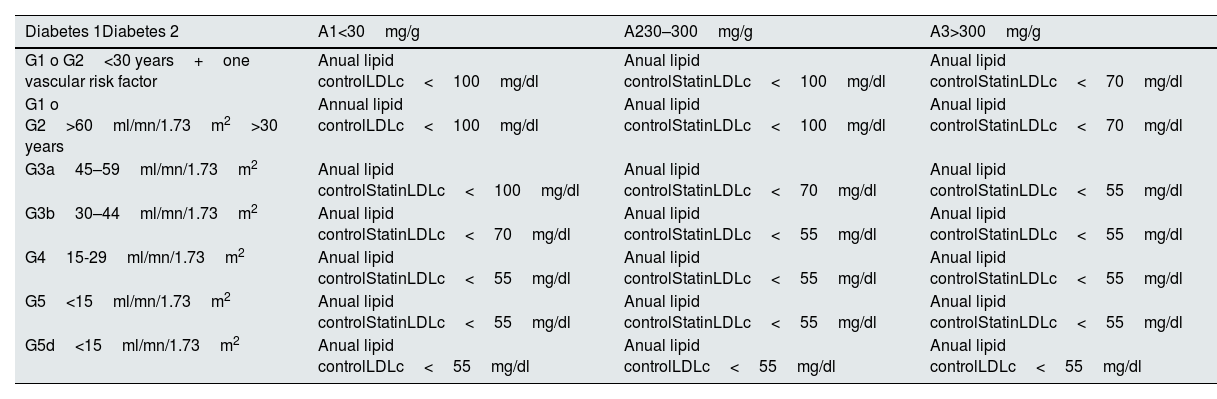
In our usual practice we consider lipid control to be key in a review on chronic kidney disease (CKD) and type 1 or 2 diabetes due to the increased risk of vascular disease in these patients and because it is a modifiable risk factor. Today, good lipid control is considered an independent objective for the improvement of patients with CKD and diabetes. Together with measures aimed at improving lifestyles, blood pressure control, weight loss, metabolic control, smoking cessation and thrombotic risk control.2 The still valid 2021 guidelines by Visseren FLJ et al. of the ESC Scientific Document Group.3 “2021 ESC Guidelines on cardiovascular disease prevention in clinical practice” recommend starting statins regardless of cholesterol levels in patients with glomerular filtration rate<60ml/min/1.73m2, with doubts about maintaining or starting it in stage 5d (Dialysis). In the same document and taking into account the presence of albuminuria as an independent risk factor, the ideal control target is recommended: LDL Cholesterol<100mg/dl in G1, G2 and A1, <70mg/dl or 50% reduction of baseline LDLc in G3 and A2 CKD, LDLc<55mg/dl in G4, G5 and A3. In Table 1, we have categorized by color according to risk (mortality from any cause, vascular mortality, renal progression or failure) following the KDIGO recommendation adapted by Marques Vidas et al.4
Proposed first-line treatment and control objective.
| Diabetes 1Diabetes 2 | A1<30mg/g | A230–300mg/g | A3>300mg/g |
|---|---|---|---|
| G1 o G2<30 years+one vascular risk factor | Anual lipid controlLDLc<100mg/dl | Anual lipid controlStatinLDLc<100mg/dl | Anual lipid controlStatinLDLc<70mg/dl |
| G1 o G2>60ml/mn/1.73m2>30 years | Annual lipid controlLDLc<100mg/dl | Anual lipid controlStatinLDLc<100mg/dl | Anual lipid controlStatinLDLc<70mg/dl |
| G3a45–59ml/mn/1.73m2 | Anual lipid controlStatinLDLc<100mg/dl | Anual lipid controlStatinLDLc<70mg/dl | Anual lipid controlStatinLDLc<55mg/dl |
| G3b30–44ml/mn/1.73m2 | Anual lipid controlStatinLDLc<70mg/dl | Anual lipid controlStatinLDLc<55mg/dl | Anual lipid controlStatinLDLc<55mg/dl |
| G415-29ml/mn/1.73m2 | Anual lipid controlStatinLDLc<55mg/dl | Anual lipid controlStatinLDLc<55mg/dl | Anual lipid controlStatinLDLc<55mg/dl |
| G5<15ml/mn/1.73m2 | Anual lipid controlStatinLDLc<55mg/dl | Anual lipid controlStatinLDLc<55mg/dl | Anual lipid controlStatinLDLc<55mg/dl |
| G5d<15ml/mn/1.73m2 | Anual lipid controlLDLc<55mg/dl | Anual lipid controlLDLc<55mg/dl | Anual lipid controlLDLc<55mg/dl |
Statins: atorvastatin 20mg/day up to 80mg/day (care<30ml/min/1.73m2) or Rosuvastatin 10mg/day, 5mg/day if <30ml/min/1.73m2; Ezetimibe: if statin intolerance 10mg/day or complement (no adjustment required); Bempedoic Acid: together with ezetimibe and statins, or in statin intolerant and ezetimibe is insufficient and Primary Hypercholesterolemia do not use<30ml/min/1.73m2; Inclisiran: In patient with recurrent vascular event or heterozygous familial hypercholesterolemia do not use<30ml/min/1.73m2; IPCSK9 (alirocumab, evolucumab): in patients with heterozygous Primary and Familial Hypercholesterolemia with High Vascular Risk do not use<30ml/min/1.73m2; Icosapent ethyl: limited experience in CKD, indicated in patients with DM and residual risk.
The recent publication by Zac-Varghese S. et al. “Clinical practice guideline for the management of lipids in adults with diabetic kidney disease” from the Joint Association of British Clinical Diabetologists and UK Kidney Association,5 very much in line with the NICE guidelines, makes the recommendations included in Table 1. Among these recommendations, the following stand out: In all stages of CKD with Diabetes, statins (atorvastatin 20mg) are recommended in patients with filtration>45ml/min/1.73m2 and it is recommended to intensify statins if necessary. If maximum doses of statins cannot be used, ezetimibe should be associated. In statin intolerance, ezetimibe should be used. In patients with filtration>45ml/min/1.73m2 with poor control and high risk, bempedoic acid can be recommended. Inclisiran and PCSK9 inhibitors should be used above 30ml/min/1.73m2 and in the prescribed conditions (familial hypercholesterolemia, primary hypercholesterolemia, poor control and repeated vascular events). Fibrates are recommended in young patients and with filtration>45ml/min/1.73m2, and there is no experience in CKD with Icosapent ethyl for patients with residual risk and high triglycerides.
With these recommendations we aim to update the optimal treatment and control of lipids and their extra risk in patients with type 1 and type 2 diabetes with CKD as a summary of the guidelines and their corresponding consulted evidence, for the use of the clinician who faces these patients on a daily basis.



