
We would like to take advantage of World Kidney Day 2017 with the slogan “Obesity and Kidney Disease”, to share epidemiological data from the study into the epidemiology of chronic kidney disease in Spain (EPIRCE).1
It is well known that obesity is a public health problem, and for several years different epidemiological studies have shown a clear relationship between obesity and the risk of developing chronic kidney disease (CKD).2 The associated nephropathy is a result of hyperfiltration, glomerular hypertrophy and increased synthesis of vasoactive and fibrogenic substances and dyslipidaemia.3
The EPIRCE study is an observational study of a randomly-selected multistage sample in 42 sampling points (towns) stratified by habitat, age and gender, providing a representative cohort of the Spanish population (n: 2746). The prevalence of obesity (BMI >30kg/m2) was 26.1% and the odds ratio (OR) of CKD development was 3.5 (95% confidence interval [CI]: 2.0–6.0) while the prevalence of another cardiovascular risk factor, such as arterial hypertension (HTN), was 42% and the OR for CKD development was 6.2 (95% CI: 4.0–9.6).
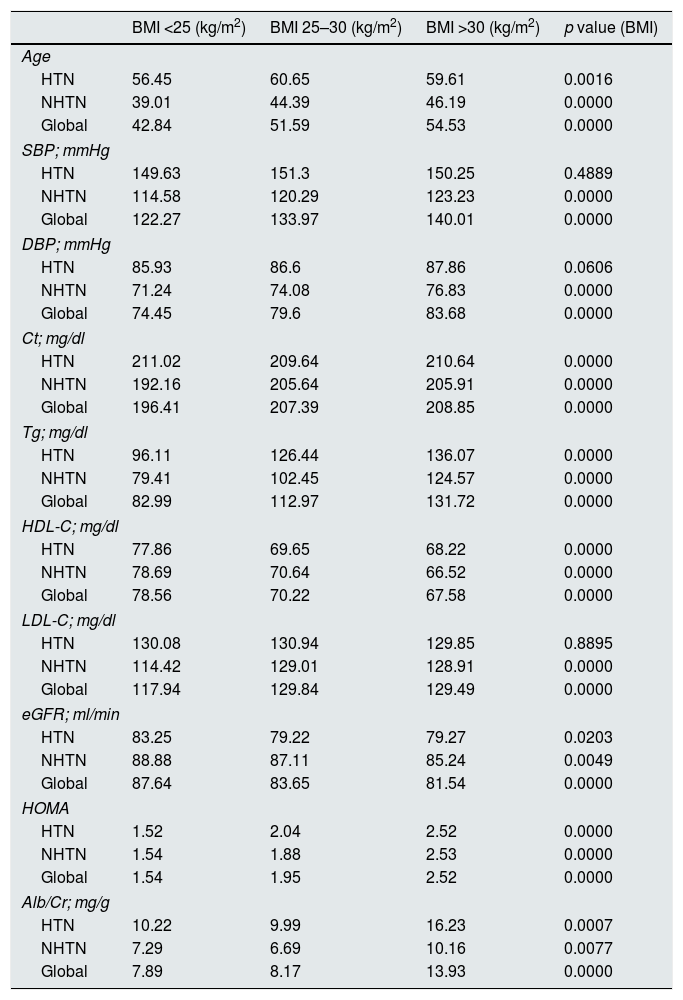
Table 1 shows that the obese population is significantly more hypertensive and dyslipidaemic, with a higher rate of insulin resistance, and the higher BMI is associated with conventional risk factors (HTN, dyslipidaemia, HOMA) and with “worse” kidney function and higher proteinuria rate (Alb/creatinine). However, these changes are also seen in the “global” population, whether they are hypertensive or not.
BMI and cardiovascular risk factors.
| BMI <25 (kg/m2) | BMI 25–30 (kg/m2) | BMI >30 (kg/m2) | p value (BMI) | |
|---|---|---|---|---|
| Age | ||||
| HTN | 56.45 | 60.65 | 59.61 | 0.0016 |
| NHTN | 39.01 | 44.39 | 46.19 | 0.0000 |
| Global | 42.84 | 51.59 | 54.53 | 0.0000 |
| SBP; mmHg | ||||
| HTN | 149.63 | 151.3 | 150.25 | 0.4889 |
| NHTN | 114.58 | 120.29 | 123.23 | 0.0000 |
| Global | 122.27 | 133.97 | 140.01 | 0.0000 |
| DBP; mmHg | ||||
| HTN | 85.93 | 86.6 | 87.86 | 0.0606 |
| NHTN | 71.24 | 74.08 | 76.83 | 0.0000 |
| Global | 74.45 | 79.6 | 83.68 | 0.0000 |
| Ct; mg/dl | ||||
| HTN | 211.02 | 209.64 | 210.64 | 0.0000 |
| NHTN | 192.16 | 205.64 | 205.91 | 0.0000 |
| Global | 196.41 | 207.39 | 208.85 | 0.0000 |
| Tg; mg/dl | ||||
| HTN | 96.11 | 126.44 | 136.07 | 0.0000 |
| NHTN | 79.41 | 102.45 | 124.57 | 0.0000 |
| Global | 82.99 | 112.97 | 131.72 | 0.0000 |
| HDL-C; mg/dl | ||||
| HTN | 77.86 | 69.65 | 68.22 | 0.0000 |
| NHTN | 78.69 | 70.64 | 66.52 | 0.0000 |
| Global | 78.56 | 70.22 | 67.58 | 0.0000 |
| LDL-C; mg/dl | ||||
| HTN | 130.08 | 130.94 | 129.85 | 0.8895 |
| NHTN | 114.42 | 129.01 | 128.91 | 0.0000 |
| Global | 117.94 | 129.84 | 129.49 | 0.0000 |
| eGFR; ml/min | ||||
| HTN | 83.25 | 79.22 | 79.27 | 0.0203 |
| NHTN | 88.88 | 87.11 | 85.24 | 0.0049 |
| Global | 87.64 | 83.65 | 81.54 | 0.0000 |
| HOMA | ||||
| HTN | 1.52 | 2.04 | 2.52 | 0.0000 |
| NHTN | 1.54 | 1.88 | 2.53 | 0.0000 |
| Global | 1.54 | 1.95 | 2.52 | 0.0000 |
| Alb/Cr; mg/g | ||||
| HTN | 10.22 | 9.99 | 16.23 | 0.0007 |
| NHTN | 7.29 | 6.69 | 10.16 | 0.0077 |
| Global | 7.89 | 8.17 | 13.93 | 0.0000 |
Alb/Cr: albumin/creatinine; Ct: total cholesterol; DBP: diastolic blood pressure; eGFR: estimated glomerular filtration rate; Global: general study population; HDL-C: HDL cholesterol; HOMA: homeostatic model assessment; HTN: hypertension; LDL-C: LDL cholesterol; NHTA: normotensive; SBP: systolic blood pressure; Tg: triglycerides.
ANOVA “t” test.
The pathogenic mechanisms of nephropathy seem to be linked to: glomerular hyperfiltration and haemodynamic changes, the dyslipidaemia itself and a greater activation of the renin-angiotensin system, hyperinsulinaemia and a greater synthesis of leptin, oestrogen and TGF-β1.4 Regarding the therapeutic approach it is essentially to lose weight, and the progression of nephropathy is reduced through blood pressure control, improvement of insulin resistance and lipid profile, as well as reduction of leptin and RAAS.4 It should be noted that this association of HTN, obesity, dyslipidaemia or proteinuria is not a metabolic syndrome, a syndrome questioned not only by Reaven5 himself but by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD)6 because the presence of a unique pathogenic substrate has not been proven. Many authors agree that the usefulness of the concept of metabolic syndrome is to highlight the association of multiple CVRFs when making clinical decisions.5 We also consider that CKD is the principal CVRF7 and the existence of a common pathogenic substrate which might explain the coexistence of obesity and CKD.4
Please cite this article as: Otero González A, de Francisco ALM, Gayoso P, López FG. Obesidad y funcion renal .datos del estudio epidemiologico: Prevalencia de la enfermedad renal cronica en España. Estudio EPIRCE. Nefrología. 2018;38:107–108.



