
El primer escalón en la prevención y tratamiento de muchas enfermedades crónicas como las enfermedades cardiovasculares es el seguimiento de una dieta saludable. Varios estudios epidemiológicos han mostrado que el seguimiento de una dieta mediterránea tradicional reduce la mortalidad global, la mortalidad cardiovascular y la incidencia de enfermedades crónicas como las cardiovasculares, el cáncer y las patologías neurodegenerativas. No obstante, un único estudio ha analizado los efectos de la dieta mediterránea en la prevención primaria de la enfermedad cardiovascular, el estudio PREDIMED (PREvención con DIeta MEDiterránea). Este ensayo incluyó 7447 sujetos con alto riesgo vascular que se aleatorizaron a tres grupos de intervención: dieta mediterránea suplementada con aceite de oliva virgen extra, dieta mediterránea suplementada con frutos secos o dieta control (baja en todo tipo de grasa). Los análisis de marcadores intermedios mostraron los efectos beneficiosos de la dieta mediterránea sobre la presión arterial, el perfil lipídico, las partículas de lipoproteínas, los marcadores de oxidación e inflamación y la aterosclerosis carotídea. No obstante, el hallazgo más llamativo fue la reducción del 30 % en el riesgo relativo de sufrir complicaciones cardiovasculares mayores (infarto de miocardio, accidente vascular cerebral y muerte cardiovascular) en ambos grupos de dieta mediterránea, comparados con los que siguieron una dieta baja en grasa. Los resultados del estudio PREDIMED demuestran, pues, que un patrón de alimentación rico en grasa no saturada y productos antioxidantes y antiinflamatorios como la dieta mediterránea resulta ser una herramienta muy útil en la reducción de la mortalidad global y en la prevención de la enfermedad cardiovascular.
The first step in the prevention and treatment of many chronic diseases such as cardiovascular diseases is to follow a healthy diet. Several epidemiological studies have observed that following a traditional Mediterranean diet reduces overall and cardiovascular mortality, as well as the incidence of chronic diseases such as cardiovascular diseases, cancer and neurodegenerative diseases. However, up to now, only one study has analysed the effects of the Mediterranean diet on the primary prevention of cardiovascular disease, the PREDIMED (PREvención con DIeta MEDiterránea) study. This trial included 7447 high vascular risk individuals who were randomly divided into three dietary intervention groups: Mediterranean diet supplemented with extra-virgin olive oil, Mediterranean diet supplemented with nuts, and a control diet (low in all types of fat). Analyses of intermediate markers demonstrated beneficial effects of the Mediterranean diet on blood pressure, lipid profile, lipoprotein particles, oxidative stress and inflammation markers and carotid atherosclerosis. However, the most important finding was the 30% reduction in the relative risk of major cardiovascular complications (heart attack, stroke and cardiovascular mortality) in both Mediterranean diet groups compared to those who followed a low-fat diet. The results of the PREDIMED trial demonstrate that a high unsaturated fat, antioxidant and anti-inflammatory diet plan such as the Mediterranean diet is a useful tool in reducing overall mortality and in preventing cardiovascular disease.
INTRODUCTION
Despite a decrease in cardiovascular mortality in Europe of almost 50% in the last three decades, cardiovascular diseases continue to be the first cause of death in the world, responsible for 42% of deaths in males and 52% of those reported in females1,2. In this context, in accordance with the previsions of the World Health Organization, heart disease and strokes will continue to be the main causes of death in the year 20303. It is therefore a real epidemic, which could be limited with a return to a healthier lifestyle and diet, the Mediterranean diet, for example4. Lifestyle and diet followed in youth and in mid-life stages seem to be the main factors that determine the occurrence of chronic diseases at later stages. For this reason, measures aimed at achieving a healthy diet and lifestyle should be the indispensable ingredients in all forms of prevention and the first step in all treatment of these diseases, as well as a priority in terms of public health for all scientific and health institutions.
Unfortunately, although this seems obvious, the reality is very different, since in clinical practice, a lack of time, but also of conviction by healthcare professionals means that these types of measures and advice are frequently overlooked, postponed or only suggested. As such, for example, the efforts made both by primary care doctors and specialists are usually aimed more at the prescription of “preventive” treatments only based on drugs (hypolipidaemic agents, antihypertensive drugs and others) than education of their patients to correct their bad habits and improve their lifestyle. If we could instil this priority of hygiene and dietary measures over drug treatment, particularly in primary care centres, not only would the short- and long-term drug cost be reduced, but comorbidities and the adverse effects derived from the extensive use of preventive drugs would also be reduced, with the resulting overall benefit for the health of the population5.
DIET PLANS, FOODS AND NUTRIENTS
The dietary recommendations to promote health have been based on diet plans, foods and nutrients that predict the risk of suffering from a chronic disease, particularly a cardiovascular disease6. However, it is currently considered that the ideal approach to studying the effects of diet on health is by analysing diet plans, more than those of certain foods or nutrients, since in the diet the synergic effects of all foods and nutrients converge7. Thus, some studies have shown that the protective effects of certain diet plans on the cardiovascular system are greater than those of foods or nutrients alone8,9. In this regard, a recent systematic review that studied the relationship between causality between dietary factors and heart disease classified the Mediterranean diet as the diet plan that provides the most scientific evidence about its protective effect against cardiovascular disease10. Indeed, many prospective cohort studies have concluded that an increased adherence to a traditional Mediterranean diet is accompanied by a significant reduction in the risk of suffering both cardiovascular complications and death due to any cause4,11. Likewise, many studies have analysed the mechanisms that are probably involved, which adds plausibility to the supposed protective effect of the Mediterranean diet on the cardiovascular system12.
Many epidemiological and dietary intervention studies have analysed the effects of the Mediterranean diet or its main components on intermediate disease markers (blood pressure, lipid profile, oxidative stress markers or pro-inflammatory molecules) as measurements of cardiovascular risk13-18. However, this approach is not fault-free, since overall vascular risk is not limited to the sum of the different known risk factors, not all risk factors have the same induction period or the same potential effect, and there are potentially many other unknown risk factors that may also play an important role in the occurrence or non-occurrence of a cardiovascular complication. Therefore, the recommendations given to certain patient groups, and in particular, society in general should be based on the results of major randomised nutritional intervention clinical trials in which very powerful final variables are assessed (hard-end points), such as heart attack, stroke, cardiovascular mortality and mortality in general. The conclusions obtained in epidemiological studies of large cohorts only have an intermediate level of scientific evidence quality and do not allow us to infer causality, due to the existence of residual confounding factors and/or unknown effects. We therefore require randomised nutritional intervention studies that assess the protective effects of different diet plans on overall mortality and the incidence of the main chronic diseases, such as cardiovascular disease, cancer and neurodegenerative diseases, amongst others.
In this regard, only two clinical trials have been performed to date, the PREDIMED study (PREvención con DIeta MEDiterránea – prevention with Mediterranean diet)19 and the Lyon Diet Heart Study20, which analysed the effects of a Mediterranean diet on the primary and secondary prevention, respectively, of cardiovascular disease. The Lyon Diet Heart Study displayed a marked reduction in cardiovascular complications and mortality in patients who had survived a heart attack and followed a α-Linolenic acid-enriched Mediterranean diet, compared with a control diet20. Likewise, the final results of the PREDIMED study were recently published, in which it was shown that following a Mediterranean diet supplemented with extra virgin olive oil or nuts (walnuts, hazelnuts and almonds) reduces the relative risk of suffering a cardiovascular complication by 30% in asymptomatic patients with a high vascular risk, compared with a diet low in all types of fat21.
TRADITIONAL MEDITERRANEAN DIET PLANS
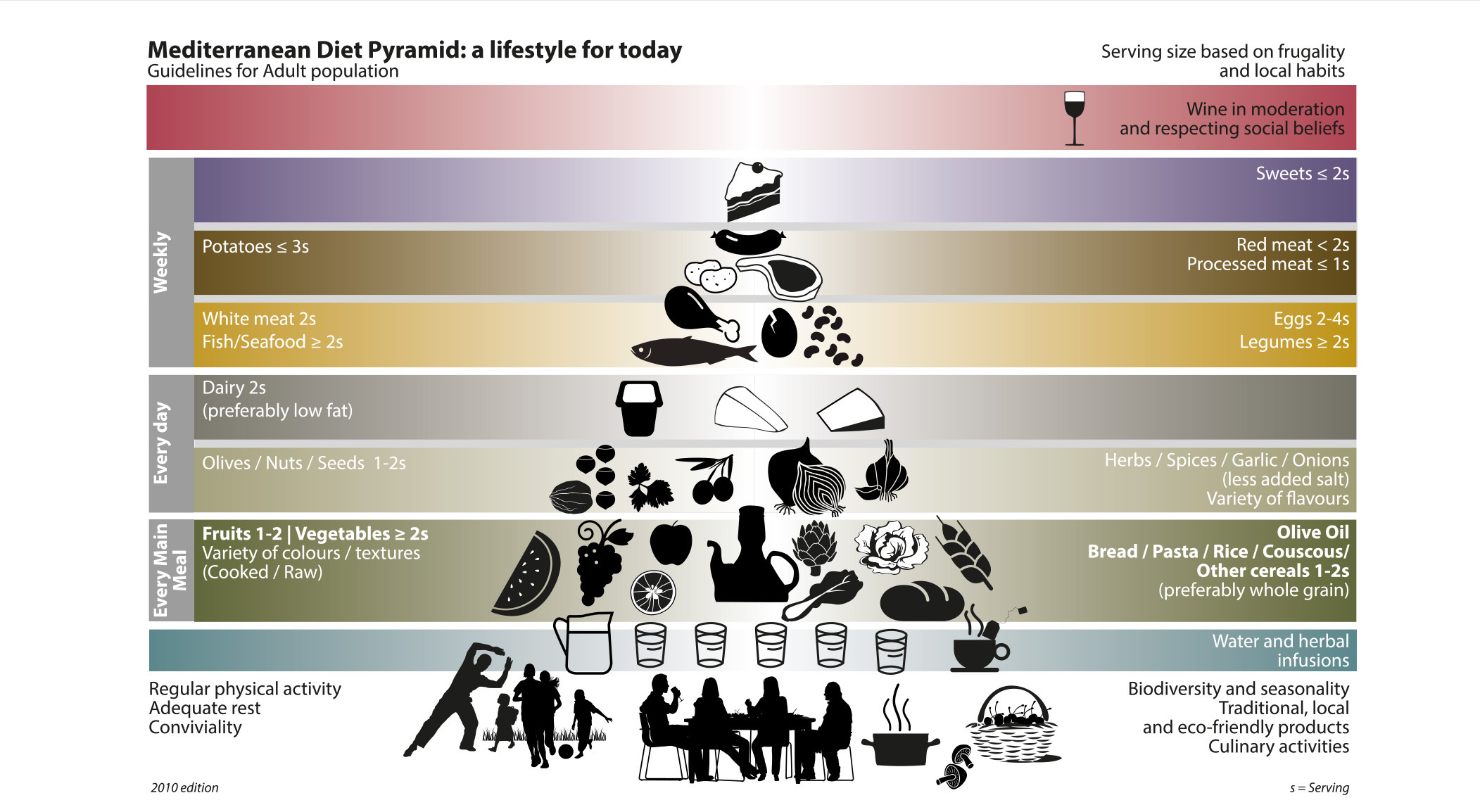
Mediterranean diet is defined as the diet plan of the countries of the Mediterranean region where olives grow (Crete, Greece and the south of Italy and Spain) at the end of the 1950s and the start of the 1960s. Although there is not one single Mediterranean diet, it is considered that its main characteristics are the following: a) high fat consumption (perhaps even more than 40% of total energy), mainly in the form of olive oil (more than 20% of total energy); b) a high consumption of unrefined cereals, fruit, vegetables, pulses and nuts; c) a moderate-high consumption of fish; d) a moderate-low consumption of white meat (poultry and rabbit), dairy products, mainly in the form of yoghurt and fresh cheese; e) low consumption of red meat and products derived from meat; and f) moderate consumption of wine, mainly with meals4. This diet plan and the proportions of the different foods of which it is composed are shown in a “food guide pyramid” that is continually updated (Figure 1). We should highlight that we added other aspects to this food guide pyramid that are related to lifestyle, such as physical exercise, social life and eating with family and friends22.
As mentioned previously in a meta-analysis of observational studies11, after analysing 8 cohorts that included a total of 534,064 subjects, we observed that an increase of 2 points on a 9-point Mediterranean diet adherence scale led to a 10% reduction in the incidence of fatal and non-fatal cardiovascular events. Since the publication of the meta-analysis by Sofi et al.11, the results of seven additional studies were reported, which were included in another meta-analysis using the same criteria as Sofi et al.11, and it was verified that the reduction in relative risk of suffering cardiovascular complications remained at 10% (relative risk 0.90; 95% confidence interval [CI]: 0.86-0.9423.
However, these meta-analyses were based on cohort studies. Randomised intervention studies contribute results of a higher scientific evidence quality. In this regard, we should highlight the French Lyon Diet Heart Study20, which demonstrated an over 50% effectiveness of the Mediterranean diet in the secondary prevention of cardiovascular disease, and the Spanish PREDIMED trial, which showed a 30% effectiveness of the diet in primary prevention.
EFFECTS OF THE MEDITERRANEAN DIET ON MORTALITY AND CARDIOVASCULAR COMPLICATIONS
After the publication of the Lyon study results, it was pointed out that it had some limitations that reduced its usefulness as a basis for future public health recommendations. It was indicated that: a) the conclusions observed are only applicable to secondary prevention, since it analysed the heart attack rate and the rate of heart-related deaths in patients who had already suffered a coronary event; b) the source of fat that was used (linolenic acid administered in the form of canola oil-based margarine) is peculiar and is not marketed or available to the public; c) the control group’s diet was richer in fat than that of the intervention group; d) the sample size was small and as a result, the number of events was relatively low (14 events in one group and 44 in another); and e) the dietary assessment during follow-up was not complete. It was therefore necessary to test another type of intervention with a Mediterranean diet in order to cover this major gap in knowledge.
The PREDIMED clinical trial was designed to demonstrate, using the greatest amount of scientific evidence, the effects of a traditional Mediterranean diet on the primary prevention of cardiovascular disease19,21. In total, 7447 participants were included, of ages ranging between 55 and 80 years (males) or 60 and 80 (females) without clinical manifestations of cardiovascular disease at the time of their inclusion, but with a high likelihood of having them, since they were high vascular risk subjects. Approximately half had diabetes mellitus and the other half had three or more vascular risk factors (smoking, high blood pressure, dyslipidaemia [high cholesterol bound to low-density lipoproteins (LDL) and/or low cholesterol bound to high-density lipoproteins (HDL)], excessive weight or obesity, or a family history of early ischaemic heart disease). These participants were randomly assigned to three dietary intervention groups: a Mediterranean diet supplemented with extra virgin olive oil (2487 participants), a Mediterranean diet supplemented with nuts (2396 participants) or a diet low in all types of fat (2349 participants). All participants were asked to attend an individual and group session with a dietician every three months and they were assessed annually. The study ended at the end of 2011, giving a mean participant follow-up period of six years.
After the baseline visit, all participants were interviewed by a PREDIMED dietician who carried out: a) a simplified assessment of adherence to the traditional Mediterranean diet plan with a 14-point validated scale24; b) the administration of recommendations to follow a Mediterranean diet or a low-fat diet (Guidelines of the American Heart Association and of the National Cholesterol Education Program-Adult Treatment Panel III); c) submission of a leaflet with written recommendations for following the corresponding diet, which included a list of the shopping basket adapted for the season of the year and 14 menus that provided an example of the recommended diet; and d) an individual intervention in accordance with the results of the 14-point questionnaire, in which the participant received personalised advice of the changes that they should make to their diet, aimed at achieving a traditional Mediterranean diet or low fat model. Participants assigned to the Mediterranean diet group supplemented with extra virgin olive oil received an additional leaflet, which contained the benefits for health, use and conservation of the oil, while those assigned to the Mediterranean diet group supplemented with nuts received information about the three types of nuts use in the trial (see www.predimed.org).
In the Mediterranean diet and oil group, the objective was to consume >40g/day of extra virgin olive oil, because this is the mean consumption that has proved to be protective in countries with a low incidence of heart disease25,26. Participants belonging to the Mediterranean diet and nut group received walnuts, hazelnuts and almonds. As we have evidence about the cardioprotective effect of α-Linolenic acid-enriched foods, particularly in walnuts, the contribution of walnuts was higher27. In spite of short-term nutritional trials28 using doses of 50g/day or even more, a mean intake of 30g/day seemed to be more acceptable for long-term consumption for 4-6 years. The added beneficial effects of long-term intake at similar or low doses are probably the origin of protection against ischaemic heart disease that is observed in epidemiological studies29-32.
The participants included in the PREDIMED were assessed annually, and in these assessments, the same measurements were taken and examinations carried out as in the initial visit. The main objective of the study was to assess the effectiveness of the Mediterranean diet on the prevention of a group that included as primary variables cardiovascular mortality, heart attack and stroke. Other variables that were considered to be secondary results (secondary end-points) were the incidence of cancer (breast, bowel, lung and stomach), diabetes and overall mortality. We also assessed the effects on blood pressure, adiposity, glycaemia, lipid profile and systemic markers of cardiovascular disease.
During follow-up, the participants included in both Mediterranean diet groups improved by a mean of almost 2 points in the 14-point scale used, with significant changes in 12 of the 14 points. This increase, with respect to the control group was observed at an early stage (after three months) and was more or less constant throughout the study. However, the main changes were observed in the consumption of extra virgin olive oil, which increased to 50g and 32g per day and in nuts, whose consumption increased to 0.9 and 6 portions (30g per portion) per week in the Mediterranean diet groups supplemented by oil and nuts, respectively. We did not observe any adverse effects related to food in any of the three groups studied.
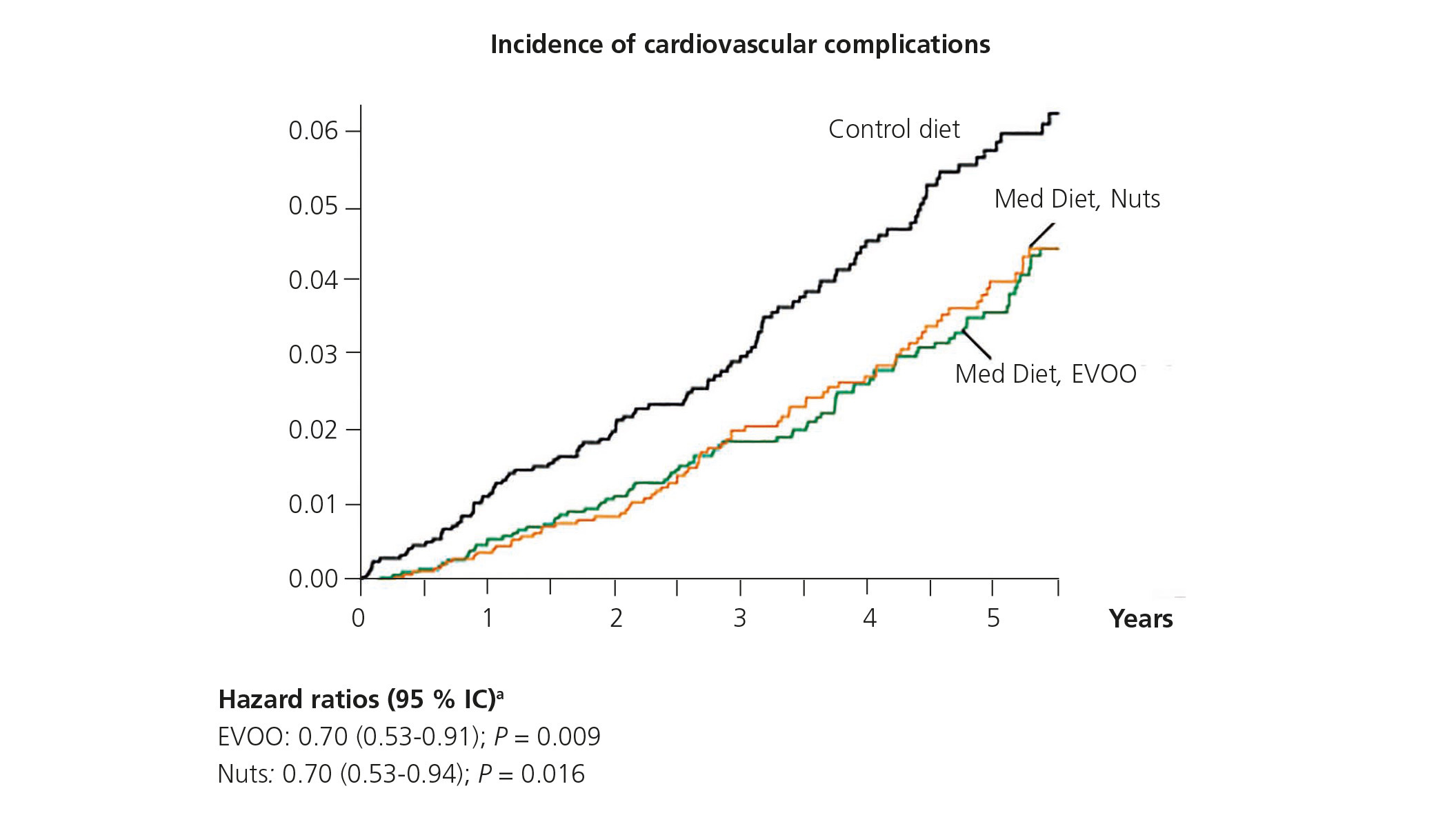
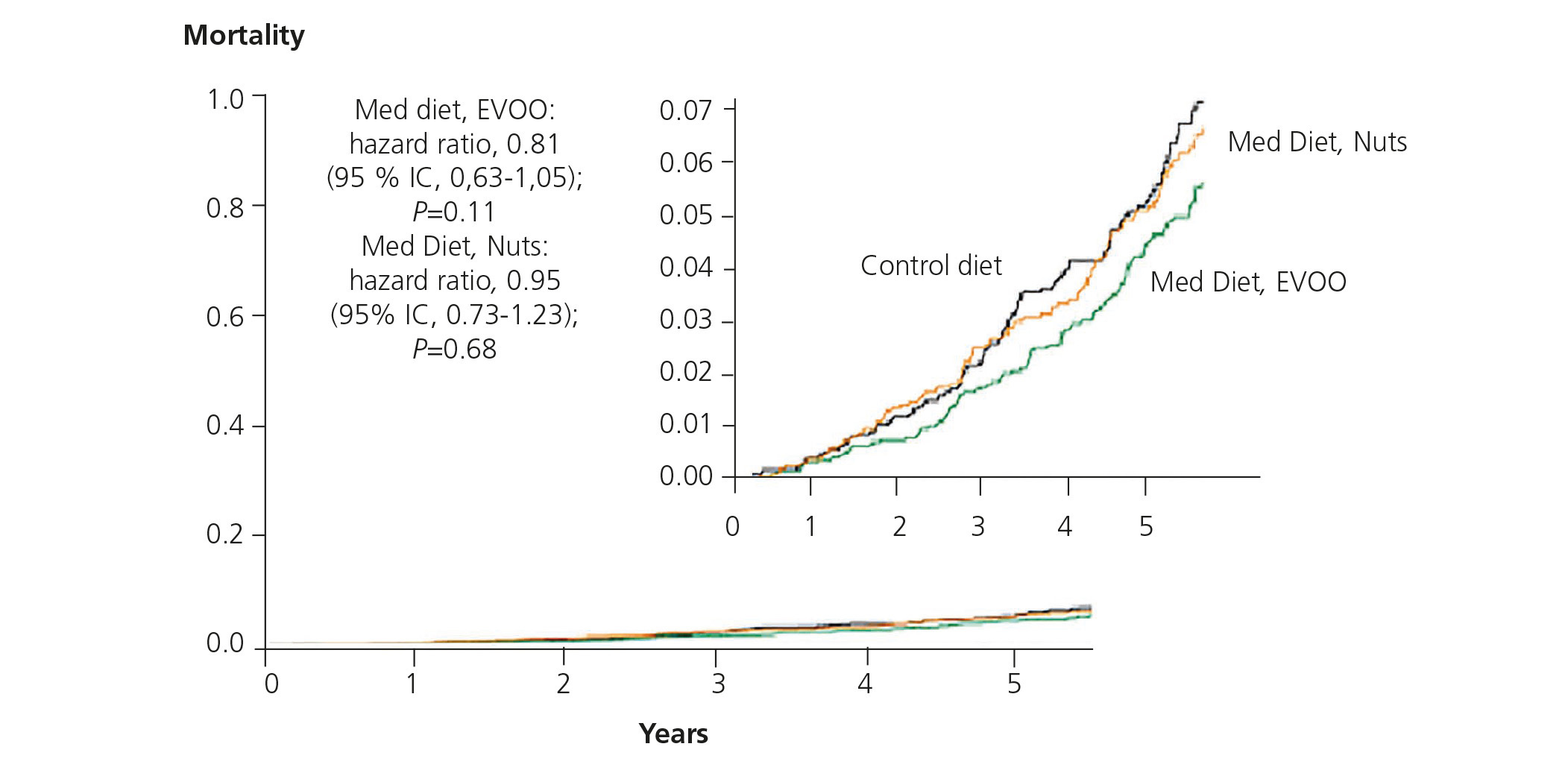
After 4.8 years of follow-up, we detected 288 major cardiovascular complications: 96 in the extra virgin olive oil group (3.8%), 83 in the nut group (3.4%) and 109 in the control group (4.5%)21. The respective primary cardiovascular event rates were 8.1, 8.0 and 11.2 per 1000 people per year-and the respective hazard ratios were 0.70 (0.53-0.91 95% CI) for the extra virgin olive oil group and 0.70 (0.53-0.94 CI) for the nut group (Figure 2). The multivariate analysis showed similar protection for both Mediterranean diet groups with respect to the control diet after adjusting for age, sex, adiposity variables and baseline risk factors. Likewise, these protective effects of the Mediterranean diet did not change in accordance with age (older/younger than 70 years old), sex (male/female), whether the individuals were diabetic (yes/no), had high blood pressure (yes/no), were dislipidaemic (yes/no), were overweight or obese (yes/no), or had a family history of early ischaemic heart disease (yes/no). We observed a reduction in overall mortality in the Mediterranean diet group supplemented with extra virgin olive oil, with a hazard ratio of 0.81 (0.63-1.05 CI; P=.11) with respect to the control group (Figure 3). Therefore, the PREDIMED study demonstrated for the first time with a randomised design that the Mediterranean diet, supplemented with extra virgin olive oil or nuts, is very effective in the primary prevention of cardiovascular disease. In this regard, another important finding is the major reduction in relative risk (>50%) of suffering another cardiovascular complication, peripheral arterial disease, in both Mediterranean diet groups compared with the control group33.
MEDITERRANEAN DIET ACTION MECHANISMS: EFFECTS ON VASCULAR RISK FACTORS
Diabetes mellitus
In the PREDIMED study, we also analysed the effectiveness of the Mediterranean diet on the incidence of new cases of diabetes mellitus, logically in participants who had not been diagnosed with this disease at the start of the trial. Previous studies, both cohort and intervention studies, already showed the effectiveness of the Mediterranean diet on the prevention of diabetes34. Many studies have analysed the role of introducing lifestyle changes aimed at achieving a weight reduction through low-calorie diets along with an increase in physical activity34. However, we did not know what role following a traditional Mediterranean diet without energy restrictions or changes to physical activity could play in the prevention of diabetes. In a preliminary study, it was observed that both intervention groups with Mediterranean diets in the PREDIMED study had around a 50% reduction in the incidence of new cases of diabetes, compared with the control group, after a mean follow-up of four years35. More recently, we analysed the incidence of cases of diabetes in the whole PREDIMED cohort and we detected 273 new cases of diabetes in 3541 participants, 80 in the olive oil group, 92 in the nut group and 101 in the control group. After adjusting for different variables, the hazard ratios for diabetes were 0.60 (0.43-0.85 CI) for the olive oil group and 0.82 (0.61-1.10 CI) for the nut group, compared with the control group36. These results confirm the effectiveness of the Mediterranean diet itself, without other changes in lifestyle, in the prevention of diabetes mellitus.
Other vascular risk factors
In the PREDIMED study, the effects of the Mediterranean diet on other vascular risk factors were also analysed. The results of the first 772 participants included in the study showed that both interventions with a Mediterranean diet reduced blood pressure, improved the lipid profile and decreased circulating inflammatory molecules related to atherosclerosis37. Likewise, it was verified that both Mediterranean diets increased the concentration of large HDL particles and that the Mediterranean diet supplemented with nuts also increased the fraction of less atherogenic LDL cholesterol particles38. In another study with the whole PREDIMED cohort and after a mean follow-up of four years, we observed that introducing a Mediterranean diet reduced diastolic blood pressure, but not systolic blood pressure, compared with the control diet39. We should highlight that these effects were observed without significant changes being noted either after three months37 or after one year of follow-up40.
While traditional risk factors play a critical role in the development of atherosclerosis, the mechanisms related to these risk factors and cardiovascular disease itself include endothelial dysfunction, inflammation, oxidative stress and genetic factors, amongst others. A high plasma concentration of LDL cholesterol is a powerful atherogenic factor, but oxidised LDL particles are critical in the onset and progression of atherosclerosis. In the PREDIMED study, we also observed a reduction in circulating oxidised LDL particles in the two Mediterranean diet groups after three months of intervention41. Inflammation also plays a major role in the pathogeny of many chronic diseases, including cardiovascular diseases. The reduction in circulating inflammatory molecules both in serum and in cells observed after three months of intervention37 and after one year42,43 confirms the reduction in the expression of pro-atherosclerotic genes related to vascular inflammation44.
A PREDIMED sub-study confirmed that participants with a high intima-media thickness included in both Mediterranean diet groups had a reduction in the thickness of this layer, which would imply a regression of atherosclerotic lesions45. In a subsequent study, it was confirmed that the group that followed the Mediterranean diet supplemented with nuts also had a regression of atheromatous plaques, and those who followed a Mediterranean diet supplemented with extra virgin olive oil had a delayed progression of lesions, compared with the control group46. Although the mechanisms involved in this protection are not well-known, these effects are attributed to the anti-oxidant and anti-inflammatory effects of the Mediterranean diet47. Indeed, as mentioned previously, nutrigenomics studies conducted reveal that the Mediterranean diet would reduce the expression of pro-atherogenic genes related to inflammation, the formation of foam cells and thrombosis44. In other words, the protective effects of the Mediterranean diet on the cardiovascular system are at least partly due to their action on classic and emerging factors of vascular risk, as well as their nutrigenomic pro-atherogenic gene inhibition effects and the promotion of anti-atherogenic gene expression.
In the PREDIMED study, we also analysed whether the protective effects of the Mediterranean diet or its components differed according to the genome of each participant in order to verify the effects of different genetic variables on intermediate phenotypes (blood pressure, lipids, etc.) and their interaction with diet, as well as the effects of these interactions on the final phenotypes (mainly cardiovascular disease and cancer).
Cyclooxygenase-2 (COX-2) and interleukin-6 (IL-6) are two important genes related to inflammation. In the PREDIMED study, we verified that the COX-2-765G>C polymorphism is associated with lower serum concentrations of IL-6 and ICAM-1 (intercellular adhesion molecule-1) in carriers of the variant allele and the IL-6-174G>C polymorphism (CC carriers versus G) was associated with greater concentrations of ICAM-1. However, we did not observe any gene-diet interaction after the intervention. As such, the Mediterranean diet decreased inflammatory markers in all participants, independently of their genotype. In other words, the anti-inflammatory effect was related more to the degree of adherence to the diet than to the genotype characteristics of the participants48. Lastly, we should highlight that the Mediterranean diet has been useful for reducing the genetic risk of suffering from certain diseases, in this case, a stroke49. In the PREDIMED study, we analysed the gene of transcription factor 7-like 2 (TCF7L2), which is strongly associated with diabetes and we observed that the intervention with both Mediterranean diets cancelled the adverse effect of the TCF7L2 polymorphism rs7903146 (C>T) on vascular risk factors (glucose and lipids) and, most importantly, on stroke incidence.
CONCLUSIONS
For the first time, the PREDIMED study has demonstrated that the traditional Mediterranean diet prolongs life and exercises a powerful protective effect against the occurrence and development of cardiovascular disease and has confirmed the beneficial effects of this diet plan on the main vascular risk factors, both classic and emerging factors. We should highlight that the Mediterranean diet exercises this protective effect independently of age, sex and vascular risk factors and that it is particularly effective in individuals who are genetically predisposed to suffering from cardiovascular disease. Its protective effects are of a similar magnitude to that observed in statins, for example, but without the secondary effects that these drugs often cause. Therefore, it is never too late to change our eating habits and have a more healthy diet, such as the traditional Mediterranean diet. However, this diet could even be improved if we changed regular olive oil to extra virgin olive oil, if we increased nut, oily fish, vegetable and pulse consumption, if we replaced bread and refined cereals with wholemeal equivalents, if we maintained a moderate consumption of wine with meals, if we reduced salt and meat, particularly red meat consumption and if we avoided intake of sweet drinks, cakes and confectionery 50.
Conflicts of interest
The author declares potential conflicts of interest. Grants: Instituto de Salud Carlos III, Ministry of the Economy and Competitiveness. Lecture fees: Spanish Transplantation Society, Laboratorios Lilly. Instituto Cervantes. Consultancy fees: FIVIN – Wine and Nutrition Research Foundation, Beer and Health Foundation. He is a member of the following boards: ERAB-European Research on Alcoholism, FIVIN- Wine and Nutrition Research Foundation, Beer and Health Foundation. He receives travel grants or travel expenses: Harvard University, Boston, United States.

Figure 1. Mediterranean diet pyramid created by the Meditarranean Diet Foundation of Barcelona (2010) (Source: Mediterranean Diet Foundation, www.dfmed.org)22.

Figure 2. Incidence of cardiovascular complications in the 7447 participants in the PREDIMED study according to an analysis of Kaplan-Meier estimates.

Figure 3. Overall mortality in the 7447 participants of the PREDIMED study according to an analysis of Kaplan-Meier estimates.



