


Patients on hemodialysis (HD) are at risk of COVID-19 for several reasons. In previous studies, the mortality rate of HD patients with COVID-19 was higher (16.3%) than that of the general population (2–3%).1 Most prospective therapeutic trials have excluded patients on HD for safety reasons. There is no adequate infection control of COVID-19 for HD patients, although these patients are one of the most vulnerable groups to contract SARS-CoV-2 infection.
Remdesivir was approved as the first antiviral agent by the FDA in 2020. However, at first, remdesivir was not suggested for patients with a low estimated glomerular filtration rate (eGFR) because its adverse event was renal impairment. Aiswarya et al. reported the efficacy and safety of remdesivir in HD patients.2 Since August 2021, the Japanese guidelines have described the possibility of remdesivir for HD patients.3
We present our clinical experience with remdesivir in 25 patients with COVID-19 on HD and support its efficacy and safety. According to a previous report,2 remdesivir was administered at a dose of 100mg/day on day 1, 4h before HD. Subsequent doses of up to a maximum of six doses were administered 4h before each HD. Neutralizing antibody (Sotrovimab) was administered intravenously to all patients 48h after admission.
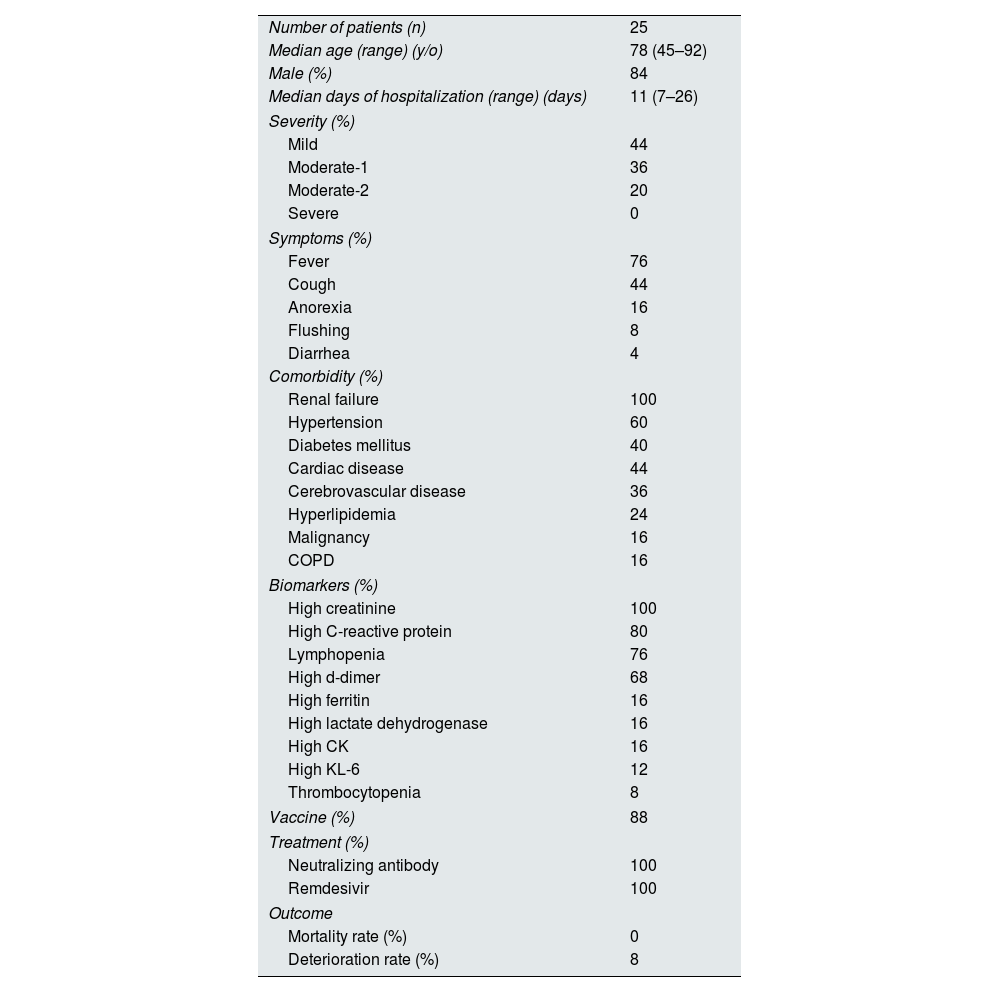
The median age of the patients was 78 years (range, 45–92 years) and was predominantly male (84%). The median duration of hospitalization was 11 days (range: 7–26 days). A total of 44% of the patients had mild disease, 36% had moderate-1 (pneumonia without oxygen), and 20% had moderate-2 (pneumonia with oxygen). Among them, 88% of the patients were vaccinated and 60% of the patients developed COVID-19 due to a cluster of facilities.
The most common symptoms were fever (76%), cough (44%), anorexia (16%), flushing (8%), and diarrhea (4%) (Table 1).
Patients’ characteristics.
| Number of patients (n) | 25 |
| Median age (range) (y/o) | 78 (45–92) |
| Male (%) | 84 |
| Median days of hospitalization (range) (days) | 11 (7–26) |
| Severity (%) | |
| Mild | 44 |
| Moderate-1 | 36 |
| Moderate-2 | 20 |
| Severe | 0 |
| Symptoms (%) | |
| Fever | 76 |
| Cough | 44 |
| Anorexia | 16 |
| Flushing | 8 |
| Diarrhea | 4 |
| Comorbidity (%) | |
| Renal failure | 100 |
| Hypertension | 60 |
| Diabetes mellitus | 40 |
| Cardiac disease | 44 |
| Cerebrovascular disease | 36 |
| Hyperlipidemia | 24 |
| Malignancy | 16 |
| COPD | 16 |
| Biomarkers (%) | |
| High creatinine | 100 |
| High C-reactive protein | 80 |
| Lymphopenia | 76 |
| High d-dimer | 68 |
| High ferritin | 16 |
| High lactate dehydrogenase | 16 |
| High CK | 16 |
| High KL-6 | 12 |
| Thrombocytopenia | 8 |
| Vaccine (%) | 88 |
| Treatment (%) | |
| Neutralizing antibody | 100 |
| Remdesivir | 100 |
| Outcome | |
| Mortality rate (%) | 0 |
| Deterioration rate (%) | 8 |
COPD: chronic obstructive pulmonary disease; CK: creatine kinase.
The most common comorbidities were renal failure (100%), hypertension (60%), cardiac disease (44%), diabetes mellitus (40%), cerebrovascular disease (36%), hyperlipidemia (24%), malignancy (16%), and chronic obstructive pulmonary disease (COPD) (16%).
The most frequent biomarkers were elevated creatinine (100%), followed by C-reactive protein (80%), lymphopenia (76%), D-dimer (68%), ferritin (16%), lactate dehydrogenase (16%), creatinine kinase (16%), KL-6 (12%), and thrombocytopenia (8%).
Two patients experienced deterioration. One patient with pneumonia at admission developed respiratory distress on day 8 and was started on oxygen therapy. The patient was started on dexamethasone; however, the patient did not respond to the treatment. He was then switched to steroid plus (methylprednisolone 1000mg/day on days 1–3, 125mg/day on days 4–5). The patient recovered from respiratory distress and was discharged on day 22. The remaining patient did not have pneumonia upon admission. He developed pneumonia on day 8 and was started on oxygen therapy. He was treated with dexamethasone and recovered from respiratory distress on day 20. None of the patients developed severe disease. All patients recovered from COVID-19 and were discharged.
A total of 20% of the patients showed persistent low-grade fever for 14 days, and 24% of the patients developed aspiration pneumonia. Various persistent symptoms have been reported. Swallowing function is damaged due to severe COVID-19 has been reported.4 In elderly patients, there is a possibility of decreased activity of daily living due to long-term hospitalization and decreased swallowing function due to COVID-19.
In our cohort, all patients recovered from the disease; therefore, there were no factors to evaluate the efficacy of remdesivir. Upon admission, some biomarkers showed an abnormal range above the standard value. We used these biomarkers and compared the data obtained before and after remdesivir treatment. The most frequent biomarker was creatinine level. However, we could not use it since all patients had renal failure; therefore, C-reactive protein and lymphocyte counts were used. C-reactive protein levels were significantly decreased (p<0.001), whereas lymphocyte counts did not show differences before and after remdesivir treatment (p=0.925) (Table 2). This is consistent with a previous study.2 C-reactive protein may be an independent parameter that reflects the efficacy of remdesivir.
Recently, Kikuchi et al. reported data on patients with COVID-19 on HD in the Japanese population. Among the 1010 patients, 98 received remdesivir. Patients treated with remdesivir had shortened hospitalization (16.2±8.1 days vs. 20.9±13.2 days) and better prognosis (Hazard ratio, 0.45; 95% CI, 0.26–0.80, p=0.004) compared to those who did not receive remdesivir.5
Our study had some limitations. First, this study included a small sample of patients from a single center. We only included patients with mild to moderate, without severe disease. Second, most of our patients were elderly, as a regional characteristic of the large elderly population. Data on patients undergoing HD are required; therefore, regardless of limitations, we believe that it is worth reporting on our practical experience.
We hope that our study helps frontline healthcare workers in the treatment of COVID-19.
Conflict of interestThe authors report no declarations of interest.
Statement of ethicsThis study was conducted following the ethical principles of the Declaration of Helsinki and was approved by the institutional review board of Biwako Ohashi Hospital.
We thank Yuu Tochitani, Rika Umeda, Shizuka Morita, Yohei Takano, Masanori Fujiie, Tsutomu Ito, Ayako Igosaki, and Satomi Ozawa for their assistance.



