
We present the case of a 69-year-old woman, originally from Nicaragua, who attended our centre in December 2015 with a diagnosis of stage 4 chronic kidney disease (CKD) of unknown aetiology. She had a history of well controlled hypertension (HTN) and high cholesterol. She had no history of nephrotoxic drug use or lithiasis.
No known kidney disease in the parents; 5 siblings with hypertension and 3 children without cardiovascular risk factors.
On physical examination, her blood pressure was 135/78, with no oedema. No associated clinical symptoms.
Blood test results: haemoglobin 11.2g/dl; creatinine 2.7mg/dl; CKD-EPI glomerular filtration rate (GFR) 18ml/min/1.73m2. Total cholesterol 170mg/dl and albumin 4.6g/dl.
Weak positive ANA (40.66), positive atypical p-ANCA, negative anti-PR3 and anti-MPO.
Immunofixation in serum with a polyclonal pattern of Igs. Complement fixation normal. Serology for hepatitis B and C, HIV and syphilis negative. Alpha fetoprotein tumour markers, carcinoembryonic antigen, CA-125 and CA 19-9 were negative.
Urine sediment without microhaematuria, and a proteinuria of 0.28g/24h. Renal ultrasound showed symmetrical kidneys of normal size and morphology, good corticomedullary differentiation and no signs of obstructive uropathy.
There was a subsequent deterioration of kidney function (GFR of 15.32ml/m) with no new findings. Given the absence of a clear aetiology of CKD, the decision was to perform a renal biopsy.
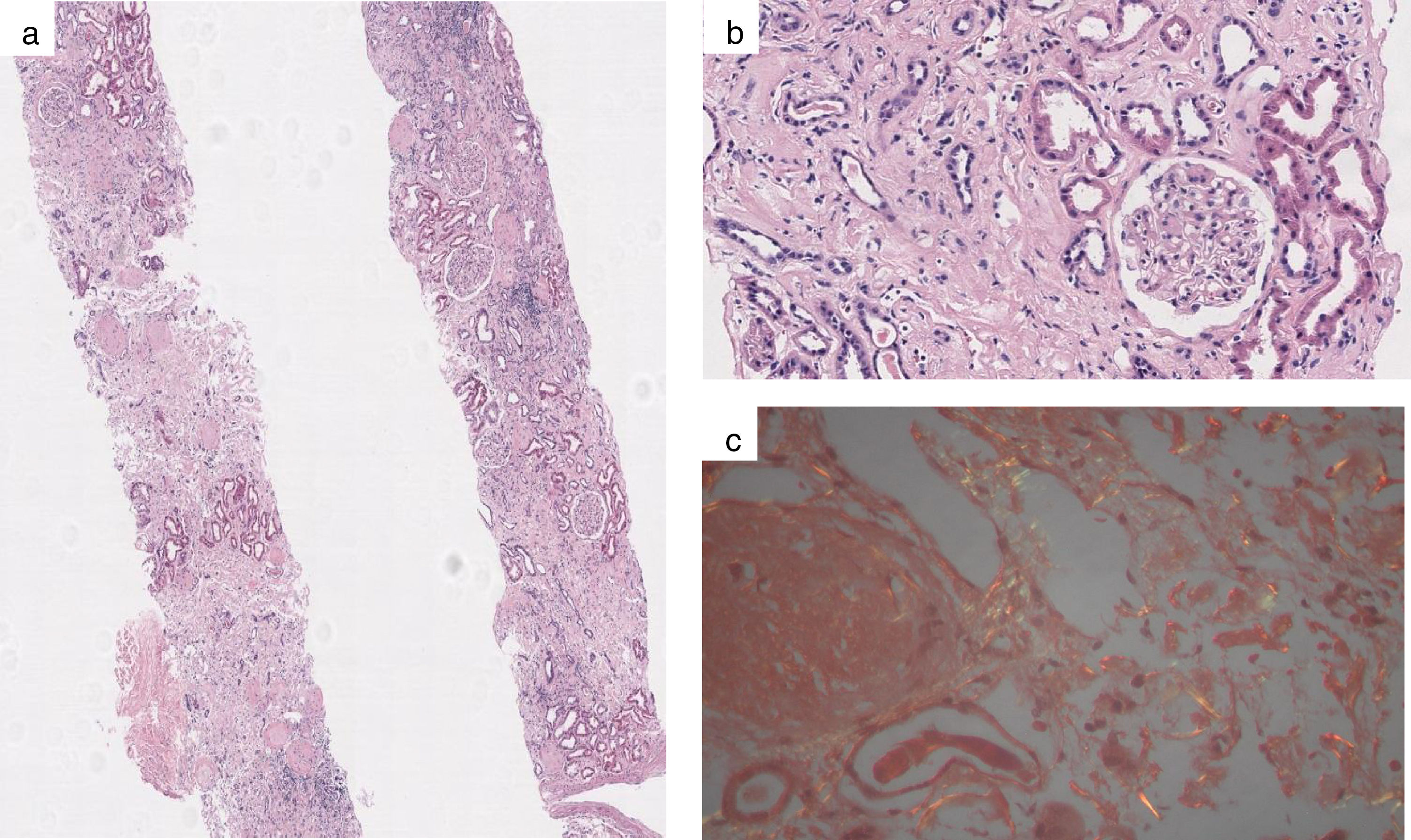
Examination under an optical microscope revealed 29 glomeruli with only 7 preserved (glomerular sclerosis of 75%), with deposits in the mesangium and occasionally in the membrane, visible with H&E staining, with negative Masson's and methenamine silver stains. Major involvement of the cortical interstitium, with foci of chronic inflammation and eosinophils, notably amorphous eosinophilic material, which stained with Congo red and showed apple-green birefringence under polarised light, indicating the presence of amyloid. This occupies the entirety of the interstitium, leading to marked tubular atrophy; it was also observed in the walls of some interstitial vessels and very focally in the glomeruli (Fig. 1).
 View of two renal casts with amorphous hyaline deposits occupying the interstitium (haematoxylin-eosin, ×20); (b) The amorphous hyaline deposits in the glomeruli are markedly fewer than in the interstitium (haematoxylin-eosin, ×200); and (c) Amyloid deposits that turn apple-green under polarised light (Congo red, ×40).")
(a) View of two renal casts with amorphous hyaline deposits occupying the interstitium (haematoxylin-eosin, ×20); (b) The amorphous hyaline deposits in the glomeruli are markedly fewer than in the interstitium (haematoxylin-eosin, ×200); and (c) Amyloid deposits that turn apple-green under polarised light (Congo red, ×40).
Direct immunofluorescence I for gG, IgA, IgM, C3, C4, C1q and fibrinogen was negative in the glomeruli, tubules or vessels.
The immunohistochemical study with amyloid A, kappa and lambda light-chain antibodies was negative.
The absence of expression of these antibodies and uncharacteristic distribution of the amyloid deposits, with marked interstitial but little glomerular involvement, together with the absence of nephrotic syndrome, and in view of the patient's Central American origin, led us to conclude that the most likely diagnosis was ALECT2 renal amyloidosis (RA).
Not having more renal tissue available, it was not possible to immunohistochemically confirm LECT2 or to send a sample for liquid chromatography–mass spectrometry analysis.
With this suspected diagnosis, and since it has been suggested that this disease may be a hereditary amyloidosis with a genetic predisposition, a genetic analysis of the patient, two of her children and her nephew was performed using DNA sequencing.
To find out the genotype of the single-nucleotide polymorphism rs31517 present in the LECT2 gene, a pair of oligonucleotides was designed to sequence a 646-bp DNA fragment, using the following strands: 5′-ATATGGTTATTAGCACCTGCGG-3′ (sense) and 5′-CCCGATAGATATTTTTTTCTGATCC-3′ (antisense).
We thus concluded that the four subjects were homozygotic for the G nucleotide in SNP rs31517, which is characteristic of this disease and confirmed our suspicion.
We present a case of a little-known variety of amyloidosis that has not previously been recorded in Spain; so-called ALECT2 or leucocyte chemotactic factor 2 amyloidosis. First described in 2008 by Benson and James,1 its importance was not realised until 2013, when Said et al.2 described it as the third leading cause of RA in the USA and the most common in the south-eastern region, with clear over-representation in the Hispanic population (88%).
In 2016, Larsen et al. recorded it as the second leading cause of RA in the Egyptian population, indicating that it is probably a common, if little-known, disease in populations around the world.3
Its aetiology is currently unknown. The strong ethnic association and evidence of a hereditary element suggest a genetic aetiology. No mutations in the LECT2 gene have been detected but all patients studied were found to be homozygotic for the G nucleotide in a non-synonymous SNP in position 172. This polymorphism is more common in Mexican lineages and has therefore been associated with Hispanic origins and not with the pathogenesis of the disease, being considered a necessary but insufficient condition to cause the disease.4
ALECT2 is characterised by an atypical presentation compared to other amyloidoses, with late-onset (mean age of 70 years) progressive CKD, with full nephrotic syndrome being rare. Urine sediment is often unremarkable, with proteinuria absent in up to a third of patients and a mean of 0.9g/24h; so frequently the disease is not diagnosed, as renal biopsy, the only method of diagnosis, is not indicated.
Histologically, it predominantly affects the cortical interstitium, in contrast with other forms of amyloidosis.6
There is no specific treatment and a 30% of patients progress to end-stage renal disease. Survival is higher than in other types of amyloidosis due to the absence of cardiac involvement.7
Kidney transplant is a good option, but cases of recurrence of the disease have been reported.5
We consider important to recognise this disease and be included in the differential diagnosis for CKD in routine practice, given the frequency with which it has been reported in recent years.
Please cite this article as: Junco EO, González CS, Pardo RS, Dominguez AL, Sánchez BS, Sainz MS, et al. Amiloidosis derivada del factor quimiotáctico de leucocitos 2 (ALECT2): a propósito de un caso. Nefrologia. 2018;38:558–560.



