
There is clear evidence about the role of low-density lipoproteins (LDL) in the process of atherosclerosis. Chronic kidney disease (CKD) entails high/very high cardiovascular risk (CVR) associated with multiple classic and non-classic CVR factors related to CKD. Despite the evidence for the benefit of lowering LDL cholesterol (LDL-C), the percentage of the population achieving guideline-recommended goals, including in CKD, remains low.1 In recent years, proprotein convertase subtilisin/kexin type 9 inhibitors (PCSK9i) have been shown to reduce the risk of cardiovascular disease (CVD) when added to statin therapy by potently lowering LDL-C levels.2
The aim of this retrospective observational study was to evaluate the profile of patients who started treatment with PCSK9i (alirocumab or evolocumab), added to their usual lipid-lowering treatment, when they did not meet the recommended LDL-C goal according to their CVR, from a Nephrology unit, and the lab test changes achieved with this treatment.3 The LDL-C goal in high CVR was <70mg/dl and in very high CVR<55mg/dl. The Hospital Dr. Peset ethics committee approved the study.
We define high-intensity lipid-lowering therapy (HILLT)4 as high-intensity statins alone (atorvastatin 40−80mg, rosuvastatin 20mg) or medium-intensity statins (atorvastatin 10–20mg, rosuvastatin 5−10mg, pitavastatin 2−4mg) combined with ezetimibe. We define atherogenic dyslipidaemia (DL) as triglycerides (TG) >150mg/dl, together with HDL cholesterol (HDL-C) <40mg/dl in men or <45mg/dl in women.
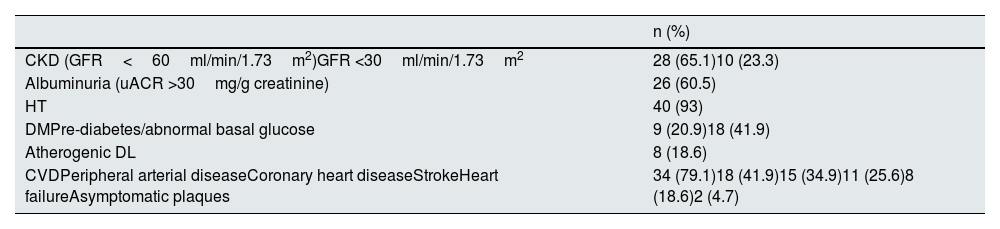
In total, 43 patients were analysed, with a median follow-up of 12 (7–19) months: mean age 65±12 years, 58.1% of the series were male. 65.1% had CKD and there were five kidney transplant patients (11.6%). 79.1% had a history of CVD. There were 13 statin-intolerant patients (30.2%); 69.8% were on statins and 34.9% on ezetimibe (32.6% of the series on statin-ezetimibe combination); 58.1% of the series were taking HILLT. The baseline clinical characteristics of these patients are shown in Table 1. In 79.1% of cases the first PCSK9i prescribed was evolocumab. Only three patients (7.1%) had to discontinue the drug due to intolerance.
Baseline characteristics of the series.
| n (%) | |
|---|---|
| CKD (GFR<60ml/min/1.73m2)GFR <30ml/min/1.73m2 | 28 (65.1)10 (23.3) |
| Albuminuria (uACR >30mg/g creatinine) | 26 (60.5) |
| HT | 40 (93) |
| DMPre-diabetes/abnormal basal glucose | 9 (20.9)18 (41.9) |
| Atherogenic DL | 8 (18.6) |
| CVDPeripheral arterial diseaseCoronary heart diseaseStrokeHeart failureAsymptomatic plaques | 34 (79.1)18 (41.9)15 (34.9)11 (25.6)8 (18.6)2 (4.7) |
CKD: chronic kidney disease; CVD: cardiovascular disease; DL: dyslipidaemia; DM: diabetes mellitus; GFR: glomerular filtration rate; HT: hypertension; uACR: urine albumin-creatinine ratio.
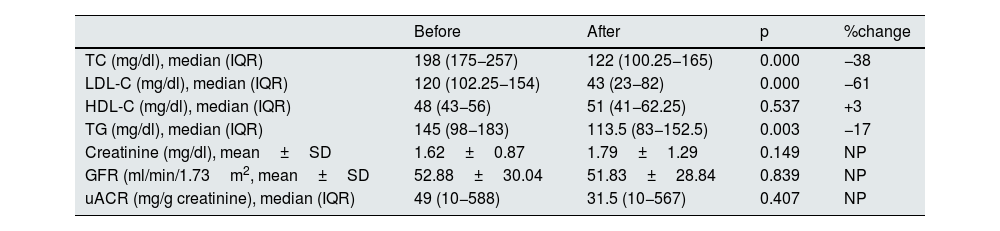
Table 2 shows the lab test results before and after starting PCSK9i. The LDL-C before starting PCSK9i was 120mg/dl (102–154). Treatment with PCSK9i led to significant reductions in total cholesterol (TC), LDL-C and TG, with LDL-C being reduced by 61%. This allowed 59% of the patients to achieve their recommended LDL-C goal. A significant difference in LDL-C reduction achieved with PCSK9i was seen between patients that were previously with or without statins, with a greater reduction in those on statins (66% vs 48%). No significant differences were found in renal function or albuminuria levels.
Lab test results before and after treatment with PCSK9i.
| Before | After | p | %change | |
|---|---|---|---|---|
| TC (mg/dl), median (IQR) | 198 (175−257) | 122 (100.25−165) | 0.000 | −38 |
| LDL-C (mg/dl), median (IQR) | 120 (102.25−154) | 43 (23−82) | 0.000 | −61 |
| HDL-C (mg/dl), median (IQR) | 48 (43−56) | 51 (41−62.25) | 0.537 | +3 |
| TG (mg/dl), median (IQR) | 145 (98−183) | 113.5 (83−152.5) | 0.003 | −17 |
| Creatinine (mg/dl), mean±SD | 1.62±0.87 | 1.79±1.29 | 0.149 | NP |
| GFR (ml/min/1.73m2, mean±SD | 52.88±30.04 | 51.83±28.84 | 0.839 | NP |
| uACR (mg/g creatinine), median (IQR) | 49 (10−588) | 31.5 (10−567) | 0.407 | NP |
GFR, glomerular filtration rate; HDL-C: high-density lipoprotein cholesterol; IQR: interquartile range; LDL-C: low-density lipoprotein cholesterol; NP: not performed; SD: standard deviation; TC: total cholesterol; TG: triglycerides; uACR: urine albumin-creatinine ratio.
This study found a significant reduction in LDL-C, similar to that reported in clinical trials with these drugs, including the renal patients.2,5,6 This has enabled a large percentage of high/very high CVR patients to achieved their LDL-C levels that previously had failed to do so with conventional therapy. Similar real-life studies have been published here in Spain, with comparable results. The RETOSS-NEFRO7 and RETOSS-CARDIO8 studies share the experience of Spanish Cardiology and Nephrology units with evolocumab. The LDL-C reduction in both studies was around 60%, similar to our results. In another study concerning experience in a tertiary hospital,9 reductions of around 55% were achieved. These studies have also shown very good tolerance to the drug, with low discontinuation rates.
Our study analysed the reduction in LDL-C according to whether or not the patient was previously on statins, and found better results in those patients taking a statin. This may show the synergistic effect on metabolic pathways of combination therapies.4
Although this study did not analyse other lipid parameters not commonly used in clinical practice, PCSK9i have been shown to reduce lipoprotein-a — and other atherogenic molecules, and to have an impact on the concentration and size of lipoparticles. This is of particular interest in renal patients, since classic oral lipid-lowering therapy has not shown much benefit in advanced CKD, and one of the reasons could be the lack of efficacy of statins and ezetimibe on lipid parameters not routinely measured or the size of lipoparticles, with these being particularly abnormal in the renal population.10 Given the benefit seen with evolocumab in different stages of CKD,5 future studies are warranted to analyse the impact of PCSK9i on all these lipid parameters and their prognostic impact, especially in the renal population.
FundingNo funding was received for this study.
Conflicts of interestV. Escudero has received lecture fees from Sanofi and Amgen. C. Castro has received lecture fees from Amgen. The other authors have no conflicts of interest to declare.



