
Patients with advanced chronic kidney disease (ACKD) present a wide range of symptoms with a high treatment cost.1 From the initial stages of ACKD, the symptoms are wide-ranging and negatively affect quality of life.1 Uncontrolled symptoms in this population contribute to greater suffering and symptomatic management is a priority.2 The lack of studies conducted in Spain makes it impossible to compare the symptomology between the different treatment groups.
The aim of this study was to describe the prevalence and severity of symptoms in patients with CKD stage 4 and 5 on dialysis and pre-dialysis, and to compare the symptomology in both groups.
In this cross-sectional, observational study, a descriptive analysis was conducted on the prevalence and intensity of symptoms in patients with ACKD, both on dialysis and pre-dialysis. The study data were collected between April and September 2015.
The inclusion criteria were as follows: (1) adult patients with CKD stage 4–5 in pre-dialysis or dialysis for more than 3 months; and (2) Spanish-speaking patients. Patients with cognitive impairment and those under 18 years of age were excluded.
Sociodemographic and clinical data were collected during the interviews, which took place during the ACKD consultation and in the dialysis room. Variables of interest such as symptomology, measured using the modified Spanish version of the Palliative Care Outcome Scale-Symptoms Renal (POS-S Renal), estimated glomerular filtration rate, measured using CKD-EPI, and estimated comorbidity, measured using the modified Charlson comorbidity index (mCCI), are included.3–5
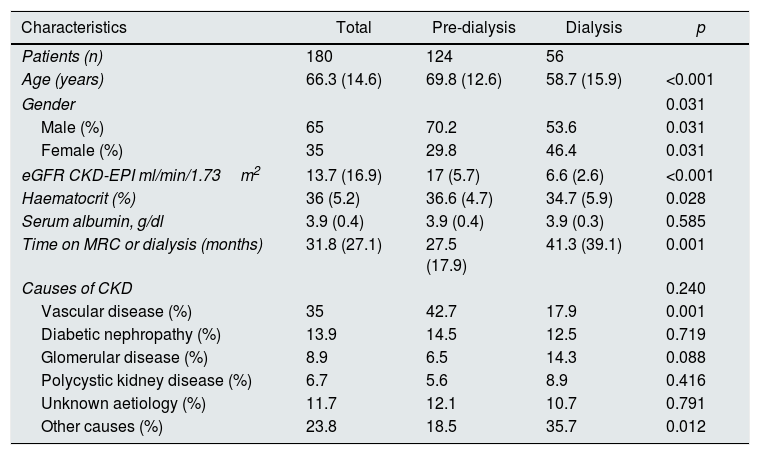
A total of 180 patients with CKD stage 4 and 5 were included in this study, of which 124 patients were on pre-dialysis and 56 were on dialysis (44 haemodialysis and 12 peritoneal dialysis). The results are shown in Table 1. The main comorbidities were: diabetes, ischaemic heart disease, peripheral vascular disease and malignancies.
Sociodemographic and clinical characteristics of the total group and the subgroups.
| Characteristics | Total | Pre-dialysis | Dialysis | p |
|---|---|---|---|---|
| Patients (n) | 180 | 124 | 56 | |
| Age (years) | 66.3 (14.6) | 69.8 (12.6) | 58.7 (15.9) | <0.001 |
| Gender | 0.031 | |||
| Male (%) | 65 | 70.2 | 53.6 | 0.031 |
| Female (%) | 35 | 29.8 | 46.4 | 0.031 |
| eGFR CKD-EPI ml/min/1.73m2 | 13.7 (16.9) | 17 (5.7) | 6.6 (2.6) | <0.001 |
| Haematocrit (%) | 36 (5.2) | 36.6 (4.7) | 34.7 (5.9) | 0.028 |
| Serum albumin, g/dl | 3.9 (0.4) | 3.9 (0.4) | 3.9 (0.3) | 0.585 |
| Time on MRC or dialysis (months) | 31.8 (27.1) | 27.5 (17.9) | 41.3 (39.1) | 0.001 |
| Causes of CKD | 0.240 | |||
| Vascular disease (%) | 35 | 42.7 | 17.9 | 0.001 |
| Diabetic nephropathy (%) | 13.9 | 14.5 | 12.5 | 0.719 |
| Glomerular disease (%) | 8.9 | 6.5 | 14.3 | 0.088 |
| Polycystic kidney disease (%) | 6.7 | 5.6 | 8.9 | 0.416 |
| Unknown aetiology (%) | 11.7 | 12.1 | 10.7 | 0.791 |
| Other causes (%) | 23.8 | 18.5 | 35.7 | 0.012 |
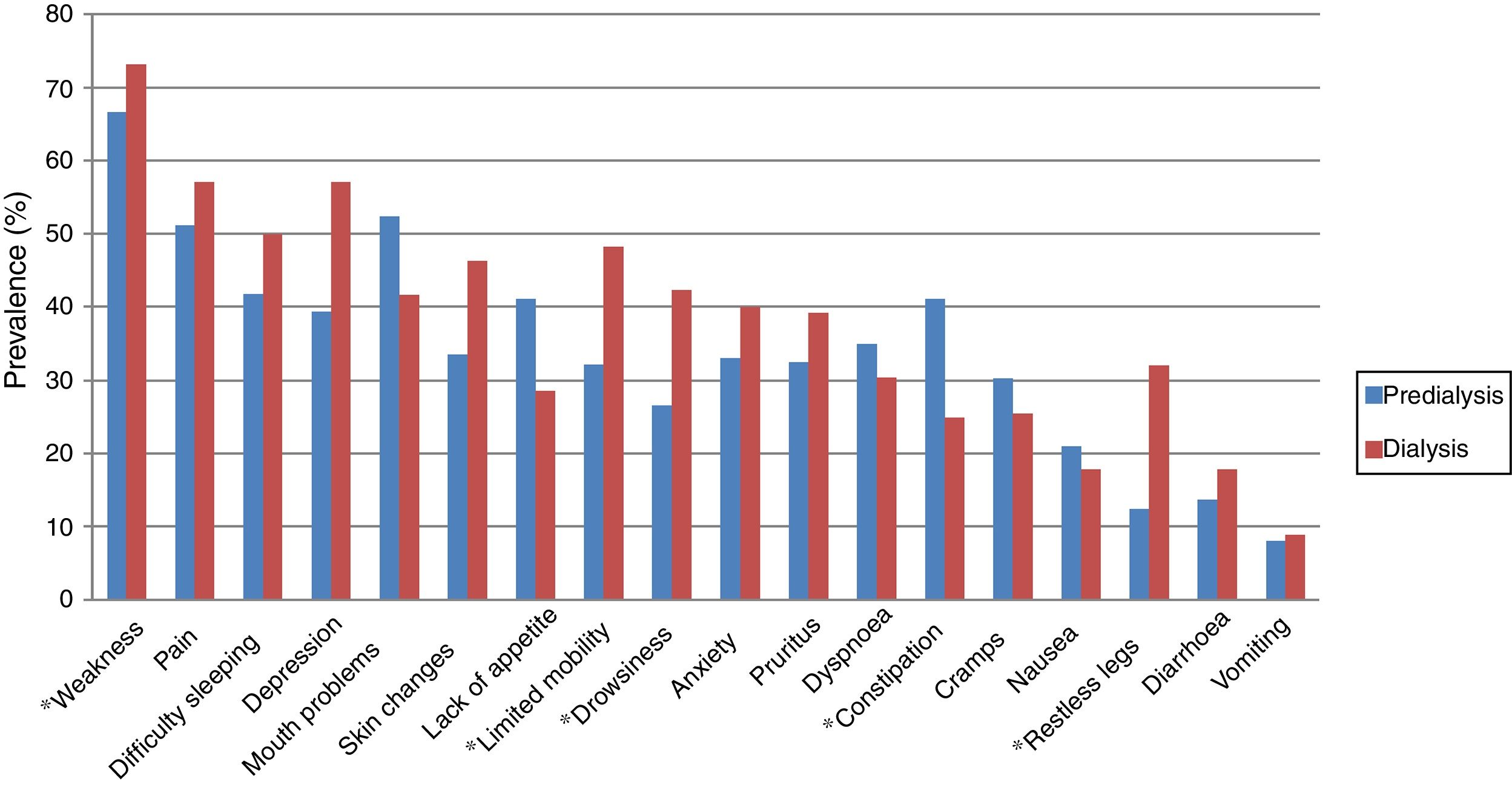
The most common symptoms were: weakness (68.7% [CI: 22–76%]), pain (53.1% [CI: 45–61%]), depression (45% [CI: 36–51%]) and difficulty sleeping (44.4% [CI: 37–53%]). Significant differences were found in the prevalence of symptoms between pre-dialysis and dialysis for weakness (p=0.027), limited mobility (p=0.018), drowsiness (p=0.03), constipation (p=0.015) and restless legs (p<0.01). The comparison of the prevalence of symptoms between pre-dialysis and dialysis is shown in Fig. 1. The most severe symptoms were: weakness (18.8%), pain (14.6%) and pruritus (11.8%).

There are several factors such as kidney failure, associated comorbidity and renal replacement therapy (RRT) that can influence the symptomology in these patients.6
More than 44% of patients presented weakness, pain, depression and difficulty sleeping. These symptoms are consistent in the majority of studies and are associated with a poorer quality of life.1 Symptoms such as weakness, limited mobility, drowsiness, constipation and restless legs presented a significant difference in both groups, being more common in patients on dialysis (except constipation).
Weakness is a very common symptom of ACKD. Various factors, such as sleep disorders, depression, anaemia and RRT can influence the onset of this symptom.1 Weakness was the most prevalent and severe symptom, and was more prevalent in dialysis (p=0.02).
Limited mobility is associated with weakness, comorbidity and RRT. Impaired mobility after starting RRT is associated with short-term mortality in elderly patients.7 In this study, limited mobility was more common in patients with RRT (p=0.01).
Regarding daytime drowsiness, this is associated with other sleep disorders (sleep apnoea, insomnia, and restless leg syndrome), and with symptoms such as weakness and depression.8 Various factors, such as psychological disorders, lifestyle, treatment and comorbidity can influence the onset of this problem.8 The results indicate that daytime drowsiness was more common in patients on dialysis (p=0.03).
Constipation is a common problem in ACKD, and is associated with dietary restrictions, limited mobility and pharmacological treatment.9 This symptom was more prevalent in pre-dialysis patients (p=0.01).
Restless legs syndrome is associated with RRT and other sleep disorders, leading to a reduced quality of life.10 This problem was more common in the dialysis group (p≤0.01).
This study has several limitations. It is a cross-sectional study conducted in a single centre and, therefore, the results cannot be generalised. Furthermore, the pre-dialysis and dialysis groups were not homogenous.
We concluded that patients with ACKD presented a higher symptom burden. In general, there is a similar symptomatic profile in pre-dialysis and dialysis, with weakness being the most common symptom in both groups.
Please cite this article as: Gutiérrez Sánchez D, Leiva-Santos JP, Macías López MJ, Cuesta-Vargas AI. Prevalencia de síntomas en enfermedad renal crónica avanzada. Nefrologia. 2018;38:560–562.



