
Rhabdomyolysis (RBD) is a syndrome characterised by skeletal muscle necrosis and the release into the bloodstream of the intracellular constituents, which can lead to severe acute kidney injury (AKI). The causes of the RBD may be divided into traumatic and non-traumatic or metabolic, which in turn can be divided into several hereditary causes (disorders of gluconeogenesis, mitochondrial myopathies) and acquired, such as drugs, infections, toxins, ischaemia or vascular occlusion processes, exertional myolysis (strenuous exercise, seizures), electrolyte disorders (sodium disorders, hypokalaemia, hypomagnesaemia, hypophosphataemia, hypocalcaemia), endocrine disorders (diabetic ketoacidosis, hyperosmolar state, myxoedema, hyperaldosteronism) and inflammatory autoimmune myopathies.1–6 There are few published studies on RBD and AKI associated with Clostridium difficile (CD).
We present the case of a 60-year-old man with chronic liver disease. He had an eight-day history of diarrhoea. The results of the tests performed are shown in Table 1 according to the timeline. The patient's inflammatory diarrhoea was found to have AB toxins positive for CD, for which he received metronidazole and later oral vancomycin; he then developed acute kidney injury (AKI), elevated creatine phosphokinase (CPK) and elevated liver enzymes. Urinalysis showed myoglobinuria. Hydration was given with crystalloids, and there was an improvement in AKI and muscle pain and normalisation of CPK. Seven days later, the patient was discharged from hospital asymptomatic.
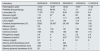
Laboratory tests and patient follow-up.
| Laboratory | 05/03/2018 | 07/03/2018 | 09/03/2018 | 10/03/2018 | 11/03/2018 |
|---|---|---|---|---|---|
| Haemoglobin (g/dl) | 13.44 | 12.87 | 12.08 | 10.87 | 11.34 |
| Platelets (thousands/μg) | 90.22 | 88.46 | 12.1 | 12 | 12.3 |
| Leucocytes (%) | 11.03 | 10.3 | 9.49 | 5.91 | 6.4 |
| Glucose (mg/dl) | 115 | 97 | 94 | 65 | 68 |
| Creatinine (mg/dl) | 0.87 | 1 | 1.71 | 2.78 | 2.1 |
| Urea (mg/dl) | 61.4 | 114 | 146 | 174 | 112 |
| Creatine phosphokinase (U/l) | 2525 | 32,437 | 29,130 | 924 | 126 |
| Albumin (g/dl) | 2.3 | – | – | – | 1.97 |
| Sodium (mmol/l) | 133 | 134 | 131 | 133 | 136 |
| Chlorine (mmol/l) | 108 | 105 | 106 | 98 | 110 |
| Phosphorus (mg/dl) | 3.6 | 4 | 4.2 | 2.5 | 2.9 |
| Potassium (mmol/l) | 5.4 | 5 | 5.67 | 5.73 | 4.8 |
| Calcium (mg/dl) | 9.7 | 9 | 9 | 9.1 | 9 |
| Alanine aminotransferase (IU/l) | 182 | – | 444 | – | – |
| Aspartate aminotransferase (IU/l) | 834 | – | 1814 | – | – |
| Gamma-glutamyl transferase (IU/l) | 25 | – | 21 | – | – |
Laboratory tests are shown on admission and during hospitalisation until returning to normal.
RBD may cause AKI in up to 33% of cases. The risk is usually low when CPK levels are below 15,000–20,000IU/l, but it can occur with values starting from 5000IU/l. It has been proposed by consensus that to induce AKI the CPK should be over 100 times its highest normal value, accompanied by a clinical syndrome.2
There are three pathogenic mechanisms involved in the development of RBD-related AKI: vasoconstriction, tubular obstruction and direct oxidative damage of myoglobin in renal tubuler cells.1–6
Tubular obstruction and oxidative injury is due to the precipitation of the Tamm-Horsfall protein with myoglobin; under physiological conditions, myoglobin is reabsorbed by the renal tubule cells, but when the presence of this pigment exceeds the reabsorptive capacity, it precipitates in the tubules as pigmentary cylinders,2 forming hyaline cylinders and causing endothelial dysfunction and tissue damage due to multiple cytokines, TNF-α, thromboxane A2 and endothelin. This all activates the sympathetic nervous system, the renin–angiotensin–aldosterone system and vasopressin release, which together reduce urine output.2 Last of all, the haem component of myoglobin causes oxidative damage in the tubules due to the production of active iron-induced oxygen radicals.1–6
Clinical expression varies from asymptomatic forms to electrolyte imbalance, respiratory distress syndrome, AKI, disseminated intravascular coagulation and multiple organ failure.7 The most common clinical presentation is muscle pain (84%), dark urine (80%), weakness (73%) and muscle swelling (8.1%).4
Infections are an uncommon cause of RBD, representing approximately 5% of cases, and 33–50% of them go on to develop AKI.8 There are few cases of RBD caused by CD reported in the literature. The Food and Drug Administration (FDA) has reported nine cases to date.9 Muralikrishna et al. reported the first case of RBD caused by CD, in a 57-year-old male with a history of irritable bowel syndrome with diarrhoea; CD was confirmed by ELISA of stool sample with the test positive for A and B toxins, with elevation of CPK>25,300IU/l and elevation of urinary myoglobin. The patient was treated with intravenous fluids, metronidazole and oral vancomycin. His symptoms resolved completely and he was discharged one week after admission.10 The FDA cases were males aged 50–59. In terms of comorbidities, eight of the nine patients were post-transplant, with dyslipidaemia and metabolic acidosis, and the other patient had rheumatoid arthritis. All the cases were taking prednisone and six of them (66.77%) were also taking sodium bicarbonate, simvastatin, dalteparin and darbepoetin. Clinical presentation was with AKI in eight patients (88.89%), myopathy and hyperkalaemia in five patients (55.56%) and diarrhoea in only 33%.9 The combination of drugs with risk of RBD, immunosuppression by steroids, chronic kidney disease or chronic liver disease in our patient are known risk factors for CD, but little is known about the risk of developing RBD. The mechanism behind RBD caused by CD is uncertain, but the direct cytotoxic effect of CD toxins remains the most likely possibility.10 The description of additional cases with RBD and AKI caused by CD would aid our understanding of the pathophysiological mechanisms of this serious complication and help standardise management.
Please cite this article as: Navarro-Blackaller G, Chávez-Iñiguez JS, Maggiani-Aguilera P, Gómez-Hernández GL, Carreón-Bautista EE, Moreno-Alvarado RA, et al. Rabdomiólisis y daño renal agudo asociado a infección por Clostridium difficile, reporte de caso. Nefrologia. 2019;39:208–209.



