



Almost 10% of kidney transplants present an episode of humoral rejection during its evolution,1 which decreases long-term graft survival. There are several published trials about the use of tocilizumab (TCZ) in patients with chronic active humoral rejection as first line therapy and rescue treatment, with good results in graft survival.2 The experience thus far has supported intravenous TCZ, so we present a case with administration of subcutaneous TCZ.
A 25-year-old man with a history of chronic renal disease due to Alport disease, who was in peritoneal dialysis for two years, received a kidney transplant from a living donor in June 2013, with 1 HLA matched (A) and no previous antibodies.
In 2014, the patient developed three de novo donor specific antibodies (DSA). Kidney graft biopsy was performed which showed acute mixed cellular and humoral rejection of renal allograft, treated with a bolus of corticosteroids, plasmapheresis, intravenous immunoglobulin (IVIg) and a cycle of bortezomib.
Eight months later he developed increased antibodies titres. Therefore, a new kidney graft biopsy was performed, showing active humoral rejection that was treated again with IVIg and a second cycle of bortezomib.
In February 2018, DSA DQ6 was no longer detected and in February 2019, a kidney biopsy was performed, confirming a diagnosis of chronic active humoral rejection. He was then started on treatment with IV TCZ (8mg/kg/monthly). After 12 months (March 2020) of treatment due to the needs of COVID-19 pandemic, the route of administration was changed to subcutaneous (dose 162mg/weekly).
Histologic control was performed 16 months after the start of treatment (June 2020), showing significant improvement in C4d deposits, reduction in inflammation in areas of interstitial fibrosis/tubular atrophy (IFTA), progression of transplant glomerulopathy and disappearance of DSA DQ2.
At the present moment, he continues treatment with SC TCZ weekly with good tolerance and without complications. During the entire follow-up, he has presented stable kidney renal function and proteinuria of less than 500mg/g (Fig. 1).
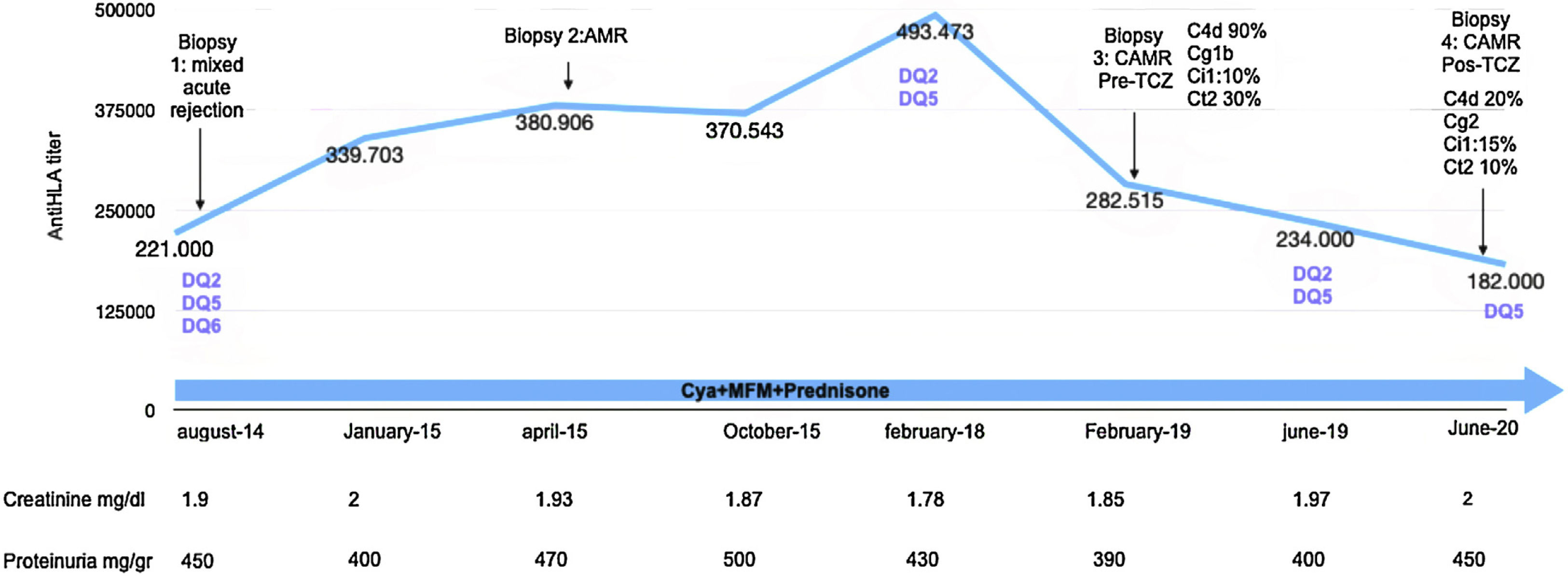
Follow-up renal function, proteinuria and histologic findings. AMR: antibody mediated rejection; CAMR: chronic active antibody mediated rejection; Cya: ciclosporin; MFM: mycophenolate mofetil; Cg: transplant glomerulopathy; Ci: interstitial fibrosis; Ct; tubular atrophy; iIFTA: inflammation in areas of interstitial fibrosis/tubular atrophy.
Intravenous TCZ was approved for use in the European Union (EU) in 2009 to treat rheumatoid arthritis (RA) and juvenile idiopathic arthritis.3
In October 2013, US FDA approved a subcutaneous formulation of TCZ for use in RA based on two trials: BREVACTA,3 which compared the subcutaneous TCZ with placebo without differences in articular response at week 24 and with similar adverse reactions, and SUMMACTA4 which showed no inferiority of subcutaneous TCZ compared to the intravenous one, with similar safety profile, apart from more injection site reactions with SC TCZ.
Iwamoto et al.,5 evaluated a cohort of 58 patients with RA and concluded that after change in formulation from IV TCZ to SC TCZ, the joint response was maintained.
In kidney transplant, there is no data regarding the use of subcutaneous TCZ; nevertheless, based on the trials reported and the favourable outcome of our patient, we could consider this form of administration, a treatment option that benefits patients.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.



